
Sanjeela Abbas1, Rabiya Noor2, Muhammad Salman Bashir3, Tehreem Mukhtar4*
1Postgrade Student Riphah College of Rehabilitation & Allied Health Sciences, Lahore, Pakistan![]()
2Associate Professor, Riphah College of Rehabilitation & Allied Health Sciences, Lahore, Pakistan![]()
3Professor, Riphah College of Rehabilitation & Allied Health Sciences, Lahore, Pakistan![]()
4*Assistant Professor, Riphah College of Rehabilitation & Allied Health Sciences, Lahore, Pakistan![]()
ABSTRACT
Background: In neck related problems, limited cervical ranges are considered a major contributor leading to forward head posture and increased disability.
Methodology: The study design was a randomized clinical trial. Total of 50 subjects were recruited that fulfilled the selection criteria. Subjects were divided into two groups. Craniocervical flexion exercises group A (n=25) and Scapular stabilization exercises group B (n=25). Numeric Pain Rating Scale (NPRS) and Neck Disability Index (ND1) were subjective while the goniometer and plumb line were used as objective modes of assessment. Baseline and after 4 weeks of treatment values were assessed by using SPSS 21.
Results: Both groups showed improvement in plumb line values, forward head posture and cervical spine mobility. NPRS, and NDI score values after the 4-week exercise program showed significant results (p-value<0.05). Outcomes except for plumb line value and NDI score indicated statistically significant improvement in the Craniocervical flexion exercise group than the scapular stabilization exercise group (p-value<0.05). However, in NPRS no statistical difference (p-value>0.05) was found between the two groups.
Conclusion: Only females were recruited. Further studies can correlate with spatiotemporal features. The idea and conceptual framework were original.
Keywords: Head posture, craniocervical, flexion exercises, scapular stabilization exercises, range of motion, plumb line, neck disability index, goniometer, numeric pain rating scale, craniovertebral angle.

Introduction
Neck pain is the utmost common problem in the world. Neck pain is termed as the pain and soreness sensed usually among the first thoracic vertebra and the lower end of the occiput1,2.
Pain in the neck region may be caused due to prolonged fixed position of the head, neck, and shoulders in our activities of daily living3. Abnormalities in head posture are assumed to be linked with the persistence of neck pain, thus according to some researchers, it has a great deal of importance during the examination. In chronic neck pain, sling exercises by McKenzie treatment showed significant improvement to decrease pain, and increasing range of motion, and strength4.
Patients with neck disorders often develop a Forward head posture. Researchers reported that around 60% of patients with pain in the neck region have a forward head posture5. Pain in the neck region is more prevalent in females than males. Although, the frequency of forwarding head posture increased with prolonged disease duration which is directly related to old age, in which the range of the cervical spine is usually decreased2,6-8. Jeong-Il Kang, Hyun Ho Choi et al 2018 determined the impact of scapular stabilization exercise on the positioning of the neck and the activity of muscles that have undergone the structural alterations surrounding the neck region as a result of the forward head position. Stabilization of the scapula brings about perfection in position by stimulating the lower trapezius and the serratus anterior muscle9. In 2020 a research reported by P.Gurdut et al and postural exercise used in the treatment of asymptomatic FHP c10 Kang-Seong Lee conducted research and followed more than -month nth scapular exercise regime, modifying the position and movements of the scapula for recovery from chronic mechanical neck pain symptoms and restoration of proper neck function11. Jun Cheol Lee et al 2018, found-the-data for-developing-training regime-that-helps in improving head posture with strengthening and elongation/stretching techniques of upper extremity muscles to find their result on correcting-pose. This study showed signify results for a group who performed neck and chest extensor muscle training12 Na-Yeon Kang et al conducted a study in 2022, and their results showed that scapular stabilization exercises and thoracic extension exercises presented significant results in forward head posture and improve breathing pattern13. Joana P et al 2018 did research on the association between forwarding head posture and pressure-pain-thresholds neck pain characteristics and forward head posture among the students. A significant association was not found between pressure pain thresholds and forward head posture in the asymptomatic group. 19% of the variance of forward-head posture was noticed in the participants having pressure thresholds at the right trapezius, having neck pain. The study concluded that in asymptomatic students, forward-head posture and pressure pain threshold are not associated14. Limited researches are available to manage pain and abnormal forward head posture in this female population. In this study, Forward head posture measurements and factors for many years of worn scarves ow many hours covered per day are examined.
