
ABSTRACT
AIMS & OBJECTIVES
The aim of this study is to evaluate and compare the effects of Short-Arc and Isometric Quadriceps exercises on Quadriceps strength and health related quality of life among Anterior Knee pain patients by using EMG biofeedback.
METHODOLOGY
Total 80 participants were recruited and randomly distributed in two groups; A and B. Individuals in group A performed isometric quadriceps exercise while group B participants performed short-arc exercise for 1st, 6th and 8th week along with a home exercise programme. Pre and post treatment assessment was performed using EMG Biofeedback, VAS, and KUJALA scoring questionnaire. Statistically, data was analysed using SPSS version 20.
RESULTS
After 8 weeks, EMG Biofeedback revealed the higher effectiveness short-arc exercises with value 88.20mv ± 6.64 comparing isometric quadriceps exercises. Moreover, Wilcoxon rank test revealed statistically significant improvement in VAS score with p-value <0.05. Furthermore, KUJALA score also advocated the effectiveness of short-arc exercises with statistically significant values (p-value < 0.05).
CONCLUSION
The study concluded the effectiveness of Short-arc quadriceps exercises comparing to static-quadriceps exercises in improving muscles strength, pain and health related quality of life after 8 weeks of intervention.
KEYWORDS
Quadriceps Muscles, Vastus Lateralis, Vastus Medialis, Knee Joint, Pain, Health-Related Quality of Life.
Muhammad Shahrukh Abbasi
Assistant Professor
Ziauddin College of Rehabilitation Sciences
Ziauddin University [email protected]
doi.org/10.36283/pjr.zu.9.1/006
Syed Abid Mehdi Kazmi Associate Professor Dr. Ziauddin Hospital [email protected]
Nabeel Baig
Assistant Professor
Ziauddin College of Rehabilitation Sciences Ziauddin University [email protected]
[Abbasi MS,Kazmi SAM,Baig N. Effectiveness of Short Arc and Isometric Quadriceps Exercises on Pain, Muscle Activity and Health Related Quality of Life in Patients with Anterior Knee Pain Pak.j.rehabil. 9(1);2020 41-46]
This is an open-access article distributed under the terms of the Creative
Commons Attribution Licence (CC BY) 4.0 https://creativecommons.org/
Anterior Knee pain is considered as one of the common problems dealt by the clinicians in the outpatient department with an estimated prevalence of around 15-45%1. Moreover, 11-17% of both physically active and sedentary individuals are suffering from anterior knee pain, especially adolescents where almost 50% of individuals continue to complain about knee pain for almost a year, subsequently affecting their quality of life and academic performance2. Interestingly, female gender is four times more prevalent as compared to males ultimately leading to degeneration of joint and an increase in Q-angle3. Patellofemoral Pain (PFP) is generally felt in front of the knee, associated with activities such as ascending and descending stairs, squatting and other similar activities4. Even though conservative medical treatment is found to be a first line of choice among people, yet physical therapy interventions and exercises turn out to be vital to maximise the chances of recovery5. According to research conducted by the US NAVY, anterior knee pain is a common problem in adolescents and in adults. The prevalence of this disorder among young adults varies from 7% to 15% in adults and it also constitutes 5% of all injuries and 25% of knee injuries. It is more common in females than males6. Isometric quadriceps exercises have a greater impact on decreasing the level of pain, enhancing muscle activity and increasing the functional status of knee pain patients7, whereas the short arc quadriceps exercises enhance the health related quality of life by decreasing the level of Patellofemoral pain, strengthen quadriceps muscle more effectively and efficiently8.
According to the studies, about half of the adult population complains of knee pain and incurred substantial cost in the healthcare system. One out of every six individuals have a medical appointment annually, out of which one-third may develop a disability9. The parameters of assessment includes Visual Analog Scale, Kujala Scoring Questionnaire and EMG Biofeedback9. EMG biofeedback machines have a potential benefit for both clinician and patients during muscle retraining programmes, the results obtained from EMG biofeedback during rehabilitation appears promising, though less researches have been done in this regard.9 Frequency parameters of EMG Biofeedback in Patellofemoral pain presented greater reliability, diagnostic accuracy and is a useful tool to diagnose individuals with Patellofemoral pain syndrome10. To measure pain intensity, the comparable tools are Verbal Rating Scale (VRS) and Numerical Rating Scale (NRS). Reliability was analysed in subgroups of 250 patients after an hour, statistical analysis present high reliability and validity (r>0.8; p< 0.01) for all tools, also the mean values of all scales present a higher association. In results, it shows high reliability and concurrent validity for VAS, NRS and VRS11. The visual analogue scale is a reliable tool for measuring pain in adults with MSK, Orthopedics and in Geriatric groups. Parameters of reliability were measured using interclass correlation coefficient (ICC) and validity measured using Bland-Altman graphs and correlations12. Kujala scoring questionnaire is a reliable assessment tool for Patellofemoral pain syndrome to assess the health related quality of life13.
