
Maria Abdul Karim1, Hufsa Tariq2*, Hafiz Muhammed Asim3
1Lahore College of Physical therapy, Lahore Medical &Dental College, Pakistan![]()
2*Lecturer Lahore College of Physical therapy, Lahore Medical &Dental College, Pakistan![]()
3Associate Professor Lahore College of Physical therapy, Lahore Medical &Dental College, Pakistan![]()
ABSTRACT
Background of the Study: To assess the functional outcome among patients with arthroscopic ACL reconstruction with endo-button at Ghurki Trust Teaching Hospital post 6 months.
Methodology: A single centered survey was conducted on 67 patients with arthroscopic AC Ligament reconstruction using Hamstring auto-graft (Semitendinosus-Gracilis tendons) after 6 months and evaluated for functional outcome. The data was collected from Ghurki Trust Teaching Hospital. The sampling procedure utilized was non-probability sampling. Functional outcome was assessed using subjective form of IKDC score. Data was analyzed using SPSS version 23.
Results: Out of 67 patients, all were male. The pre-operative subjective IKDC scoring was less than 30 and post-operative mean IKDC scoring is 73.92. On the basis of findings of study, significant improvement was observed after ACL reconstruction post 6 months.
Conclusion: ACL reconstruction shows significant improvement in knee function and significant recovery of preoperative functional status.
Keywords: Anterior cruciate ligament reconstruction, international knee documentation score, functional outcome, arthroscopy, endobutton, hamstring tendon, ligament injury.

Introduction
AC Ligament considered as passive primary restraint against anterior tibial translation on femur ACL gives rotational stability in both planes frontal and transverse1,3. AC ligament is most commonly injured ligament in knee joint. The most common mechanism of injury is non-contact and the involved forces are valgus and internal rotation4. ACL injuries are particularly common in sports (basketball, soccer, and skiing) due to motions that require a lot of deceleration (pivoting, jumping, abrupt stops, and changing directions quickly)5,6,7,2. The annual incidence for ACL injuries are at least 0.8 per 1000 persons between 10 -64 years of age. In all Knee injuries, approximately 25% are ACL injuries8. ACL rupture results in increase the risk of early performance degenerative changes in joint, subsequent injury to meniscus, with athletic difficulty9,2. Since majority non-operative managements and procedures gives functional outcome which are not acceptable26. In ACL injuries, treatment choice is ACL reconstruction. For knee with deficit ACL, the treatment choice remains arthroscopic assisted ACL reconstruction10. Because it is anatomically more correct, successful and morbidity rate associated with this procedure is low11.The tendons of Semitendinosus and Gracilis (STG) become the method of choice in ACL reconstruction. For STG tendons graft, widely use device is femoral fixation Endo-Button (Smith and Nephew) system12 because it appeared as sufficiently resistant, rigid and reliable13. Surgical technique of Endo-button reduces the potential risk of interference screw fixation. This technique reduces the need for second incision, also adjustable to a range of graft materials (allograft or auto graft BPTG and hamstring). Because of its easy use and early fixation strength, many of surgeons favor this fixation device. Functional outcome are defined as ability of a patient to perform activities of daily living as result of any health care services14. Functional outcomes reported by patients such as quality of life related to health and disability help to make a difference between the varieties of treatments effectiveness and helps to choose the best possible treatment for patient. Individual recovery is the area of focus in functional outcome especially in vocational areas and social functioning rather than on symptom resolution15. AC Ligament reconstruction goals are to help the patient with ACL deficient knee to gets functionally stable joint, symptoms free and possible recovery of activity that present before injury7,5. Sustained ACL injury substantially increases the future risk of early degenerative changes in the knee joint in young people and adolescents demonstrated by different researches16. Methods of reconstruction are also influenced the rehabilitation. Arthroscopic assisted ACL reconstruction allows the early weight bearing but open ACL reconstruction requires long period of post immobilization. Assessment of functional outcomes is done by subjective form of International knee documentation score (IKDC). Subjective IKDC is patient oriented questionnaire and utilized for evaluation of functions, symptoms in activities of daily living in people with different type of knee disorders (Meniscal, patellofemoral dysfunction, ligamentous and osteoarthritis). It has 18 items and possible score range 0–100, where increasing score indicate less limitation in activities of daily living, sports and more symptoms absence17. The goal of ACL Rehabilitation (ACLR) programs is to track patients’ improvement in terms of muscular strength, bilateral and unilateral balance, coordination, range of motion, and overall mobility24. The rehabilitation period is strictly dependent on individuals. In general, patients can resume regular everyday activities after 2-3 months (short-term rehab), while a longer period of 6 to 9 months allows for a return to sport (long-term rehab)25. The objective of this study was to assess the functional outcome among patients with ACL reconstruction in Ghurki Hospital post 6 months. The rationale was to provide a window of opportunity to design and incorporate a well-planned, individualized rehabilitation plan according to patient needs and demands.
