
Hina Gul1*, Iqra Tahir2
1*Assistant professor, Riphah International University QIE Campus, Lahore, Pakistan![]()
2Student, Riphah International University QIE Campus, Lahore, Pakistan![]()
ABSTRACT
Background and Aim: To compare the effects of mulligan rotational movement and medial gapping technique on pain, range of motion and disability in knee osteoarthritis patients.
Methodology: This study was a Randomized Clinical Trial. The data was collected using a convenience sampling technique. Data was collected from Jinnah Hospital Lahore, from 15th December – 30th June 2022.36 subjects (males and females) were recruited in two groups. The first group received Mobilization with movement along with a conservative treatment protocol. The second group received the Medial gapping technique along with conservative treatment protocol. Each group was treated for four weeks in which three sessions per week were given. Numeric pain rating scale and the disability index were used as outcome measures. Data was analyzed through statistical package for the social sciences (SPSS) version 25.
Results: Within-group comparison by paired t-test showed the p-value was significant <.05, indicating that both treatment was effective in improving symptoms. Between groups, comparison by independent t-test showed that Mulligan Mobilization Technique is more effective than the medial gapping technique in improving pain disability and quality of life.
Conclusion: The study concluded that Mulligan Mobilization Technique provides more clinical benefits regarding pain, disability and range of motion in osteoarthritis patients than Medial Gapping Technique.
Keywords: Arthritis, knee osteoarthritis, movement, pain, patients, range of motion.

Introduction
Osteoarthritis is also known as an outcome of some joint’s inability to restore itself after facing abnormal forces due to any deviations of the joint or periarticular structures from normal stability. Osteoarthritis affects the whole joint, despite the fact that the loss of cartilage is its primary symptom. Within a knee and amongst individuals, the rate of advancement changes over time. Osteoarthritis of knee joint presents with the symptoms that include joint pain, knee stiffness, decreased joint motion, and weakness of muscles. Due to high level of mobility and lack sufficient stability, knee joint is more prone to osteoarthritis3. Knee osteoarthritis affects three parts of the knee joint (medial, lateral, and patellar-femoral joints) and progresses slowly, usually over 10-15 years, restricting our daily activities. Regardless of the intrinsic mechanism, OA means damage to articular cartilage, bone spur formation, hardening of subchondral bone and loss of joint space. Many factors play a role in the etiology of knee osteoarthritis. Most general factors include morbidly obese people, ageing of a person, sex of person (more frequent in females), people who carry out heavy weight training and climbing stairs daily, genes and hereditary also play significant role in the causation of disease. Exercise, stretching, transcutaneous electrical nerve stimulation and manual therapy are recommended in all clinical guidelines because knee osteoarthritis is correlated with relatively few side effects. Quadriceps strengthening has traditionally been a main part of the knee osteoarthritis exercise program. This is because quadriceps weakness is a frequent complaint in people with knee osteoarthritis. Therefore, it is clear that a substitute exercise program is needed to decrease knee tension and lessen the symptoms of patients with medial compartment OA and varus deformity. Neuromuscular training is a relatively expanded category of exercise plans, including programs termed as functional training. Neuromuscular exercise is usually performed in an active, weight-supporting position that emphasizes the quality and efficiency of the exercise and the positioning of the trunk and lower limb joints6.
Mulligans Bent Leg Raise method with a heat pack and the MET with a hot pack is also effective in reducing pain intensity and increasing hamstring flexibility in osteoarthritis patients7. Manual Traction is also a good treatment option in treating the condition8. Exercise treatment, electrotherapy, and manual therapy are among the therapeutic methods used in the rehabilitating of OA patients (MT). Among these methods, manual therapy (MT) is a physical therapy technique that helps patients feel less pain and perform better. The body’s musculoskeletal components, including the joints, soft tissues, and nerve tissues, are treated by manual therapists to activate various biomechanical, neurophysiological, and psychological processes9.To the best of the researcher’s knowledge, limited data was available on the effects of Mulligan rotational movements vs the Medial gapping technique. As a result, this study would add knowledge to the growing body that if these two treatment techniques yield similar outcomes and if one is better than the other, which should be an alternative choice of treatment in the field of physiotherapy for the treatment of knee osteoarthritis through evidence-based approach.
Methodology
Study Design
The current study was a Randomized Clinical Trial.
