
Aribah Ahmed 1, Nabeel Baig2*, Dr. Ummul Kiram Sheikh Zain-ul-Abedin3
1MPhil Candidate, Ziauddin College of Rehabilitation Sciences, Ziauddin University, Karachi, Pakistan![]()
2Assistant Professor, Ziauddin College of Rehabilitation Sciences, Ziauddin University, Karachi, Pakistan![]()
3Saifee Hospital, Karachi, Pakistan![]()
ABSTRACT
Background of the Study: Multiple Physical Therapy approaches have recently been developed and reported in the literature for providing better results in the treatment regimens of tension-type headaches. The advancement in the field of Physical therapy towards the treatment approaches of tension-type headaches has become the driving force for writing this article.
Methodology: Studies comparing the effects of physical therapy management with conventional treatment approaches are included in the meta-analysis. PRISMA guidelines were used for performing the qualitative analysis and assessment of risk of biases.
Results: According to the findings of nine randomized controlled trials, the analysis of the results had revealed that physical therapy intervention demonstrated a significant improvement in reducing headache severity. In a random effect model, the pool effects of physical therapy strategies in terms of Standardized Mean Difference had an impact of 1.41, which according to a Cohen rule of thumb displays a larger effect of physical therapy management in significant decrease in pain intensity among tension-type headache patients
Conclusion: The study has concluded that physical therapy-based management strategies as provided in several RCTs analyzed in this review article revealed a pool effect of moderate size in managing the frequency of pain and a larger effect size in managing pain intensity and duration. Further, it was concluded that tension-type headaches can be effectively managed through physical therapy-based approaches.
Keywords: Functional status, parkinson disease, cognitive dysfunction, disease progression, orthostatic hypotension, tremors.

Introduction
Primary headache including tension-type headache and migraine headaches are among the commonly occurring form of headaches that affects almost 47% of the world population1. Among different types of headaches, the tension-type headache has a prevalence of around 35%, whereas migraine has a remaining 12% of prevalence out of the total population that has been affected by headaches2. According to the study, tension-type headache greatly impacts socioeconomic conditions around the globe while creating an economic burden of around 1.6 billion dollars every year; making it one of the costliest disorders worldwide3. Patients complaining of tension-type headaches usually describe the pain as a band around the head in the form of pressing and tightening and not throbbing and pulsating, which occurs bilaterally with the intensity of mild to moderate4. Tension-type headache does not aggravate usually while performing routine activities such as climbing and descending stairs. Patients suffering from tension type headaches also do not complain of nausea and vomiting; which is actually an obvious symptom associated with migraine5,6. Studies have also provided significant evidence that tension-type headache is 1.5 times more frequent among the female population than males whereas it has also been estimated that during menstrual periods and pregnancy, women experience a more frequent bout of pain including both tension-type headache and migraine; which in some cases even leads to depression among females7. Several factors have been considered as a cause of tension-type headaches that includes sleep disturbance, emotional stress, nociceptive muscle pain, muscular tightness, and trigger point on and around the neck8. Various management approaches ranging from the prescription of analgesic medication to lifestyle modification have been recommended by the clinician but the role of physical therapy management approaches has made a substantial advancement in providing the long-term palliative relief to the patients9,10. Multiple Physical Therapy approaches have recently been developed and reported in the literature for providing better results as the treatment approaches of tension-type headache which includes strategies like mobilization, manipulation, combination therapy, the release of Trigger points (TrPs), and application of electrotherapy modalities11,12. This recent advancement in the field of Physical therapy towards the management of tension-type headaches has become the driving force for the writing of this review as much literature is available in the database that has been claiming the efficacy of physical therapy-based management approaches in relieving pain. Hence, the current study is being conducted to determine the effects of physical therapy-based management approaches on tension-type headaches.
Methodology
The guidelines of Preferred Reporting Items of Systematic Review and Meta-Analysis (PRISMA) were followed.