Study Setting
The study was conducted in Department of Rehabilitation Sciences Ziauddin Hospital, Clifton, Karachi.
Target Population
Patients suffering with Anterior Knee Pain.
Study Design
Randomised Control Trial.
Sample Selection
Simple Random Sampling Technique.
Selection Of Patients
Inclusion Criteria
The patients aged between 16-40 years was with Anterior Knee Pain referred to department of Rehabilitation Sciences.
Exclusion Criteria
Those patients with recent surgery in the hip, knee and back, history of skin infection, positive instability test indicative of ligamentous tear, metal allergy, and positive meniscal tear test were excluded from the study.
Moreover, presence of bilateral Knee pain, recurrent patellar subluxation or dislocation, previous surgery to the knee joint, patient’s with referred pain to the knee, non-compliance, osteoporosis, and those with the inability to perform the prescribed exercises were also excluded.
Data Collection Procedure
The participants recruited in the study were divided into two groups A (n=40) and B (n=40). Group A received Isometric Quadriceps exercises whereas Group B received Short arc quadriceps exercises. Each group received interventions for one week under the supervision of expert physical therapists including traditional physical therapy (hot packs, cold packs, and electrotherapy). Moreover, the exercise regime was followed by 7 weeks of a home exercise programme and a weekly visit to the physiotherapy department for assessment was mandatory to ensure that recommended exercises are not increasing the pain or worsening the condition. A total 8 weeks of exercise therapy programme and assessments using EMG biofeedback, Kujala Scoring Questionnaire and Visual Analogue Scale (VAS) were performed.
Group-A: Isometric Quadriceps Exercises Group-A received Isometric Quadriceps exercise for 8 weeks (at least 1 session/week under the supervision of a physiotherapist) and regular home-based programme. The frequency of sets of 10 repetitions; with an initial dosage: 1 set of exercise performed twice a day for the 1st week.
For advance training, 2 sets with 10 repetitions per set, twice a day for 2nd and 3rd week followed by 3 sets with 10 repetitions per set, twice a day till 4th to 8th week. The patient was advised to lie in a supine position where the towel is to be placed under the knee joint. A towel is then compressed by applying downwards pressure on knee joint without elevating foot.
Group-B: Short Arc Exercises
Group-B received short arc Quadriceps exercise for 8 weeks for at least 1 session per week under the supervision of a physiotherapist and regular home exercise. The initial dosage was 3 sets with 10 repetitions per set for first three weeks. In the advance training, 3 sets with 20 repetitions per set from 3rd to 8 weeks. Patient was in supine lying position where a bolster was placed under the knee joint. Patient was asked to lift the heels keeping knee extended and ankle is in dorsiflexion while pressing the pillow. Position was to be maintained for 3 to 5 seconds, and then slowly returned to the starting point.
The pre and the post assessment of pain, muscle activity and health related quality of life of the participants recruited in this study was assessed by using Visual Analog Scale, EMG biofeedback and KUJALA assessment form respectively.
A total of 80 patients included in the study were divided into two groups (n=40). The demographic details including age and gender were recorded where majority of females were included in both the groups (Group A: n=35, Group B: n=38). The mean age of the participants in group A and B was found to be 29.47±6.16 and 31.46±7.47 respectively.
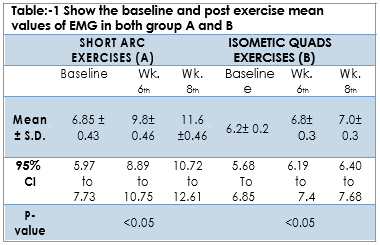
Repeated Measures Analysis of Variance was applied to determine the with-in group analysis at baseline, 6th week and 8th week (Table: 1). Improvement was observed both in group A and B, although the mean difference was found to be significant in groups.
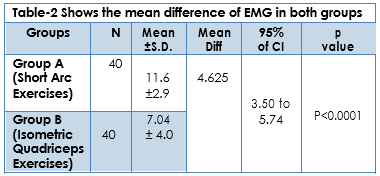
Within the group analysis of the effects of both short arc and isometric quadriceps on EMG of the patients were determined at 95% of Confidence Interval. The normality of the data was identified using Skweness and kurtosis test that confirmed the data is found to be normally distributed. The results revealed that the average mean value of EMG of the participants of Group A (short arc) at Baseline was found to be 6.85± 0.43 that improved at week 6, 9.8±0.46 whereas, improvement was further continued till the 8th Week 11.6±0.46 (Table-2).
