
Nimra Basit 1, Hafiza Neelam Muneeb2*, Dr. Muhammad Amir3, Kinza Mazhar4
1Student, Riphah International University, Lahore, Pakistan![]()
2*Senior Lecturer, Riphah International University, Lahore, Pakistan![]()
3Ex-Registrar Pediatric Surgery, Children Hospital & ICH Lahore, Pakistan![]()
4Student, Riphah International University, Lahore, Pakistan![]()
ABSTRACT
Background of the Study: To compare the effects of cervical muscles strengthening with and without shoulder exercises on post- mastectomy patients with neck pain.
Methodology: It was a randomized clinical trial, conducted in physical therapy department of a clinical setting through Dynamometer. Sample size of 24 patients were taken. Non-probability convenience sampling technique was used. A written consent form was taken from patients meeting inclusion criteria and were randomly allocated. In one group, patients were treated with cervical Muscles strengthening with shoulder exercises. In other group, patients were treated with cervical Muscles strengthening alone. Treatment was given once a day for three weeks. Muscle strength was examined using dynamometer, Baseline data was taken before treatment on first day after inclusion in study and again on the last day after treatment. SPSS 25 was used to analyze the data.
Results: Wilcoxon signed rank test was used to compare individuals within the group which showed significant results in both groups, p-value 0.000 (i.e. <0.001) for neck strength. Between groups comparison was done using Mann-Whitney U Test and it showed no significant changes for cervical extensors (p- value;0.143) , cervical side bending (right) (p-value; 0.315) and cervical side bending (left) (p-value; 0.853) strength differences, but however cervical flexors strength showed statistically significant results as p-value was 0.003.
Conclusion: It was concluded that Cervical strengthening along with shoulder Rehabilitation can help improve the strength of cervical flexors. However, both the groups have equally resulted in improved cervical extensor, Side bending right and left strength.
Keywords: Cervical, mastectomy, muscle strength, rehabilitation, exercises, therapeutic.

Introduction
Breast cancer is the most common cancer in women and the leading cause of cancer death in women worldwide1,2. Each year, more than 1.5 million women worldwide that is, 25% of all cancer patients, are diagnosed with breast cancer3. Breast cancer is the second leading cause of cancer deaths among women4,5. Globally, the survival rate of breast cancer patients’ vary greatly, with developed countries having an estimated 5-year survival rate of 80 percent and developing countries having a rate of less than 40 percent6. Mastectomy is common therapeutic option in treating breast cancer7. Breast conserving therapy (BCT) and mastectomy have equivalent chances of survival in early-stage breast cancer and can be considered treatments of the same nature8. However, the consequences of surgery resulted in a practical limitation of several movements, and changes in scapular kinematics, muscle strength loss, axillary sensory loss, shoulder joint movement limitations, postural changes, and axillary web syndrome, which have acquired special attention in recent years9,10. A variety of conditions, such as axillary web syndrome, adhesive capsulitis, myofascial dysfunction, brachial plexopathy, and rotator cuff injury, can become a risk for patients later in their life following breast cancer surgery11,12. Each one of these factors can lead to practical impairments such as lymphatic function, reduced range of motion, and muscular strength, and pain in the shoulder13,14. A clinically significant post-operative consequence following a mastectomy is pain15. An aching and cramping like pain myofascial pain seldom occurs in cancer patients. The pain is normally difficult to locate and may be confused with other deep somatic structures. Lack of activity is common in advanced stages of carcinoma, which is likely to develop muscle pain16. A significant difference between pain and its severity was observed between the lumpectomy and mastectomy groups. Females of both groups indicated discomfort in shoulder and neck region, however the severity of the pain was greater in the mastectomy group17. Furthermore, the intensity of self – reported neck and shoulder/axillary pain was related to greater hypersensitivity in the mastectomy group17. Post mastectomy pain patients complained of trigger point activation in the upper trapezius, sternocleidomastoid, sub occipital, levator scapulae, scalene, infraspinatus, and pectoralis major muscles18,19. Following, mastectomy there is a shift in distribution of weight, which disrupts trunk posture and, consequently, can affect neck posture20. The development of scarring or compensatory posture because of muscle weakening might impair upper extremity alignment. Treatments can affect function by reducing muscle strength and physical function21,22. The cervical issues although persists in later stages, however the effect of strengthening the cervical muscles in the context of management of pain sensitivity and improvement of function is not yet substantially explored. However, this study is focused on secondary complication that is cervical pain in later stages of post mastectomy patients. Previous researches were conducted on shoulder rehabilitation and cervical strengthening. These techniques are separately addressed in previous evidence. According to knowledge of the researcher, cervical strengthening along with shoulder has not yet been addressed in post mastectomy patients.