Setting
The study was performed at the Physiotherapy Department of Jinnah Hospital, Lahore and Riphah Rehabilitation Centre, Lahore.
Duration of Study
The study was completed six months after the approval of synopsis.
Sample Size
By entering the following pain data from prior research into the online EPITOOL sample size calculator, the sample size of 40 was determined27.
T Tests-Means: Difference between two independent means (two groups)
Inputs
Mean 1= 24
Mean 2= 22.67
Variance = 2
Confidence level = 0.95
Power = 0.8
Tails =2
Results
Sample size
Sample size (per group) = 18
Total sample size (both groups) = 36
After the attrition rate of 10%, the sample size will be 4027
Sampling Technique
A convenient sampling technique was used to collect data.
Sample Selection
Inclusion Criteria
- Unilateral Knee OA
- Males and females between 30 and 60 years of age
- Patients suffering from Grade II osteoarthritis of the knee using the Kellgren Lawrence grading Scale.
- Patients with restricted ROM.
- Patients are having more than grade III strength of knee muscles.
Exclusion Criteria
- Patients having unstable knee joint after Total Knee Arthroplasty.
- Joint infection of hip and knee.
- Soft tissue injuries around knee joints, including tendinitis and bursitis.
- Any fracture including patellar fracture, femur or tibia.
Study groups
The participants were divided into two groups, i.e., Group A was given Mobilization with movement, whereas Group B was given the Medial Gapping Technique.
Baseline treatment
Modalities:
Transcutaneous Electrical Nerve Stimulation TENS (F=100Hz, I=12mA, T=high TENS, T=20min), hydro collateral hot pack for 40 minutes and strengthening and stretching exercise for Quadriceps and hamstrings, respectively irrespective of the cause or region involved in knee OA.
Exercise Program:
- Quads strengthening (knee press ball)
5 seconds/ 20 repetitions 2 times a day.
- Hamstring stretching (Straight Leg Raise)
5 seconds and repeat it 10 times.
- Strengthening of hip abductors
Gravity eliminated=10 times without hold
Against gravity=10 times each.
Group A: Mulligan rotational movements for 4 weeks, 3 sessions per week.
Protocol for Group A
Mulligan Rotational Movements:
The patient was in a supine position, and the therapist stood next to the affected knee. The therapist put both hands on the flexed knee, fingers interlaced, with the heel of one hand resting over the tibial tuberosity and the heel of the second hand resting over the lower end of the femur. The tibial plateau was then glided posteriorly, and the patient was instructed to bend their knee as the glide was maintained with mild overpressure. A Mulligan belt was used to help the patient, significantly to enhance flexion. One end of the belt was wrapped around the ankle joint on the limited side, while the other was gripped by the patient’s hands17.
Group B: Medial gapping technique was applied for 4 weeks,3 sessions per week.
Protocol for Group B
Medial Gapping Technique:
The patient is laid supine with the hip in flexion, adduction and internal rotation. The therapist is standing lateral to the patient knee. The therapist holds the calcaneus from the medial side, externally rotating the patient’s foot and ankle using his forearm. At the same time, therapist is holding the lateral part of patient’s knee over the joint space. At this point, therapist applies valgus stress in the knee on the joint space. As a result, “Gapping up” the medial side of knee joint. Then he gradually extends the knee or asks the patient to extend his knee actively.
Home Plan
- To help soothe stiff joints and relax muscles, use hot packs for 10 to 15 minutes.
- Avoid Cross Leg Sitting.
- Always warm up your joint before standing from sitting to lying by straightening and bending your leg for 10 to 15 minutes so that the knee is prepared well to take the pressure.
- Wear knee cap when the knee is in weight bearing position, e.g., stair climbing and long standing.
- Place cushion between knees is side lying position when sleeping.
- Try to take a healthy diet that assists Weight loss.
- Exercise including SLR, Quads and VMO strengthening 10 repetitions 3 times daily.
- Pain relievers’ drugs when pain exacerbates.
Data Analysis Procedure
- The SPSS for Windows program, version 21, was used to analyze the data. P = 0.05, was chosen as the threshold for statistical significance Following tests were used:
- A parametric test was applied to compare two populations at varied intervals.
- Descriptive Statistics: To show a summary of group measures collected over time, frequency tables, pie charts, and bar charts were used.
- Difference between Groups: Independent sample t-test was used to compare two populations at various intervals.