Electronic Databases and Searching Strategies
The researcher incorporated literatures found in the database including Medline, Pedro, Google Scholar, and Web of Sciences. The following MESH words has been used: Tension-type headache, physical therapy, trigger points, and pain. Search Strategies includes use of bullion “and” & “or”
Criteria for Eligible Studies and Participants
Comparative study in which the effects of physical therapy management with conventional treatment approaches are included in the inclusion criteria which determines the impact on intensity, duration, and severity of tension-type headache patients aged >18 years. Articles which are available in full text and English language during the year of 2017 to 2020 have been incorporated as latest research as a source of evidence.
Trials in which any other treatment strategies were incorporated like neck collars and pharmacological pain management strategies other than exercise based approaches were excluded. Besides this, Full-text articles which were unavailable and published articles in which the language was un-preferred were not considered.
Quantitative Analysis
MedCalc Statistical Software was used for quantitative analysis (Version 18.11.3). Inferential statistics were drawn through Continuous measure analysis using a standardized mean difference (SMD). The levels of effect size were measured through Cohen’s rule of thumb classification that categories effect size as small= 0.2 to 0.5; moderate=0.5 to 0.8; and large= >0.8. Heterogeneity was determined by the value of I2.
Extraction and analysis of data
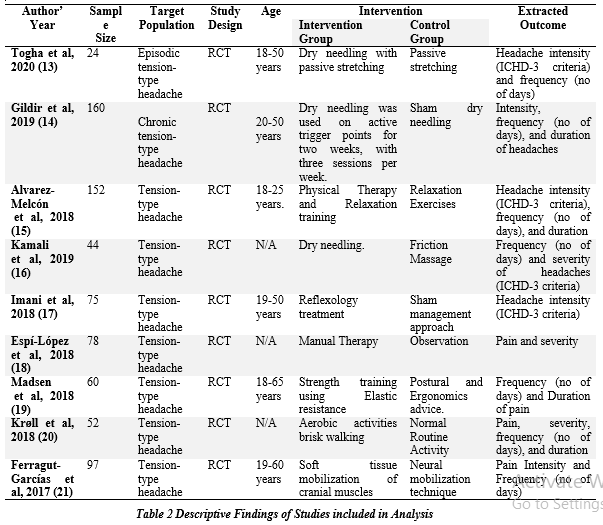
The data was fetched according to the publication year, study design, targeted population, intervention type, experimental and control group respectively, and the extracted outcome as shown in table 113,21.
Risk of Bias
Analysis for Risk of Bias was performed on the parameters such as allocation (Random and Concealment), Blinding (Participants and assessment of outcomes), reporting (outcome data and selected), and publication bias22.
Quality Appraisal and Risk of Bias
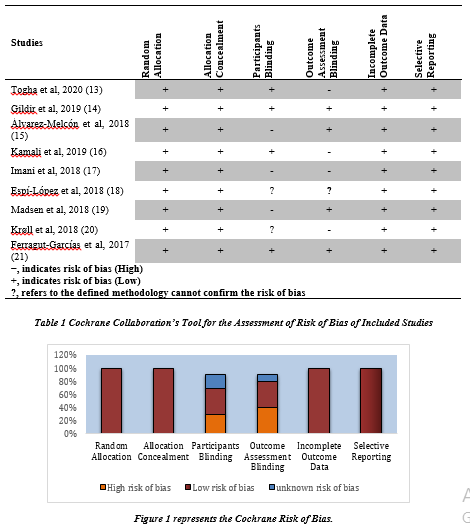
The risk of bias was analyzed on the basis of the decision of author using Cochrane tool. The tool was used to assess the risk of bias in the domains as shown in Table-1, Figure-1:
Random Sequence Generation
Low level risk of bias had been observed in all nine studies13,14,15,16,17,18,19,20,21.
Allocation Concealment
Similarly, for all randomized controlled trials, the concealed allocation was marked down to have a minimal risk of bias13,14,15,16,17,18,19,20,21.
Blinding of Participants and Personnel
Four studies13,14,16,21 considered personnel blinding and the participants, whereas three of the studies15,17,19 showed a less risk of bias and two studies18,20 showed an unknown risk of bias.
Blinding of Assessment Outcome
Four studies14,15,19,21 were found to show a low risk of bias while, four studies13,16,17,20 came up with a high risk of bias14,17,22 whereas only one study18 represented an unknown risk.