The results of Group B (i.e.) Isometric quadriceps exercises also improved till 8th week. However the average mean value of EMG of the participants of Group B at Baseline was found to be 6.2±0.2 that improved at week 6.8±0.3 whereas improvement was further continued till the 8th Week 7.0±0.3. Table 3.
Wilcoxon Rank Test
The values of Wilcoxon rank test shows that after comparing the values for the 8th week, there will be a marked decrease of pain level as compared to isometric quadriceps exercises isolating the p-value which is p<0.0001 for both the exercises. The lowest value for pain is 0 and the highest value for 8th week shows a marked decrease in level of pain for short arc exercises than isometric quadriceps exercises which is for short arc level of pain recorded was (4) and for isometric exercises the highest level of pain for week 8 was (8) which shows the effectiveness of short arc quadriceps exercises as compared to isometric quadriceps exercises.
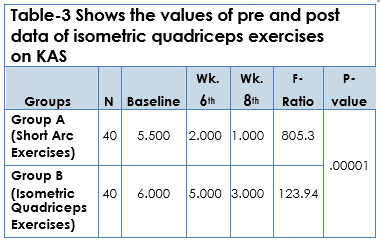
Friedman Test
Whereas, the values of median from baseline to 8th week are markedly decreased for short arc exercises as compared to isometric quadriceps exercises, also Friedman test showed that the value of the F-Ratio is increased for short arc quadriceps exercises with p value (P < 0.0001) hence, the efficacy of short arc quadriceps exercises for pain relief is greater than isometric quadriceps exercises. Kujala assessment score was used to identify the activity of patients suffering with Anterior knee pain. The form consists of 13 questions and each question consists of a minimum value of (0) and maximum value of (10). The total score of this form is 100. By compiling the score of all 13 questions, forty individuals n=40 were enrolled for the assessment of pre and post exercise plan for both groups i.e. (Isometric and Short arc quadriceps exercise group). The assessment includes the first day i.e. week 1st and post assessment was done at the last week (i.e.) 8th week.
The distribution chart shows that the highest value of pre data is 83, 84 whereas the highest value of post data is 85 for isometric quadriceps exercises. For short arc exercises the highest value of pre data is 84 whereas the highest value for post data is 95. Table-4.
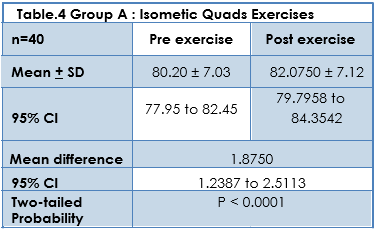
The results of Group A after applying paired t-test i.e. Isometric Quadriceps exercises shows the improvement of mean and SD of post exercise i.e. 82.0750 + 7.1266 with two tailed probability of P<0.0001.Table-4.
COMPARISION OF PRE AND POST SHORT ARC QUADRICEP EXERCISES
The results of Group B after applying paired t-test i.e. short arc Quadriceps exercises shows the improvement of mean and SD of post exercise i.e. 88.20+ 6.64 with two tailed probability of P<0.0001.
POST EXERCISE COMPARISION OF ISOMETRIC AND SHORT ARC QUADRICEP EXERCISES
After comparing the results of both groups the Mean±S.D is higher (88.20+ 6.64) for Group B (Short arc quadricep exercises than Group A (Isometric exercises) (82.07±7.12) with constant mean difference for both exercises i.e. 6.12, 95 % C.I=3.05 to 9.19 with probability<0.05.
The results of the study revealed that short arc quadriceps exercises have a beneficial effect in patients with Anterior Knee Pain N=(40). The results of this study demonstrated that Short arc quadriceps exercises brought significant improvements on all parameters than isometric quadriceps exercise after the 8-week training programme.
The results of our study showed that short arc quadriceps exercises have significant impact on pain, muscle activity and HRQoL in comparison with isometric exercises in reducing anterior knee pain. A study conducted by Earl et al showed greater reduction in level of pain. The pain was reduced significantly (Pre mean: 40.6±18 to post mean: 5±7. In this research we focused on HRQoL, muscle activity and reducing level of pain. Focus on the study, comparison of short arc and isometric quadriceps exercises shows that the Short arc quadriceps exercises brought significant improvements on all parameters than isometric quadriceps exercise after the 8-weeks training programme. In the current study VAS Scale (numerical) is used to measure pain, whereas in the research of Earl et al, pain was also measured via Numerical Rating Scale, knee abductor muscle should be focused to strengthen instead of knee extensor muscle14. Study on quasi-randomised trials evaluating the effect of exercise therapy on pain, function and recovery in adolescents and adults with patellofemoral pain syndrome. Researcher used vas numerical rating scale (0-10 ) to evaluate the level of pain and suggested that the pain decreased not only in short term of exercise therapy, but after long term of functional exercise therapy which includes strength exercises such as isokinetic, open and closed kinetic exercises on the knee joint with mean and S.D (0.99±1.84). Similar to our study NRS numerical rating scale is used to measure the level of decreasing pain with time and the most decrease in pain was found at eight weeks of short arc quadricep exercises with 95% C.I (0-2) and P-value <0.00515.