Methodology
A randomized clinical trial rewash registered on clinical trial.gov with clinical trial number NCT04557904. The study was conducted at the outdoor physical therapy departments of Akhtar Saeed hospital, 6 months after the approval of the synopsis. Non-probability purposive sampling was used. 50 sample sizes were taken in this study by expecting a mean pain of 31.9 ± 2.6 using 95% power of the study and 5% its level of significance15. Female age group between 20 to 40 years with a minimum duration of wear head scarves participated in this study. While on assessment Craniovertebral (CV) angle was less than 50 degrees and pain on NPRS between 4 to 6. Those subjects were excluded from having any systemic illness, history of fracture in the last 6 months, steroidal use, and neuropathic pain or nerve entrapment sign in the upper limb. Subjects were randomly divided into groups. The envelope-sealed led method was used Written consent was taken from patients before treatment. Group A subjects were treated with Craniocervical flexion exercises and the subjects in group B were treated with scapular stabilization exercises. Before treatment evaluation was completed by using NPRS and NDI as subjective measurements. For objective assessment goniometry was used for the measurement of AROM the plumb line method for measuring head posture. The last reading was taken at the end of the 4th week. The assessor was another physiotherapist who was blind after the intervention assignment. All changes recorded and saved after that were analyzed by using SPSS 25.
Results
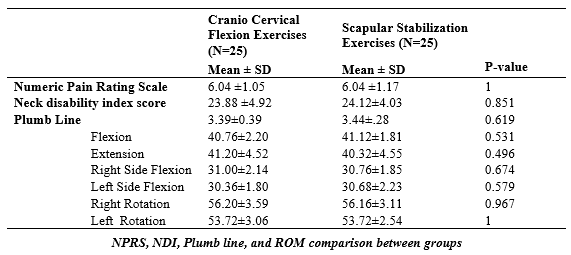
Descriptive statistics of both groups were taken. (Table 1) The collected data was normally distributed p-value was more than 0.05 then apply parametric test. An independent sample t-test was applied to compare the effect of Craniocervical flexion exercises and scapular stabilization exercises on neck pain and forward head posture improvement (Table 2). Both groups showed improvement in plumb line values (forward head posture) and cervical spine mobility (Table 3) Numeric pain rating scale (NPRS) and the Neck disability index (NDI) score values after the 4-week exercise program (p-value<0.05). All these outcomes except plumb line value and NDI score showed statistically significant improvement in the Craniocervical flexion exercise group than scapular stabilization exercise group (p-value<0.05) but no significant difference was noted between these two groups’ NPRS score values (p-value>0.05). However, within-group comparison of, plumb line value, NDI, NPRS, and cervical range of motion in all directions was calculated by paired sample t-test. The mean difference in pre-treatment and post-treatment values for both groups showed statistically significant differences for all the parameters with p-value<0.05.
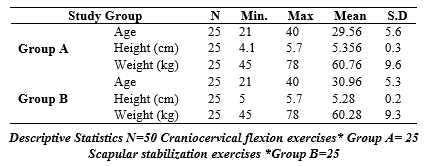
The table showed the average value of age, height, and weight of group A. Minimum age of patients in group A was 21 years and the maximum age was 40 years with a mean of 29.56 and SD of 5.64. The minimum height of patients in group A was 4.11 ft. the and maximum age of 5.70 with a mean value for height was 5.35 and SD .30, minimum weight of patients in both groups A was 45 kg and the maximum weight was 78kg with a mean of 60.76 kg and SD 9.63. However, the minimum age of patients in group B was 21 years and the maximum age was 40 years with a mean of 30.96 and SD of 5.26. The minimum height of patients in group B was 5.00 ft. and the maximum height of 5.70 with a mean value for height was 5.28 and SD .20, minimum weight of patients in both groups B was 45 kg and the maximum weight was 78kg with a mean 60.28 kg and SD 9.26.