Methodology
A Case series type of Descriptive study was performed at Ghurki Trust and Teaching Hospital, GTTH for a period of Six months from April 2019 to October 2019. About sample size of 67 patients are taken by using the WHO sample size calculator considering values such as 17% prevalence (P) (18), 95% confidence interval (1-α) and 0.09 precision (d). Participants aged above 16 with arthroscopic AC Ligament reconstruction using hamstring autograft (Semitendinosus-Gracilis tendons) with Endo-button femoral fixation post 6 months, who had preoperative subjective IKDC score less than 30 were included in study. Participants with history of infection, operation on either knee previously, other concurrent fracture, PCL, collaterals ligament injury and meniscus injury were excluded from this study. Patients were evaluated for functional outcome using subjective form of IKDC score. A prior consent was taken from participants. Data entry and statistical analysis was done by SPSS version 23. The study variables were presented in the form of descriptive statistics. Ethical permission was taken from the Committee of ethics at LCPT. Questionnaire in form of information sheet that briefly describe the aims and it also included the consent sheet and assure the participants that their responses will be kept confidential. The IKDC Subjective Knee Form was divided into three sections: symptoms including swelling, pain, stiffness, giving way, and locking, sports, current knee function and knee function after knee injury (not included in the total score)1. Number of items of IKDC, 18 (7 items for symptoms, 1 item for sport activity, 9 items for daily activities, and 1 item for current knee function)22. Both inter- and intra-observer reliability were highest for IKDC (0.79 and 0.86 respectively)23.
Results
About 67 participants took part in this study and all were male. When both right and left sides were compared the results showed 2.77:1. About 50 patients (74.6%) and 18 (26.86%) had right and left sided injury respectively as mention in Table 1. When looked on the mode of injury, majority of participants about 36 (52.94%), injury mode were RTA, sports injury 17 (25%) participants and 15 (22.05%) participant’s injury mode were others like falls as mention in Table 1. Participants of 17 to 60 years age range were included in study with mean age 28.46 years as mention in Table 1.

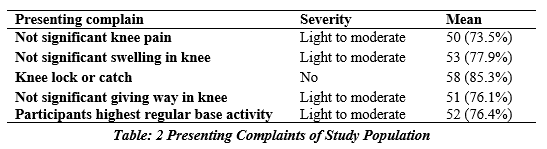
Majority of patients about 50 (73.5%) and 53 (77.9%) can perform light to moderate activities without significant knee pain and swelling in knee respectively as mention in Table 2. About 58 (85.3%) patients had no complaint of knee lock and catch and 51 (76.1%) can perform light to moderate activities without significant giving way in knee as mention in Table 2. Most of study population about 52 (76.4%) can participate in light to moderate activities on regular basis which shows why majority of patients can perform light to moderate activities without any problem in knee after ACL reconstruction because their regular activities are in light to moderate category before injury.
After ACL reconstruction, majority of study population had minimally to moderate difficulty in kneeling on front of knee, squatting, sit with knee bent, jump and land on involved leg and stop and start quickly. The study population (n=67) had pre-operative subjective IKDC score less than 30 with mean 25 and mean post-operative subjective IKDC score was 73.92 which showed improvement in patient function after ACL reconstruction (Table 3).
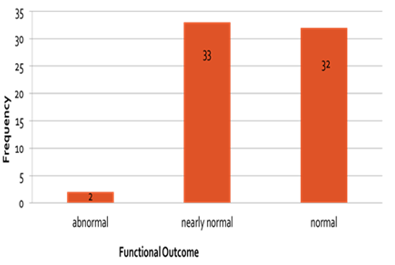
According to grading system of IKDC out of 67 sample size, 32 patients were in Grade A (Normal), 33 patients in Grade B (Nearly Normal), 2 patients in Grade C (Abnormal).