- Difference within Groups: paired t test was used to compare a single group at various intervals.
Results
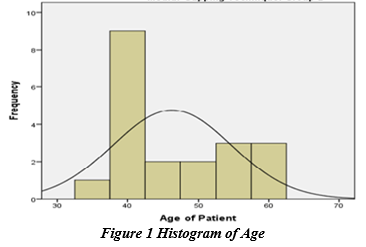
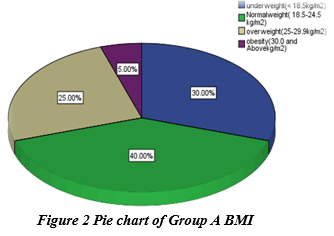
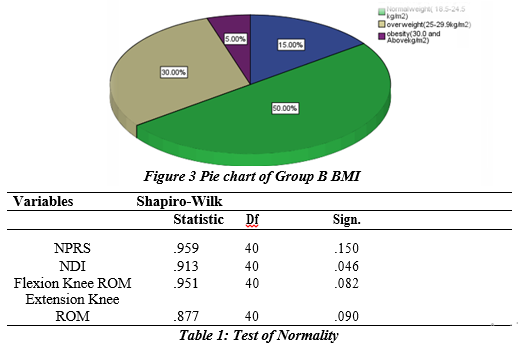
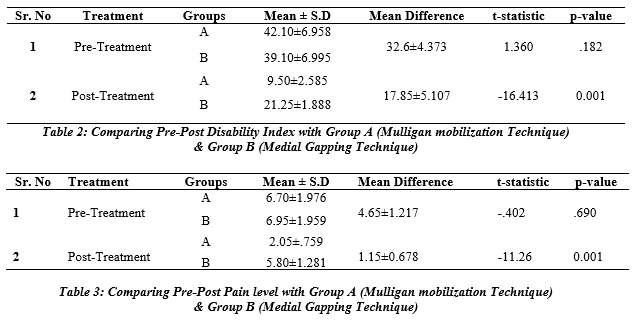
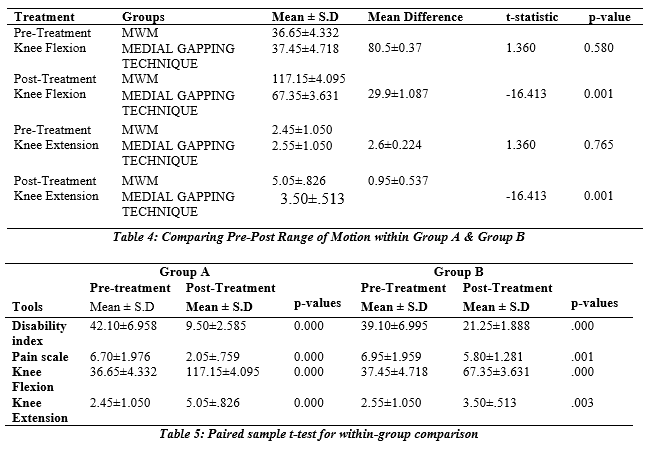
According to the normality test (Shapiro-Wilk: because sample size less than 50). After applying the test of normality, data was normally distributed with a significant p-value (>0.05). The parametric test was used, independent t-test applied for group comparison. Paired t-test applied for within-group comparison. The average mean age of participants was 48.9±7.159 years. In group A and group B was 46.3±8.392. The mean height of participants was 6.66±.395 years. In Group A and Group B mean height was 5.67±.336. The participants’ mean weight was 56.8 ±5.61kg, in Group A it was 64.6±10.72 and in group B it was 69.5±1.261. In group A, 25% were male and 75% were female. In group B 30% were male and 70% were female. In group A, 30% of patient was underweight, 40% were of normal weight, 25% were overweight and 5% fall under the category of obese. In group B, 15% of patient was underweight, 50% were of normal weight, 30% were overweight and 5% fall under the category of obese. The findings showed that, for pre-treatment p-value = .182 > .05 which is insignificant and indicated that the Mulligan Mobilization Technique and Medial Gapping Technique were same for disability scale. Whereas the post-treatment data suggested that the Mulligan Mobilization was effective, with significant outcomes of .001 to.05 and Medial Gapping Technique were significant for disability scale. However, mean difference for group A 32.6±4.373 shows the more improvement than group B 17.85±5.107, that shows the more effectiveness of Mulligan Mobilization Technique than Medial Gapping Technique in improving disability in osteoarthritis.