*SD=Standard deviation
Both groups were similar in numeric pain rating scale score, neck disability index score, plumb line value and cervical functional mobility at baseline treatment values with a p-value>0.05. The mean value of the numeric pain rating score were 6.04 ±1.05 and 6.04 ±1.17 for the craniocervical flexion exercise group and scapular stabilization exercise group respectively. The mean neck disability index score was 23.88 ±4.92 for the craniocervical flexion exercise group and 24.12±4.03 for the scapular stabilization exercise group. The average value of the plumb line for the craniocervical flexion exercise group was 3.39±0.39 and 3.44±.28 for the scapular stabilization exercise group.
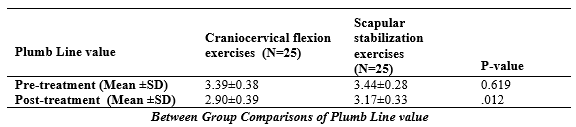
An independent sample T-test was applied to measure any significant difference between Pre and Post Treatment values of a plumb line. The results showed that there was a statistically significant difference between the two groups with a p-value < 0.05, but there was a greater reduction in plumb line value was measured in the craniocervical flexion exercise group (group A) with a mean and SD 2.90±0.39 as compared to scapular stabilization exercise group (group B) with mean and SD 3.17±0.3.
Discussion
The current study indicated that cervical ranges were limited especially in left and right rotation and extension. Moreover, the greater increase in NPRS and NDI scores is seen in females who use to wear the head scarves 8 or 10 hours daily regularly but the number of years wearing the headscarf, use of under hijab cap, and hijab volume don’t show the statistically significant difference in cervical range of motion limitation, NPRS, and NDI scores. The limitation of this study is that duration was short a four weeks exercise program, which cannot describe the long terms effects of these exercises. Muscle energy techniques and stabilization exercises were effective to increase mobility of forward head posture and rounded shoulder16 However, the age of onset of wearing a head scarf and number of years worn showed no statistically significant difference in cervical spine range15 Thus, prolonged use of wearing a head scarf may result in adaptive shortening of muscles and changes in the neck posture. Neck mobility can be restricted due to the daily use of a head scarf, which may act as a physical barrier to a cervical range of motion which is quite similar to the results of Dunleavy K et al17 Cht yip et al. determined that increased forward head posture ratio was seen in patients with decreased Craniovetebral angle, therefore, increase in forwarding head posture increase the disability18. The results of this study revealed that females wearing head scarves show a decrease in Craniovetebral angle or neck range of motion as measured by a cervical goniometer which is supported by the findings of the Lopez et al. study. They measured the head posture in the standing position of patients with and without neck pain. They found that individuals with neck pain have decreased Craniovetebral angle than pain-free individuals19.The subjects with insidious onset of pain while having a history of chronic neck pain f out the left rotation restriction as in this study20. In addition, Lee et al. reported the significantly reduced left-side rotation of the neck in young participants with neck pain21. Jull et al. conducted the study which included 40 patients with chronic neck pain, divided into two treatment groups. Deep cervical flexion exercises were allocated to group 1 and simple neck-bending exercises were allocated to group 2. The results of that study are in good agreement with the results of the present study showing that greater improvements in NDI and NPRS scores were reported in both groups after four weeks of follow-up. However, the effects of deep cervical flexion exercises were more beneficial in reducing pain and improving the functional status of patients with neck pain as compared to simple bending exercises22. 6 weeks deep cervical flexion exercise program for the participants with neck/cervical pain and substantial decrease in NDI score. They concluded that after eight weeks of follow-up, the NDI score in the deep cervical flexion exercise group was significantly improved23. In this study, the craniocervical flexion exercises as compared to scapular stabilization exercises show better improvement in neck pain and forward head posture in females wearing headscarves. A study conducted with 8-week follow-up program for subjects with chronic neck pain who had undergone either generalized strengthening exercises for the cervical spine or deep cervical flexors activation exercises for four weeks and assessed the related parameters like neck pain, neck/shoulder posture, and functional status before 4 weeks and then after the 8 weeks to compare those parameters. The result of their study indicated that neck pain, neck/shoulder posture, and NDI score were substantially improved in both groups after four weeks of exercise24. Kang J-I et al. 2018 suggested scapular stabilization exercises for the treatment of problems related to the neck scapula, and upper back. According to their study results, forward head posture caused by structural derangements and muscles producing the compensatory movements of the neck can be effectively improved by scapular stabilization exercises same in the present study, the scapular stabilization exercises are shown to improve the Craniovertebral angle or cervical range of motion in all directions thus relieving the neck pain and correcting the forward head posture9. Wegner et al. prescribed scapular stabilization exercises to 38 patients with neck pain because of the long-term use of technology especially computers. Their study concludes that these exercises may alter the activity of the trapezius muscle thus helping in reducing neck pain25. Muscle stiffness and positional faults around the scapular and neck areas and forward head posture can be improved by scapular stabilization exercises. Their study concluded that strengthening the weak muscles like the serratus anterior and lower trapezius and inhibiting the over-activation of the upper trapezius muscle and enhancing the controlled use of serratus anterior and upper trapezius muscles bring back the scapular and thoracic scapular positions near to normal from forward head posture26. A study investigated that scapular stabilization exercise may have beneficial impacts on muscle activation, craniovertebral angle, and cranial rotation angle. These exercises change asymmetric muscle activation patterns5. While the current study is also supporting these aspects.