Incomplete Outcome Data
All studies were found to have a less risk of bias13,14,15,16,17,18,19,20,21,22.
Selective Reporting
All studies were found to reveal a less risk of bias13,14,15,16,17,18,19,20,21,22.
Result
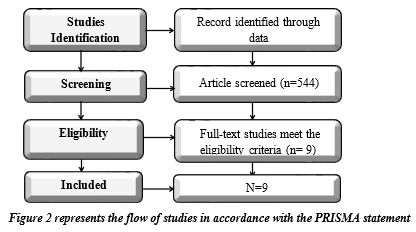
A total number N=9 studies were included, after the detailed searching for potentially relevant articles which were published. Searching was performed from various electronic databases. The search strategy produced 790 original articles which were evaluated on the basis of their content and title whereas relevant articles which were full-text were sorted and selected after the elimination of 246 duplications, elimination of articles due to lack of full-text articles, and those which were in un-preferred language. After the full-text screening, only 9 randomized controlled trials met the inclusion criteria targeted physical therapy management approaches on intensity, duration, and severity of tension-type headache. The flow of studies is illustrated in Figure 2.
Effects of physical therapy-based management approaches Analysis on the intensity of pain
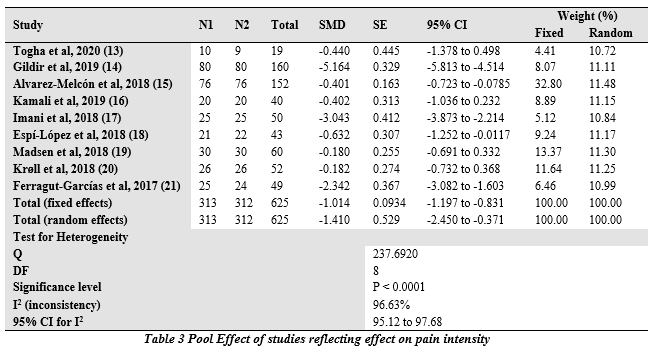
The analysis of various studies revealed that physical therapy intervention demonstrated a significant improvement in reducing headache severity, according to the findings of nine randomized controlled trials. In a random effect model, the pool effects of physical therapy strategies in terms of SMD had an impact of 1.41, which according to a Cohen rule of thumb displays a larger effect of physical therapy management in decreasing pain intensity prominently among tension-type headache patients (Table 2).
The combined effects of physical therapy management strategies on pain intensity were illustrated in figure 3.

Standardized Mean Difference on Pain Intensity
The combined outcome of the studies included in this analysis on pain intensity revealed an effect size of 1.41 (t value -2.664, P 0.008) suggesting a larger effect of the physical therapy-based intervention on pain intensity among tension-type headache patients. A random effect model had been used for interpretation due to the larger percentage of heterogeneity among studies as reflected by the value of I2 = 96.63%.
Effect of physical therapy-based management approaches Analysis on the frequency of pain
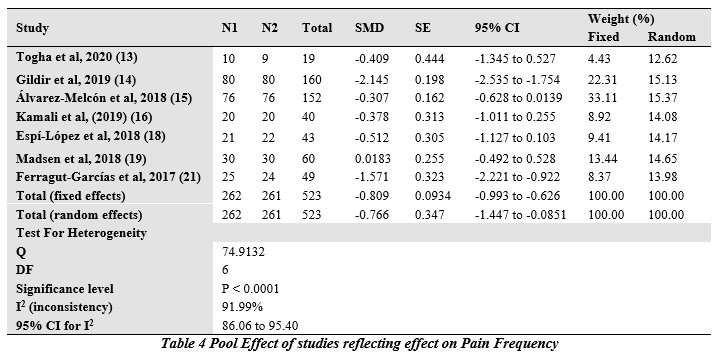
Physical therapy intervention demonstrated a significant improvement in lowering the frequency of pain, according to the consequent finding of seven randomized controlled trials it was observed that the frequency of pain among the tension-type headache patients had been reduced as shown in forest plot Figure 4.