The findings showed that, for pre-treatment p-value = .690 > .05, which is insignificant and indicated that the Mulligan Mobilization Technique and Medial Gapping Technique were the same for pain scale. Whereas the after treatment showed the significant results as .001 < .05 and indicated that the Mulligan Mobilization Technique and Medial Gapping Technique were significant for pain scale. However, mean difference for group A 4.65±1.217 shows the more improvement than group B 1.15±0.678, that shows the more effectiveness of Mulligan Mobilization Technique than Medial Gapping Technique in improving pain in osteoarthritis. The findings showed that, for pre-treatment p-value = .580 > .05 which is insignificant and indicated that the Mulligan Mobilization Technique and Medial Gapping Technique were same for Knee flexion. While the post-treatment analysis revealed significant findings of.001 to.05 and demonstrated the effectiveness of the Mulligan Mobilization Technique and Medial Gapping Technique were significant for Knee flexion. However, mean difference for group A 80.5±0.37 shows the more improvement than group B 29.9±1.087, that shows the more effectiveness of Mulligan Mobilization Technique than Medial Gapping Technique in improving knee flexion in osteoarthritis.
The findings showed that, for pre-treatment p-value = .765> .05 which is insignificant and indicated that the Mulligan Mobilization Technique and Medial Gapping Technique were same for Knee Extension. Whereas the after treatment showed the significant results as .001 < .05 and indicated that the Mulligan Mobilization Technique and Medial Gapping Technique were significant for Knee Extension. However, mean difference for group A 2.6±0.224 shows the more improvement than group B 0.95±0.537, that shows the more effectiveness of Mulligan Mobilization Technique than Medial Gapping Technique in improving knee extension in osteoarthritis.The Disability Scale, Pain Scale, and Paired Sample T Test were utilized to evaluate the pre-post effects. In Group A (Mulligan mobilization Technique) the p-value for each instrument was less than.05, indicating that the treatment was successful and the patients had improved following it. For group B (Medial Gapping Technique), the p-value for each tool was also less than.05, indicating that the therapy was successful and that the patients’ conditions had improved.
Outcome measures
- Goniometer (Validity=0.97, Reliability=0.98)
- Numeric Pain Rating Scale (NPRS) (Validity=, Reliability=)
- Disability Index(Validity=, Reliability=)
Discussion
Mulligan mobilization has been shown to enhance mechanical loading, joint stability, and endurance of weak muscles through mechanical, self-confidence, and motivational aspects for ROM. In a cohort trial, KOA patients were given a manual physical therapy programme that focused on passive extension mobilization of the knee, and the restorative benefits in the Mulligan mobilization group were not superior to those in the exercise group. Current study concluded the same result that Mulligan mobilization Technique provide more clinical benefits regarding pain, disability and range of motion in osteoarthritis patient’s31.Ola Grimsby, in his book “Science, Theory and Clinical Application in Orthopedic Manual” discussed about different manual techniques. Some of these were used for assessment and some were for the treatment purposes. Among those techniques, he used a medial gapping technique for the increase in knee range of motion. In the current study, medial gapping technique is applied to see its beneficial effects on knee osteoarthritis in comparison with mulligan’s mobilization technique. It showed that medial gapping technique is effective but less than mulligan’s mobilization technique40.Gupta et al. discovered that mobilization significantly improved pain reduction, physical impairment, including knee joint proprioception. This might imply that the expelling out of fluid during each compression and consuming of fluid when the compression is released has a favorable effect on joint nourishment. Squeezing happens when the mobilization method is used, and fluid ingesting happens when the joint is lax. This might be the cause of the pain decrease and subsequent eventually betterment in ROM and function observed at the completion of the therapy session 34.