Conclusion
Craniocervical flexion exercises are more effective in improving neck pain and forward head posture than scapular stabilization exercises among females wearing headscarves.
Recommendations
The only female population was involved in the study. Future research can be conducted on advanced levels including different areas and more population.
AUTHORS’ CONTRIBUTION:
The following authors have made substantial contributions to the manuscript as under:
Conception or Design: Sanjeela Abbas
Acquisition, Analysis or Interpretation of Data: Muhammad Salman Bashir
Manuscript Writing & Approval: Tehreem Mukhtar
All authors acknowledge their accountability for all facets of the research, ensuring that any concerns regarding the accuracy or integrity of the work are duly investigated and resolved.
ACKNOWLEDGEMENTS: I extend my sincere appreciation to all individuals who contributed to the successful completion of the manuscript.
INFORMED CONSENT: Yes
CONFLICT OF INTEREST: No
FUNDING STATEMENTS: No
ETHICS STATEMENTS: The protocol of the present study was registered by the local ethics committee of RIPAH INTERNATIONAL UNIVERSITY APPROVAL CODE Ripah/RCRS/REC/18/1006/registered in clinicaltrial.gov NCT04557904
References
- Nejati P, Lotfian S, Moezy A, Moezy A, Nejati M. The relationship of forward head posture and rounded shoulders with neck pain in Iranian office workers. Medical journal of the Islamic Republic of Iran 2014; 28:26.
- Lindstrøm R, Schomacher J, Farina D, Rechter L, Falla D. Association between neck muscle coactivation, pain, and strength in women with neck pain. Manual therapy. 2011;16(1):80-6.
- Motialla T, Haghighi FM, Ghanbari A, Moezi SA, Saadat Z. The correlation between forward head posture and trigger points in trapezius muscle in subjects with chronic neck pain. Journal of Research in Rehabilitation Sciences. 2013;8(6): 989-97.
- Seo SC, Choi JY, Joo MY, Kim JH, Chang SK. Effects of sling exercise and McKenzie exercise program on neck disability, pain, muscle strength and range of motion in chronic neck pain. Physical Therapy Rehabilitation Science 2012;1(1):40-8.
- Im B, Kim Y, Chung Y, Hwang S. Effects of scapular stabilization exercise on neck posture and muscle activation in individuals with neck pain and forward head posture. Journal of physical therapy science 2015;28(3):951-55.
- Demaille-Wlodyka S, Chiquet C, Lavaste JF, Skalli W, Revel M, Poiraudeau S. Cervical range of motion and cephalic kinesthesis: ultrasonographic analysis by age and sex. Spine. 2007;32(8): 254-61.
- Fejer R, Kyvik KO, Hartvigsen J. The prevalence of neck pain in the world population: a systematic critical review of the literature. European spine journal. 2006;15(6): 834-48.
- Chiu TTW, Law EYH, Chiu THF. Performance of the craniocervical flexion test in subjects with and without chronic neck pain. Journal of Orthopaedic & Sports Physical Therapy 2005;35(9): 567-71.