Discussion
Improvements in research and advancements in arthroscopy techniques make the ACL reconstruction a successful procedure. In current study, mean IKDC score is 73.92 compare with pre-operative subjective IKDC score was less than 30 concluded that functional outcome after reconstruction was improved. This research results are close to those of previous researches. The previous study (19) results show that mean pre-operative IKDC scoring was 42.45 and mean post-operative IKDC score was 81.87, which showed significant improvement after Arthroscopically assisted AC ligament reconstruction. ACL reconstruction offers a significant improvement in knee function and complications are minimal with significant recovery of preoperative functional status. In comparison, current study is somewhat similar to19, both shows the significant improvement in functional outcome after reconstruction. But differences in value of IKDC scores, because in current study pre-operative IKDC score is low less than 30 as compare with19 pre-operative IKDC score which is high 42.45.In another study20, results show that in about 30 patients, 80% patients in Grade A, 16.6% in Grade B and 3.33% in Grade C, according to IKDC grading system. The majority of patients showed two grades improvement in outcomes. In comparison, current study results are somewhat similar with20 study, it shows that out of 67 patients, 49% in Grade A, 48% in Grade B, 2.9% in Grade C. Both studies results show the improvement in functional outcome.
In another previous study13, the results indicate that endobutton fixation device show no complications. On IKDC score, 92.4% patients are in A& B normal and nearly normal and 7.8% were in grade C and D abnormal and severely abnormal. The Endobutton fixation device for graft in femoral tunnel is providing good mechanical stability. In comparison, current study results are somewhat similar with13 study, in current study 97% patients are in grade A and B and 3% are in grade C. In this study, mean subjective IKDC score of 73.92 are somewhat similar with19 81.87 and21 86.4.
Conclusion
ACL reconstruction with endobutton shows improvement in knee function and recovery of preoperative functional status.
AUTHORS’ CONTRIBUTION:
The following authors have made substantial contributions to the manuscript as under:
Conception or Design: Maria Abdul Karim
Acquisition, Analysis or Interpretation of Data: Maria Abdul Karim, Hufsa Tariq
Manuscript Writing & Approval: Hafiz Muhammed Asim
All authors acknowledge their accountability for all facets of the research, ensuring that any concerns regarding the accuracy or integrity of the work are duly investigated and resolved.
ACKNOWLEDGEMENTS: We acknowledge Lahore College of physical therapy and Ghurki hospital, Lahore, Pakistan for helping us accomplish the study objectives.
INFORMED CONSENT: Prior to survey, patients were informed and written consent was obtained by participants.
CONFLICT OF INTEREST: None
FUNDING STATEMENTS: None
ETHICS STATEMENTS: The study conduct was approved by the Lahore College of Physical Therapy research committee.
References
- Heusdens CH, Hopper GP, Dossche L, Roelant E, Mackay GM. Anterior cruciate ligament repair with Independent Suture Tape Reinforcement: a case series with 2-year follow-up. Knee Surgery, Sports Traumatology, Arthroscopy 2019 Jan; 27(1):60-7.
- Dong Z, Niu Y, Qi J, Song Y, Wang F. Long term results after double and single bundle ACL reconstruction: Is there any difference? A meta-analysis of randomized controlled trials. Acta orthopaedica et traumatologica turcica 2019;53(2):92-9.
- Mishra AK, Girish S. A prospective study of functional outcome of ACL reconstruction with quadrupled semitendinosus tendon autograft using Endobutton and bioabsorbable interference screw. International Journal of Orthopaedics 2018;4(3):47-55.
- Bates NA, McPherson AL, Rao MB, Myer GD, Hewett TE. Characteristics of inpatient anterior cruciate ligament reconstructions and concomitant injuries. Knee Surgery, Sports Traumatology, Arthroscopy 2016;24(9):2778-86.
- Xie X, Xiao Z, Li Q, Zhu B, Chen J, Chen H, Yang F, Chen Y, Lai Q, Liu X. Increased incidence of osteoarthritis of knee joint after ACL reconstruction with bone–patellar tendon–bone autografts than hamstring autografts: a meta-analysis of 1,443 patients at a minimum of 5 years. European Journal of Orthopaedic Surgery & Traumatology 2015 Jan;25(1):149-59.
- Domnick C, Raschke MJ, Herbort M. Biomechanics of the anterior cruciate ligament: Physiology, rupture and reconstruction techniques. World journal of orthopedics 2016;7(2):82.
- Bin SI. Have evolving surgical methods improved clinical outcomes after anterior cruciate ligament reconstruction. Knee Surgery & Related Research 2017 Mar;29(1):1.
- Bigoni M, Turati M, Gandolla M, Sacerdote P, Piatti M, Castelnuovo A, Franchi S, Gorla M, Munegato D, Gaddi D, Pedrocchi A. Effects of ACL reconstructive surgery on temporal variations of cytokine levels in synovial fluid. Mediators of Inflammation 2016 Oct;2016.
- Paschos NK. Anterior cruciate ligament reconstruction and knee osteoarthritis. World journal of orthopedics 2017;8(3):212.