Methodology
This randomized clinical trial study was conducted in 2021 at physical therapy department, Lahore. Ethical approval was received for the present study from Institutional Review Board (IRB) of Riphah International University Lahore (IRB reference # F19C14G30003). All participants in the study gave their written, informed consent. Sample size was calculated from online calculator. It was estimated that 13 patients were needed for each of our two groups. The inclusion criteria of the study was Females who have undergone mastectomy with age group between 30 – 65 years, Females with neck pain, Post mastectomy patients with no signs of recurrence. However, following patients were excluded which are having history of trauma, cancer or fracture in cervical spine. Previous history of fibromyalgia or Cervical Radiculopathies were also excluded from the study. Each patient who was recruited in the study signed the consent form and the baseline measurements were taken in the beginning. The dynamometer was used to measure the muscle strength of Cervical Flexors, Cervical Extensors, Cervical side bending (right) and (left). Non-probability convenience sampling technique was used and participants were allocated to Group A and Group B randomly, using lottery method. Group A received Cervical strengthening with Shoulder Rehabilitation exercises. Prior to the treatment an ultrasound therapy to the cervical area was given to the patient for 7 minutes. Afterwards, the patient performed Cervical Range of motion exercises in each plane for 5 times. Then, neck isometrics were performed in all planes (i-e flexion, extension, side bending and rotation) for 10 repetitions. Patient was in seated position with their feet flat on the floor and shoulder relaxed. Patient was asked to resist their neck muscles against therapist hand on their forehead. Hold for 10 seconds. Relax. Repeat 10 times. Patient was asked to resist again by pressing against side of their head. Repeat 10 times. Switch sides. Repeat 10 times. The patient was additionally given the shoulder Rehabilitation exercise which included walking fingers up the wall, lifting arm above the head, elbow push back exercise, shoulder external rotation, flexion, and extension exercises. Each exercise was performed for 5 repetitions each. Group B received cervical strengthening. Prior to the treatment, an ultrasound therapy was given to the patient for 7 minutes. Afterwards, the patient performed Cervical Range of motion exercises in each plane for 5 times. Then, neck isometrics were performed in all planes (i-e flexion, extension, side bending and rotation) for 10 repetitions. Patient was in seated position with their feet flat on the floor and shoulder relaxed. Patient was asked to resist their neck muscles against therapist hand on their forehead. Hold for 10 seconds. Relax. Repeat 10 times. Patient was asked to resist again by pressing against side of their head. Repeat 10 times. Switch sides. Repeat 10 times. Data was collected by a valid tool i.e. Dynamometer to measure the muscle strength. Furthermore, it was made sure that this data would be utilized for research, quality assurance, and academic purposes. Data was acquired from participants after obtaining written informed consent from the enrolled patients. It was noted that the participants’ identities would be concealed, and that the data would not be able to be traced back to the participants included in the study. After collecting the data, normality of the study was done through Shapiro Wilk test and since the data was not normally distributed Non-Parametric tests were applied. . Data analysis was carried out using both Microsoft Office Excel 2010 and SPSS version 25. Descriptive statistics were employed. Using inferential statistics, Wilcoxon sign rank and Man Whitney U tests were applied to compare results within the groups and across two groups. Findings were statistically significant at a p-value < 0.05
Results
Within groups analysis was done through Wilcoxon sign-rank test and statistically, Group A showed significant improvement in muscle strength of Cervical Flexors, Extensors, and side bending (Right) and (left) as p-value of each muscle strength group was <0.05 Since p-value among all the groups is <0.05; therefore, within the group’s results were statistically significant. Conversely, between groups analysis showed the statically significant results for cervical flexors muscle groups, however; cervical extensors, side flexors both right and left muscle groups exhibited insignificant results across the groups.