Current study concluded the same result that Mulligan mobilization Technique improve pain Kaya Mutlu et al. discovered that mulligan mobilization is more effective than the control group in lowering pain, enhancing quadriceps muscular power, knee range of motion, and functional level in knee OA participants 37. Current study concluded the same result that Mulligan Mobilization Technique provide more clinical benefits regarding pain in osteoarthritis. Bhagwat and colleagues when compared to the placebo group, mobilization reduced knee discomfort and improved physical mobility in knee OA patients. This might be linked to the biomechanical mechanics of Mulligan’s MWM notion. The treatment glides utilized in the intervention group may have immediately changed the osteoarthritic knee’s typical kinematics. resulting in immediate pain relief 38. Current study concluded the same result that Mulligan mobilization Technique improve pain, ROM in osteoarthritis patients Alkhawajah and Alshami discovered that Mobilization surpassed the sham group in terms of pain relief, physical function (TUG), and knee flexion. In contrast, WOMAC demonstrated no noticeable impact on knee patients OA (P=0.067). This might be because of the fact that the OA grade was relatively low, indicating little limitation of functional activities. 32 Current study concluded the same result that Mulligan Mobilization Technique provide more clinical benefits regarding pain ROM in osteoarthritis. Saddam Hussain Shaik et al the reduction in pain in the intervention group might be attributed to the idea that Mobilization calms a concerned, accelerated system, particularly the dorsal horn, by shocking it with pain free normality that it has been freckled to receive. One more likely cause is that central processes are implicated, because the no opioid mediate CNS pain restricting system is activated. Furthermore, the arthrokinetic reflex, which is characterized by joint mechanoreceptor afferent activity on muscles surrounding the joint, is assumed to be the mechanism responsible for quadriceps peak torque augmentation 39. Current study concluded the same result that Mulligan Mobilization Technique provides more clinical benefits regarding pain in osteoarthritis.
Conclusion
The study concluded that Mulligan Mobilization Technique provide more clinical benefits regarding pain, disability and range of motion in osteoarthritis patients than Medial Gapping Technique.
AUTHORS’ CONTRIBUTION:
The following authors have made substantial contributions to the manuscript as under:
Conception or Design: Hina Gul, Iqra Tahir
Acquisition, Analysis or Interpretation of Data: Hina Gul, Iqra Tahir
Manuscript Writing & Approval: Hina Gul, Iqra Tahir
All authors acknowledge their accountability for all facets of the research, ensuring that any concerns regarding the accuracy or integrity of the work are duly investigated and resolved.
ACKNOWLEDGEMENTS: Special thanks to Riphah international university for providing research facilities.
INFORMED CONSENT: Written Informed Consent was taken from each patient.
CONFLICT OF INTEREST: The author (s) have no conflict of interest regarding any of the activity perform by PJR.
FUNDING STATEMENTS: None declared
ETHICS STATEMENTS: The protocol of the present study was registered by the local ethics committee of Riphah international university approval code REC/RCR & AHS/22/0142/registered in Clinical Trial.gov NCT05338840.
References
- Atalay SG, Durmus A, Gezginaslan Ö. The Effect of Acupuncture and Physiotherapy on Patients with Knee Osteoarthritis: A Randomized Controlled Study. Pain Physician 2021;24(3):E269.
- Sharma L. Osteoarthritis of the Knee. N Engl J Med 2021;384(1):51-59.
- Lalnunpuii A, Sarkar B, Alam S, Equebal A, Biswas A. Efficacy of mulligan mobilisation as compared to Maitland mobilisation in females with knee osteoarthritis: a double blind randomized controlled trial. International Journal of Therapies and Rehabilitation Research 2017;6(2):37.
- Jagatheesan alagesan rk, srinivasan v. Efficacy of resisted exercise in knee osteoarthritis among female population. Turkish Journal of Physiotherapy and Rehabilitation.;32:2.
- Alsiri NF, Alhadhoud MA, Al‐Mukaimi A, Palmer S. The effect of Mulligan’s mobilization with movement following total knee arthroplasty: Protocol of a single‐blind randomized controlled trial. Musculoskeletal Care 2021;19(1):20-7.
- Bennell KL, Egerton T, Wrigley TV, Hodges PW, Hunt M, Roos EM, et al. Comparison of neuromuscular and quadriceps strengthening exercise in the treatment of varus malaligned knees with medial knee osteoarthritis: a randomised controlled trial protocol. BMC musculoskeletal disorders 2011;12(1):1-12.
- Tariq K, Shoukat F, Ahmed U. Effectiveness of Mulligan s Bent Leg Raise Technique Versus Muscle Energy Technique on Pain Intensity and Hamstring Flexibility in Patients with Knee Osteoarthritis. Rawal Medical Journal 2020;45(2):358-.
- Karokaro TM, Jehaman I, Gurusinga R, Hayati K, Bintang SS, Sitepu SDEU, et al. The Effect of Roll Slide Mobilization and Traction Manual on Knee Pain Scale Intensity Patients with Osteoarthritis.