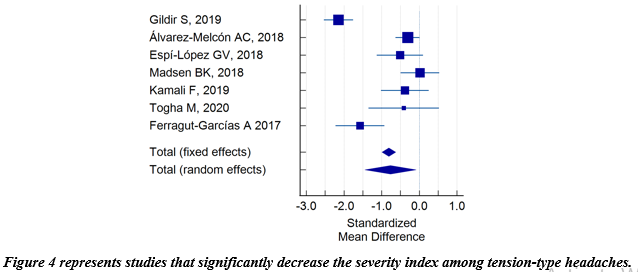
Analysis of the frequency of Pain using a Standardized Mean Difference Model
The analysis revealed an effect size of -0.766 (t value -2.210, P 0.028) which suggest a moderate level of improvement in the frequency of pain among tension-type headache patients. Random effect Model had been used for determining the pool effects due to the high percentage of heterogeneity among different studies I2 = 91.99, represented in table 4.
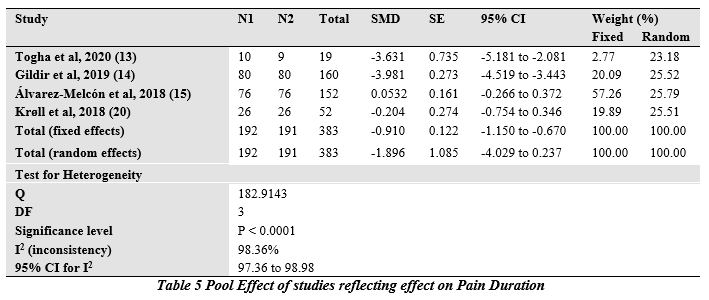
Analysis of the effect of physical therapy-based management approaches on the duration of pain
Four studies out of 9 had determined the effects of physical therapy on the duration of pain and had provided evidence that the impact of physical therapy-based management approaches reduces the duration of pain as depicted in figure 5.
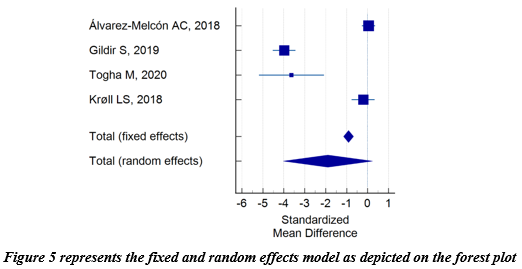
Standardized Mean Difference analysis on the duration of pain
The analysis revealed that the combined effect of studies at the random effect model showed an effect size of -1.89 (t value -1.747, P 0.081) which suggested a large effect of intervention in decreasing the duration of pain. The pool effect at random effect model was used because of the higher percentage of heterogeneity I2=98.36% as shown in Table 5.
Discussion
The result provided the evidence that physical therapy interventions reported in different studies including this analysis had revealed that the intensity and duration of pain had been reduced with larger effect sizes whereas the frequency of pain had been reduced with an effect size of moderate impact as estimated using a random effect model due to high percentage of heterogeneity among the studies. The findings of our analysis were according to the finding of another study in which the effects of manual therapy were determined on headaches and it was estimated in that analysis that manual therapy was found to be effective in reducing the headache disability index with an estimated effect size -4.01 however in the same study no account has been mentioned in identifying pain intensity, duration, and frequency23.
Similarly, in another study, spinal manipulation techniques effects had been determined on migraine and it was observed that spinal manipulation had a small effect of Hedges g = -0.34 as identified on the frequency of pain. Further, the analysis was performed on n=6 RCTs24. In a study conducted on determining the effects of aerobic exercises in which the studies were incorporated from the period of 1950 to 2009, it had been observed that SMD of 1.25 had been noticed on pain intensity, SMD of 0.76 on frequency, and SMD of 0.41 on duration revealing the fact that exercises had a mild to moderate impact on reliving migraine symptoms pertinent to pain but these reviews were only limited to migraine25. We in this study had come across certain good evidence that physical therapy-based management approaches including dry needling, combination exercises, mobilization, and TrPs releasing strategies were all provided findings favoring tension-type headache management through physical therapy intervention. Hence authors of this study concludes that physical therapy approaches could be a choice of intervention in the pain management of tension-type headaches.