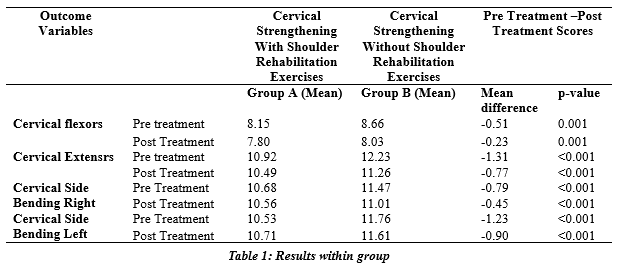
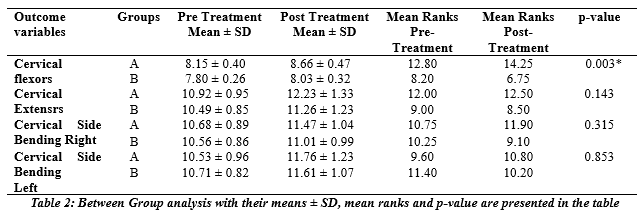
*p-value<0.05; results are statistically significant for Cervical Flexors muscle strength across the group
Discussion
The present study analyzed the comparison of the effectiveness of Cervical Strengthening with and without Shoulder Rehabilitation exercises. This study found that within groups, results showed significant improvement in muscle strength in both the groups. However, in between groups’ comparisons, the results showed significant difference cervical muscles (flexor) strength, with no significant improvement in rest of cervical muscles strength. JT Eckner et al investigated the feasibility and effects of cervical resistance training on head kinematics in young athletes. The results of the study indicated that neck strength was increased in both experimental and control group. However, the results showed neck strength to be 2.6 times greater than in control group. It’s unclear whether the control group’s considerably lower increases in neck strength were due to indirect effects of the general resistance training exercises they did or just age-related effects of normal growth and maturation. 23 The study conducted in post mastectomy patients, showed the similar results as cervical strength was greatly improved in both experimental and control groups with significant improvement in cervical flexors strength in experimental group. Raju, Addala Suvarna et al conducted a comparative study on deep cervical flexors training and neck stabilization exercises in subjects with chronic neck pain. The results of the study revealed that among groups, there was a substantial improvement in all factors, but between group comparisons revealed significant improvements in the third week and highly significant improvements in the fourth week. In participants with persistent neck pain, deep cervical flexors exercise reduced pain intensity, functional impairment, and improved muscular strength.24.The results of the study indicated that cervical strengthening exercises with and without shoulder Rehabilitation program has resulted in considerable increase in patients’ cervical muscular strength. IH Lin et al studied the progressive effects of neck-shoulder exercise and the results indicated that the experimental group had an improvement in performance index of the cranio-cervical flexion test, with improvement in superficial neck flexor strength, superficial neck extensor strength after the intervention, indicating that the 6-week intervention influenced the improvement of cervical muscle functions significantly. 25 The current study, however, indicated that with an invention program of 3-weeks with neck strengthening and shoulder Rehabilitation exercise has significantly improved the strength of cervical muscles. The major limitation of this study was that because of the on-going situation of Covid-19, there was limited access to patients, which can be a reason for dropout. In addition, long term follow up was not continued. For further studies, there is a need to explore larger population for deductive reasoning to implement results, also, long-term effects needed to be studied so that effects of strengthening can further implement results in the functional outcome of patients.
Conclusion
It is concluded that that cervical strengthening along with Shoulder Rehabilitation Exercises can help in improvement of strength of cervical flexors. However, both treatment groups have equally improved patients’ strength of cervical extensors and side bending right and left muscle groups.
AUTHORS’ CONTRIBUTION:
The following authors have made substantial contributions to the manuscript as under:
Conception or Design:
Acquisition, Analysis or Interpretation of Data:
Manuscript Writing & Approval:
All authors acknowledge their accountability for all facets of the research, ensuring that any concerns regarding the accuracy or integrity of the work are duly investigated and resolved.
ACKNOWLEDGEMENTS: The authors are extremely grateful to all the participants of this study who took out time from their hectic schedules and gave honest feedback. We acknowledge the co-operation of the research department of both the institutions.
INFORMED CONSENT: Written Informed Consent was taken from each patient.
CONFLICT OF INTEREST: The author (s) have no conflict of interest regarding any of the activity perform by PJR.
FUNDING STATEMENTS: None declared
ETHICS STATEMENTS: The study has been approved by the Ethical Board of Lahore College of Physical Therapy LCPT/DPT/16/631.
References
- Chang PJ, Asher A, Smith SR. A Targeted Approach to Post-Mastectomy Pain and Persistent Pain following Breast Cancer Treatment. Cancers 2021;13(20):5191.
- Ortiz-Comino L, Fernández-Lao C, Castro-Martín E, Lozano-Lozano M, Cantarero-Villanueva I, Arroyo-Morales M, et al. Myofascial pain, widespread pressure hypersensitivity, and hyperalgesia in the face, neck, and shoulder regions, in survivors of head and neck cancer. Supportive Care in Cancer 2020;28(6):2891-8.
- Bender E. Developing world: global warning. Nature 2014;509(7502):S64-S5.
- Leitner A, Chang C, editors. Fundamentals of Cancer Pain Management. Springer International Publishing 2021.
- Mur‐Gimeno E, Postigo‐Martin P, Cantarero‐Villanueva I, Sebio‐Garcia R. Systematic review of the effect of aquatic therapeutic exercise in breast cancer survivors. European Journal of Cancer Care 2021.
- Berrino F, Lutz J, De Angelis R, Rachet B, Gatta G. Cancer survival in five continents: a worldwide population-based study (CONCORD).