- Tsokanos A, Livieratou E, Billis E, Tsekoura M, Tatsios P, Tsepis E, et al. The efficacy of manual therapy in patients with knee osteoarthritis: a systematic review. Medicina 2021;57(7):696.
- Teo PL, Bennell KL, Lawford BJ, Egerton T, Dziedzic KS, Hinman RS. Physiotherapists may improve management of knee osteoarthritis through greater psychosocial focus, being proactive with advice, and offering longer-term reviews: a qualitative study. Journal of Physiotherapy 2020;66(4):256-65.
- Weleslassie GG, Temesgen MH, Alamer A, Tsegay GS, Hailemariam TT, Melese H. Effectiveness of mobilization with movement on the management of knee osteoarthritis: a systematic review of randomized controlled trials. Pain Research and Management. 2021;1-2.
- Nigam A, Satpute KH, Hall TM. Long term efficacy of mobilisation with movement on pain and functional status in patients with knee osteoarthritis: a randomised clinical trial. Clinical Rehabilitation 2021;35(1):80-9.
- Mehmood Z, Anwar N, Tauqeer S, Shabbir M, Khalid K, Mehmood S. Comparison of Maitland Mobilization and Mulligan Mobilization with Movement in Knee Osteoarthritis Patients. Pakistan Journal of Medical Research 2021 Oct 25;60(3):126-30
- Nazir SN, Ali SS, Akhtar S. Effectiveness of Mulligan joint mobilizations and trunk stabilization exercises versus isometric knee strengthening in the management of knee osteoarthritis: study protocol for a randomized controlled trial. medRxiv 2020:2020-05.
- Mahmooda S, Ishaq I, Safdar M, Sabir M, Tahir A, Irshad S. Effects of Mulligan’s mobilization with movements versus myofascial release in addition to usual care on pain and range in knee osteoarthritis. Rawal Medical Journal 2020;45(2):353-7.
- Gomes MG, Primo AF, De Jesus LL, Dionisio VC. Short-term Effects of Mulligan’s Mobilization With Movement on Pain, Function, and Emotional Aspects in Individuals With Knee Osteoarthritis: A Prospective Case Series. Journal of Manipulative and Physiological Therapeutics 2020;43(5):437-45.
- Alkhawajah HA, Alshami AM. The effect of mobilization with movement on pain and function in patients with knee osteoarthritis: a randomized double-blind controlled trial. BMC Musculoskeletal Disorders 2019;20(1):1-9.
- Bhagat M, Neelapala YR, Gangavelli R. Immediate effects of Mulligan’s techniques on pain and functional mobility in individuals with knee osteoarthritis: A randomized control trial. Physiotherapy Research International 2020;25(1):e1812.
- Hedya WM. Combined effect of using static traction in some therapeutic methods to reduce knee arthritis symptoms. International Journal of Sports Science and Arts 2019;3(02):72-87.
- Alghadir AH, Anwer S, Sarkar B, Paul AK, Anwar D. Effect of 6-week retro or forward walking program on pain, functional disability, quadriceps muscle strength, and performance in individuals with knee osteoarthritis: a randomized controlled trial (retro-walking trial). BMC musculoskeletal disorders 2019;20(1):1-10.
- Lee DK. The effect of knee joint traction therapy on pain, physical function, and depression in patients with degenerative arthritis. The Journal of Korean Physical Therapy 2019;31(5):317-21.
- Kiran A, Ijaz M, Qamar M, Basharat A, Rasul A, Ahmed W. Comparison of efficacy of mulligan’s mobilization with movement with maitland mobilization along with conventional therapy in the patients with knee osteoarthritis: A randomized clinical trial. Libyan International Medical University Journal 2018;3(01):26-30.
- Altmış H, Oskay D, Elbasan B, Düzgün İ, Tuna Z. Mobilization with movement and kinesio taping in knee arthritis—evaluation and outcomes. International orthopaedics 2018;42(12):2807-15.
- Iijima H, Eguchi R, Shimoura K, Yamada K, Aoyama T, Takahashi M. Transcutaneous electrical nerve stimulation improves stair climbing capacity in people with knee osteoarthritis. Scientific reports 2020;10(1):1-9.