- Hurley ET, Calvo-Gurry M, Withers D, Farrington SK, Moran R, Moran CJ. Quadriceps tendon autograft in anterior cruciate ligament reconstruction: a systematic review. Arthroscopy: The Journal of Arthroscopic & Related Surgery 2018 May 1;34(5):1690-8
- Al Hulaibi F, Al Eid Z, Altaher S, Albarrak A, Alzaid Z. Kneeling assessment after Anterior Cruciate ligament reconstruction using Bone-Patellar Tendon-Bone autograft versus hamstring autograft.
- Saygi B, Karaman O, Sirin E, Arslan I, Demir AI, Oztermeli A. Comparison of different femoral fixation implants and fit techniques for tunnel widening and clinical outcome in ACL reconstruction using hamstring autograft. Archives of orthopaedic and trauma surgery 2016 Feb;136(2):241-7.
- Gabler CM, Jacobs CA, Howard JS, Mattacola CG, Johnson DL. Comparison of graft failure rate between autografts placed via an anatomic anterior cruciate ligament reconstruction technique: a systematic review, meta-analysis, and meta-regression. The American journal of sports medicine 2016;44(4):1069-79.
- Grimshaw SL, Taylor NF, Mechinaud F, Shields N. Assessment of physical function in children with cancer: A systematic review. Pediatric blood & cancer 2018;65(12):e27369.
- Sonesson S, Kvist J, Ardern C, Österberg A, Silbernagel KG. Psychological factors are important to return to pre-injury sport activity after anterior cruciate ligament reconstruction: expect and motivate to satisfy. Knee surgery, sports traumatology, arthroscopy 2017;25(5):1375-84.
- Simon D, Mascarenhas R, Saltzman BM, Rollins M, Bach BR, MacDonald P. The relationship between anterior cruciate ligament injury and osteoarthritis of the knee. Advances in orthopedics 2015;2015.
- Collins NJ, Misra D, Felson DT, Crossley KM, Roos EM. Measures of knee function: international knee documentation committee (IKDC) subjective knee evaluation form, knee injury and osteoarthritis outcome score (KOOS), knee injury and osteoarthritis outcome score physical function short form (KOOS‐PS), knee outcome survey activities of daily living scale (KOS‐ADL), Lysholm Knee Scoring Scale, Oxford Knee Score (OKS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), Activity Rating Scale (ARS), and Tegner Activity Score (TAS). Arthritis care & research 2011;63(S11):S208-28.
- Shah F, Riaz MU, Hassan D, Abbas Z. Factors contributing anterior cruciate ligament injury and pattern of presentations 2017.
- Veeragandham P, Raghavan V, Chattopadhyay A, Banerjee U, Kothari S. Functional outcome following arthroscopic ACL reconstruction using semitendinosus graft: a prospective observational study. International Journal of Research in Orthopaedics 2017;3(3):423.
- Robindro P, Latchumi NV, Kanthimathi BD. To study the functional outcome of arthroscopic ACL reconstruction using hamstring graft fixed with endobutton for femur and interference screw and suture post for tibial fixation. International Journal of Medical and Dental Sciences 2016;5(1):978-83.
- Devgan A, Magu N, Siwach R, Rohilla R, Sangwan S. Functional outcome in athletes at five years of arthroscopic anterior cruciate ligament reconstruction. ISRN orthopedics 2011;2011.
- Ahmed KM, Said HG, Ramadan EK, Abd El-Radi M, El-Assal MA. Arabic translation and validation of three knee scores, Lysholm knee score (LKS), Oxford knee score (OKS), and International Knee Documentation Committee Subjective Knee Form (IKDC). Sicot-j 2019;5.
- Eckersley T, Faulkner J, Al-Dadah O. Inter-and intra-observer reliability of radiological grading systems for knee osteoarthritis. Skeletal Radiology 2021:1-0.
- DiFabio M, Slater LV, Norte G, Goetschius J, Hart JM, Hertel J. Relationships of functional tests following ACL reconstruction: exploratory factor analyses of the lower extremity assessment protocol. Journal of sport rehabilitation 2018;27(2):144-50.
- Bottone S, Demarchi D, Tedesco S. Acl rehabilitation: An inertial sensors-based approach for functional assessment and progress monitoring. Ph. D. dissertation 2018.
- Moksnes H, Risberg MA. Performance‐based functional evaluation of non‐operative and operative treatment after anterior cruciate ligament injury. Scandinavian journal of medicine & science in sports 2009;19(3):345-55.
The Ziauddin University is on the list of I4OA, I4OC, and JISC.
This is an open- access article distributed under the terms of the Creative Commons Attribution License (CC BY 4.0).