- Kang JI, Choi HH, Jeong DK, Choi H, Moon YJ, Park JS. Effect of scapular stabilization exercise on neck alignment and muscle activity in patients with forward head posture. Journal of Physical Therapy Science 2018;30(6): 804-8.
- Gurudut P, Welling A, Chodankar A. Effect of self-care exercises in forward head posture on craniovertebral angle and craniocervical flexion endurance: A pilot study. Indian Journal of Physical Therapy and Research. 2020;2(1): 25.
- Lee KS. Effect of a Five-week Scapular Correction Exercise in Patients with Chronic Mechanical Neck Pain. The Journal of Korean Physical Therapy 2020;32(2):126-31.
- Lee JC. Effect of strengthening and elongation exercises of upper extremity muscle to forward head posture correction. International journal of advanced smart convergence. 2018;7(1):33-41.
- Kang NY, Kim K. Effects of a Combination of Scapular Stabilization and Thoracic Extension Exercises on Respiration, Pain, Craniovertebral Angle and Cervical Range of Motion in Elementary School Teachers with a Forward Head Posture: A Randomized Controlled Trial. Korean Society of Physical Medicine 2022;17(2):29-40.
- Pacheco J, Raimundo J, Santos F, Ferreira M, Lopes T, Ramos L, et al. Forward head posture is associated with pressure pain threshold and neck pain duration in university students with subclinical neck pain. Somatosensory & Motor Research 2018;35(2): 103-8.
- Alqabbani S. The Effects of Wearing Headscarves on Cervical Spine Proprioception and Range of Motion. Bains G, Daher, Noha S.Johnson, Eric, , editor: Loma Linda University Libraries; 2017.
- Kaliyaperumal AB, Sekar K, Manickavelu P, Senthilmurugan S. Effect of Muscle Energy Technique and Stabilization Exercise on Forward Neck and Rounded Shoulder for Elite Swimmers. Indian Journal of Physiotherapy & Occupational Therapy Print-(ISSN 0973-5666) and Electronic–(ISSN 0973-5674) 2023;17(1):1-6.
- Dunleavy K, Goldberg A. Comparison of cervical range of motion in two seated postural conditions in adults 50 or older with cervical pain. Journal of Manual & Manipulative Therapy 2013;21(1):33-9.
- Yip CHT, Chiu TTW, Poon ATK. The relationship between head posture and severity and disability of patients with neck pain. Manual therapy 2008;13(2):148-54.
- Lopez-de-Uralde-Villanueva I, Beltran-Alacreu H, Paris-Alemany A, Angulo-Diaz-Parreno S, La Touche R. Relationships between craniocervical posture and pain-related disability in patients with cervico-craniofacial pain. Journal of pain research. 2015;8: 449-58.
- Sjölander P, Michaelson P, Jaric S, Djupsjöbacka M. Sensorimotor disturbances in chronic neck pain—range of motion, peak velocity, smoothness of movement, and repositioning acuity. Manual therapy 2008;13(2):122-31.
- Lee H, Nicholson LL, Adams RD, Bae S-S. Proprioception and rotation range sensitization associated with subclinical neck pain. Spine 2005;30(3): 60-7.
- Jull G, Falla D, Vicenzino B, Hodges P. The effect of therapeutic exercise on activation of the deep cervical flexor muscles in people with chronic neck pain. Manual therapy 2009;14(6):696-701.
- Kim JC, Yi CH, Kwon OY, Oh DW, Jeon HS. Strength and endurance of the deep neck flexors of industrial workers with and without neck pain. Journal of the Ergonomics Society of Korea 2007;26(4):25-31.
- Kim JY, Kwag KI. Clinical effects of deep cervical flexor muscle activation in patients with chronic neck pain. Journal of physical therapy science 2016;28(1):269-73.
- Wegner S, Jull G, O’Leary S, Johnston V. The effect of a scapular postural correction strategy on trapezius activity in patients with neck pain. Manual therapy 2010;15(6): 562-6.
- Kim D, Cho M, Park Y, Yang Y. Effect of an exercise program for posture correction on musculoskeletal pain. J Phys Ther Sci 2015; 27(6):1791-4.
The Ziauddin University is on the list of I4OA, I4OC, and JISC.
This is an open- access article distributed under the terms of the Creative Commons Attribution License (CC BY 4.0).