- Abdel-Aziem AA, Soliman ES, Mosaad DM, Draz AH. Effect of a physiotherapy rehabilitation program on knee osteoarthritis in patients with different pain intensities. Journal of physical therapy science 2018;30(2):307-12.
- Rao RV, Balthillaya G, Prabhu A, Kamath A. Immediate effects of Maitland mobilization versus Mulligan Mobilization with Movement in Osteoarthritis knee-A Randomized Crossover trial. Journal of bodywork and movement therapies 2018;22(3):572-9.
- Chew E, Perin J, Grader-Beck T, Orbai AM. Measurement of minimal disease activity in psoriatic arthritis using PROMIS-Physical Function or the Health Assessment Questionnaire-Disability Index. Arthritis care & research 2022;74(1):151..
- Shamsi M, Mirzaei M, Khabiri SS. Universal goniometer and electro-goniometer intra-examiner reliability in measuring the knee range of motion during active knee extension test in patients with chronic low back pain with short hamstring muscle. BMC Sports Science, Medicine and Rehabilitation 2019;11(1):1-5.
- Alghadir AH, Anwer S, Iqbal A, Iqbal ZA. Test–retest reliability, validity, and minimum detectable change of visual analog, numerical rating, and verbal rating scales for measurement of osteoarthritic knee pain. Journal of pain research 2018;11:851.
- Douglas‐Withers J, McCulloch K, Waters D, Parker K, Hogg N, Mitsuhashi T, et al. Associations between Health Assessment Questionnaire Disability Index and physical performance in rheumatoid arthritis and osteoarthritis. International journal of rheumatic diseases 2019;22(3):417-24.
- Albertin ES, Miley EN, May J, Baker RT, Reordan D. The Effects of Hip Mobilizations on Patient Outcomes: A Critically Appraised Topic. Journal of sport rehabilitation 2019;28(4):390-4.
- Rao RV, Balthillaya G, Prabhu A, Kamath A. Immediate effects of Maitland mobilization versus Mulligan Mobilization with Movement in Osteoarthritis knee- A Randomized Crossover trial. Journal of bodywork and movement therapies 2018;22(3):572-9.
- Alsiri NF, Alhadhoud MA, Al-Mukaimi A, Palmer S. The effect of Mulligan’s mobilization with movement following total knee arthroplasty: Protocol of a single-blind randomized controlled trial. Musculoskeletal care 2021;19(1):20-7.
- Altmış H, Oskay D, Elbasan B, Düzgün İ, Tuna Z. Mobilization with movement and kinesio taping in knee arthritis-evaluation and outcomes. International orthopaedics 2018;42(12):2807-15.
- Gomes MG, Primo AF, De Jesus L, Dionisio VC. Short-term Effects of Mulligan’s Mobilization With Movement on Pain, Function, and Emotional Aspects in Individuals With Knee Osteoarthritis: A Prospective Case Series. Journal of manipulative and physiological therapeutics 2020;43(5):437-45.
- Westad K, Tjoestolvsen F, Hebron C. The effectiveness of Mulligan’s mobilisation with movement (MWM) on peripheral joints in musculoskeletal (MSK) conditions: A systematic review. Musculoskeletal science & practice 2019;39:157-63.
- Li LL, Hu XJ, Di YH, Jiao W. Effectiveness of Maitland and Mulligan mobilization methods for adults with knee osteoarthritis: A systematic review and meta-analysis. World journal of clinical cases 2022;10(3):954-65.
- Stathopoulos N, Dimitriadis Z, Koumantakis GA. Effectiveness of Mulligan’s Mobilization With Movement Techniques on Range of Motion in Peripheral Joint Pathologies: A Systematic Review With Meta-analysis Between 2008 and 2018. Journal of manipulative and physiological therapeutics 2019;42(6):439-49.
- Tsokanos A, Livieratou E, Billis E, Tsekoura M, Tatsios P, Tsepis E, et al. The Efficacy of Manual Therapy in Patients with Knee Osteoarthritis: A Systematic Review. Medicina (Kaunas, Lithuania) 2021;57(7).
- Ola Grimsby JR. Science, Theory and Clinical Application in Orthopaedic Manual Physical Therapy: Applied Science and Theory 2008. 556 p.
The Ziauddin University is on the list of I4OA, I4OC, and JISC.
This is an open- access article distributed under the terms of the Creative Commons Attribution License (CC BY 4.0).