- Sheppard LA, Ely SJTBJ. Breast cancer and sexuality 2008;14(2):176-81.
- Gu J, Groot G, Boden C, Busch A, Holtslander L, Lim HJCbc. Review of factors influencing women’s choice of mastectomy versus breast conserving therapy in early stage breast cancer: a systematic review. Clinical breast cancer 2018;18(4):e539-e54.
- Yeung WM, McPhail SM, Kuys SS. A systematic review of axillary web syndrome (AWS). Journal of Cancer survivorship: research and practice 2015;9(4):576-98.
- da Silva FP, Moreira GM, Zomkowski K, de Noronha MA, Sperandio FF. Manual therapy as treatment for chronic musculoskeletal pain in female breast cancer survivors: a systematic review and meta-analysis. Journal of manipulative and physiological therapeutics 2019;42(7):503-13.
- Ezzati K, Laakso E-L, Salari A, Hasannejad A, Fekrazad R, Aris A. The beneficial effects of high-intensity laser therapy and co-interventions on musculoskeletal pain management: a systematic review. Journal of lasers in medical sciences 2020;11(1):81.
- Kannan P, Lam HY, Ma TK, Lo CN, Mui TY, Tang WY. Efficacy of physical therapy interventions on quality of life and upper quadrant pain severity in women with post-mastectomy pain syndrome: A systematic review and meta-analysis. Quality of Life Research 2022;31(4):951-73.
- Ozyemisci-Taskiran OJPp. Ultrasound-guided block of the suprascapular nerve in breast cancer survivors with limited shoulder motion–case series. 2017;20:E233-E9.
- Yang A, Sokolof J, Gulati A. The effect of preoperative exercise on upper extremity recovery following breast cancer surgery: a systematic review. International Journal of Rehabilitation Research. 2018;41(3):189-96.
- Haroutiunian S, Nikolajsen L, Finnerup NB, Jensen TS. The neuropathic component in persistent postsurgical pain: a systematic literature review. PAIN® 2013;154(1):95-102.
- Bulbule A. Effectiveness of Rhythmic Chopping & Lifting Pattern on Shoulder Range of Motion and Upper Extremity Functional Index in Post: Mastectomy Patients. Indian Journal of Public Health Research & Development 2020;11(2).
- Fernández-Lao C, Cantarero-Villanueva I, Fernández-de-las-Peñas C, Del-Moral-Ávila R, Menjón-Beltrán S, Arroyo-Morales M. Widespread mechanical pain hypersensitivity as a sign of central sensitization after breast cancer surgery: comparison between mastectomy and lumpectomy. Pain medicine 2011;12(1):72-8.
- la R, Arendt-Nielsen L, Arroyo-Morales M. Myofascial trigger points in neck and shoulder muscles and widespread pressure pain hypersensitivtiy in patients with postmastectomy pain: evidence of peripheral and central sensitization. The Clinical journal of pain 2010;26(9):798-806.
- Ge H-Y, Fernández-de-Las-Peñas C, Madeleine P, Arendt-Nielsen L. Topographical mapping and mechanical pain sensitivity of myofascial trigger points in the infraspinatus muscle. European Journal of Pain 2008;12(7):859-65.
- Rostkowska E, Bak M, Samborski W. Body posture in women after mastectomy and its changes as a result of rehabilitation. Adv Med Sci 2006;51(1):287-97.
- Ebaugh D, Spinelli B, Schmitz KH. Shoulder impairments and their association with symptomatic rotator cuff disease in breast cancer survivors. Medical hypotheses 2011;77(4):481-7.
- Giordano S, Kääriäinen M, Alavaikko J, Kaistila T, Kuokkanen H. Latissimus dorsi free flap harvesting may affect the shoulder joint in long run. Scandinavian Journal of Surgery 2011;100(3):202-7.
- Eckner JT, Goshtasbi A, Curtis K, Kapshai A, Myyra E, Franco LM, et al. Feasibility and effect of cervical resistance training on head kinematics in youth athletes: a pilot study. American journal of physical medicine & rehabilitation 2018;97(4):292.
- Raju AS, Apparao P, Swamy G, Chaturvadi P, Mounika RG. A comparative study on deep cervical flexors training and neck stabilization exercises in subjects with chronic neck pain. Indian Journal of Physiotherapy & Occupational Therapy 2019;13(2).
- Lin IH, Chang K-H, Liou T-H, Tsou C-M, Huang Y-C. Progressive shoulder-neck exercise on cervical muscle functions in middle-aged and senior patients with chronic neck pain. European journal of physical and rehabilitation medicine 2017;54(1):13-21.
The Ziauddin University is on the list of I4OA, I4OC, and JISC.
This is an open- access article distributed under the terms of the Creative Commons Attribution License (CC BY 4.0).