Conclusion
The study has concluded that physical therapy-based management strategies as provided in several RCTs, analyzed in this review article revealed a pool effect of moderate size in managing the frequency of pain and a larger effect size in managing pain intensity and duration. Further, it was concluded that tension-type headaches can be effectively managed through physical therapy-based approaches.
AUTHORS’ CONTRIBUTION:
The following authors have made substantial contributions to the manuscript as under:
Conception or Design: Aribah Ahmed
Acquisition, Analysis or Interpretation of Data: Nabeel Baig
Manuscript Writing, Critical Review & Approval: Aribah Ahmed, Dr. Ummul Kiram
All authors acknowledge their accountability for all facets of the research, ensuring that any concerns regarding the accuracy or integrity of the work are duly investigated and resolved.
ACKNOWLEDGEMENTS: We thanks all the participants in this study.
INFORMED CONSENT: Written Informed Consent was taken from each patient.
CONFLICT OF INTEREST: The author(s) have no conflict of interest
FUNDING STATEMENTS: Aribah Ahmed
ETHICS STATEMENTS: The study has been approved by the ERC Ziauddin University in the meeting of January 2022 with the referenc code: 4541121AAREH.
References
- Fernández-de-Las-Peñas C, Fernández-Muñoz JJ, Palacios-Ceña M, Parás-Bravo P, Cigarán-Méndez M, Navarro-Pardo E. Sleep disturbances in tension-type headache and migraine. Therapeutic advances in neurological disorders. 2018 Jan 10;11: 1756285617745444.
- Li C, Zhang L, Zhou J, Fan Z, Wang Y, Wang X, Wang W, Yu S. Prevalence of primary headache disorders among information technology staff in China: the negative effects of computer use and other correlative factors. BMCPH. 2020 Dec;20(1):1-0.
- Simić S, Rabi-Žikić T, Villar JR, Calvo-Rolle JL, Simić D, Simić SD. Impact of individual headache types on the work and work efficiency of headache sufferers. International journal of environmental research and public health. 2020 Jan;17(18):6918.
- Palacios-Ceña M, Wang K, Castaldo M, Guillem-Mesado A, Ordás-Bandera C, Arendt-Nielsen L, Fernández-de-Las-Peñas C. Trigger points are associated with widespread pressure pain sensitivity in people with tension-type headache. Cephalalgia. 2018 Feb;38(2):237-45.
- Burch R. Migraine and tension-type headache: diagnosis and treatment. Medical Clinics. 2019 Mar 1;103(2):215-33.
- Ailani J, Burch RC, Robbins MS, Board of Directors of the American Headache Society. The American Headache Society Consensus Statement: Update on integrating new migraine treatments into clinical practice. Headache: The Journal of Head and Face Pain. 2021 Jul;61(7):1021-39.
- Delaruelle Z, Ivanova TA, Khan S, Negro A, Ornello R, Raffaelli B, Terrin A, Mitsikostas DD, Reuter U. Male and female sex hormones in primary headaches. The journal of Headache and Pain. 2018 Dec;19(1):1-2.
- Fuensalida-Novo S, Jiménez-Antona C, Benito-González E, Cigarán-Méndez M, Parás-Bravo P, Fernández-De-Las-Peñas C. Current perspectives on sex differences in tension-type headache. Expert Review of Neurotherapeutics. 2020 Jul 2;20(7):659-66.
- Jiang W, Li Z, Wei N, Chang W, Chen W, Sui HJ. Effectiveness of physical therapy on the suboccipital area of patients with tension-type headache: A meta-analysis of randomized controlled trials. Medicine. 2019 May;98(19).
- Bentivegna E, Luciani M, Paragliola V, Baldari F, Lamberti PA, Conforti G, Spuntarelli V, Martelletti P. Recent advancements in tension-type headache: a narrative review. Expert review of neurotherapeutics. 2021 Jul 3;21(7):793-803.
- Coelho M, Ela N, Garvin A, Cox C, Sloan W, Palaima M, Cleland JA. The effectiveness of manipulation and mobilization on pain and disability in individuals with cervicogenic and tension-type headaches: a systematic review and meta-analysis. Physical Therapy Reviews. 2019 Mar 4;24(1-2):29-43.
- Carvalho GF, Schwarz A, Szikszay TM, Adamczyk WM, Bevilaqua-Grossi D, Luedtke K. Physical therapy and migraine: musculoskeletal and balance dysfunctions and their relevance for clinical practice. Brazilian journal of physical therapy. 2020 Jul 1;24(4):306-17.
- Abaschian F, Mansoursohani S, Togha M, Yassin M, Abadi L. The Investigation of the effects of deep dry needling into trigger points of temporalis, sternocleidomastoid and upper trapezius on females with episodic tension type headache. Researcher Bulletin of Medical Sciences. 2020;25(1):e6-.
- Gildir S, Tüzün EH, Eroğlu G, Eker L. A randomized trial of trigger point dry needling versus sham needling for chronic tension-type headache. Medicine. 2019 Feb;98(8).
- Álvarez-Melcón AC, Valero-Alcaide R, Atín-Arratibel MA, Melcón-Álvarez A, Beneit-Montesinos JV. Effects of physical therapy and relaxation techniques on the parameters of pain in university students with tension-type headache: a randomized controlled clinical trial. Neurología (English Edition). 2018 May 1;33(4):233-43.
- Kamali F, Mohamadi M, Fakheri L, Mohammadnejad F. Dry needling versus friction massage to treat tension type headache: a randomized clinical trial. Journal of bodywork and movement therapies. 2019 Jan 1;23(1):89-93.
- Imani N, Shams SA, Radfar M, Ghavami H, Khalkhali HR. Effect of applying reflexology massage on nitroglycerin-induced migraine-type headache: A placebo-controlled clinical trial. Agri. 2018 Jul 1;30(3):116-22.
- Monzani L, Zurriaga R, Espí López GV. Anxiety and the severity of tension-type headache mediate the relation between headache presenteeism and workers’ productivity. PLoS One. 2018 Jul 19;13(7):e0201189.
- Madsen BK, Søgaard K, Andersen LL, Tornøe B, Jensen RH. Efficacy of strength training on tension-type headache: A randomised controlled study. Cephalalgia. 2018 May;38(6):1071-80.
- Krøll LS, Hammarlund CS, Linde M, Gard G, Jensen RH. The effects of aerobic exercise for persons with migraine and co-existing tension-type headache and neck pain. A randomized, controlled, clinical trial. Cephalalgia. 2018 Oct;38(12):1805-16.
- Ferragut-Garcías A, Plaza-Manzano G, Rodríguez-Blanco C, Velasco-Roldán O, Pecos-Martín D, Oliva-Pascual-Vaca J, Llabrés-Bennasar B, Oliva-Pascual-Vaca Á. Effectiveness of a treatment involving soft tissue techniques and/or neural mobilization techniques in the management of tension-type headache: a randomized controlled trial. Archives of physical medicine and rehabilitation. 2017 Feb 1;98(2):211-9.
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Moher D. Updating guidance for reporting systematic reviews: development of the PRISMA 2020 statement. Journal of clinical epidemiology. 2021 Jun 1;134:103-12.
- Falsiroli Maistrello L, Rafanelli M, Turolla A. Manual therapy and quality of life in people with headache: systematic review and meta-analysis of randomized controlled trials. Current pain and headache reports. 2019 Oct;23(10):1-4.
- Rist PM, Hernandez A, Bernstein C, Kowalski M, Osypiuk K, Vining R, Long CR, Goertz C, Song R, Wayne PM. The impact of spinal manipulation on migraine pain and disability: a systematic review and meta‐analysis. Headache: The Journal of Head and Face Pain. 2019 Apr;59(4):532-42.
- Lemmens J, De Pauw J, Van Soom T, Michiels S, Versijpt J, Van Breda E, Castien R, De Hertogh W. The effect of aerobic exercise on the number of migraine days, duration and pain intensity in migraine: a systematic literature review and meta-analysis. The journal of headache and pain. 2019 Dec;20(1):1-9.
The Ziauddin University is on the list of I4OA, I4OC, and JISC.
This is an open- access article distributed under the terms of the Creative Commons Attribution License (CC BY 4.0).