Only statistical significant improvements brought about by the strengthening exercises was in the mental aspect of the SF-12 questionnaire. The main difference between the study by Foley et al and the present study was the shorter duration of the intervention, which consisted of eight weeks and shorter duration of session. Whereas, in the current study, KUJALA assessment questionnaire was used instead of the SF-12 Questionnaire. However, both studies performed rehabilitation protocols. EMG Biofeedback used as an assessment protocol for the study. Biofeedback mechanism system identifies the efficiency of the muscle16. The efficacy of EMG biofeedback on vastusmedialis and vastus lateralis muscle, similarly in this study the referenced muscle was vastusmedialis. Briani in his study performed exercises in a sitting position, whereas in the current study, exercises have been performed in a supine lying position17.
In the current study, short arc quadriceps exercises are more efficient to produce strength and enhance health related quality of life (HRQoL) with pain relief. A study was conducted to identify the effect of short arc quadriceps exercises with or without EMG Biofeedback mechanism and proved that exercise with EMG biofeedback increased the efficiency of muscle than exercises without usage of EMG Biofeedback18,19.
The quadriceps exercises on knee joint also has an effect on the adjacent joints like hip and knee by producing the particular group of exercises. It not only produces strength in the knee joint, but also enhances the efficiency of the hip joint and reduc-es the level of pain20-23. Vastus medialis and vastus lateralis, both muscles are involved in the alignment of the knee cap (patella) and isometric contrac-tions of the quadriceps muscle group can produce a great impact of the strength on knee dynamic stability24,25.
After comparing the results, it has been concluded that the values of short arc exercises shows greater muscle activity on EMG Biofeedback and reduction of pain (Visual Analog Scale) as compared to isometric quadricep exercises. The values of KUJALA assessment form after applying paired and independent t-test shows that the effectiveness of short arc quadriceps exercises are more effective to improve Activities of daily livings (ADLs). Hence, short arc quadriceps exercises are more effective to reduce pain, increase muscular activity and improve health related quality of life.
- Anwer S, Alghadir A. Effect of isometric quadri-ceps exercise on muscle strength, pain, and function in patients with knee osteoarthritis: a randomized controlled study. J. Phys. Ther. Sci. 2014;26(5):745-8.
- Bird ML, Callisaya ML, Cannell J, Gibbons T, Smith ST, Ahuja KD. Accuracy, validity, and reliability of an electronic visual analog scale for pain on a touch screen tablet in healthy older adults: a clinical trial. Interact. J. Med. Res.. 2016;5(1):e3.
- Khasawneh RR, Allouh MZ, Abu-El-Rub E. Mea-surement of the quadriceps (Q) angle with respect to various body parameters in young Arab population. PloS one. 2019;14(6).
- Vora M, Curry E, Chipman A, Matzkin E, Li X. Patellofemoral pain syndrome in female athletes: A review of diagnoses, etiology and treatment options. Orthopedic reviews. 2017 ;9(4)..
- Hernández-Socorro CR, Saavedra P, López-Fernández JC, Ruiz-Santana S. Assess-ment of muscle wasting in long-stay ICU patients using a new ultrasound protocol. Nutrients. 2018 ;10(12):1849.
- Argent R, Slevin P, Bevilacqua A, Neligan M, Daly A, Caulfield B. Clinician perceptions of a prototype wearable exercise biofeedback system for orthopaedic rehabilitation: A quali-tative exploration. BMJ open. 2018 ;8(10):e026326.
- Holsen M. Operative Treatment and Magnetic Resonance Imaging-Based Diagnostics of Knee Disorders in Military Conscripts. 2017.
- Henderson RE, Walker BF, Young KJ. The accu-racy of diagnostic ultrasound imaging for musculoskeletal soft tissue pathology of the extremities: a comprehensive review of the literature. Chiropr. Man. Ther. 2015;23(1):31.
- Ittenbach RF, Huang G, Foss KD, Hewett TE, Myer GD. Reliability and validity of the anterior knee pain scale: applications for use as an epidemiologic screener. PLOS one. 2016;11(7).
- Kim TW, Gay N, Khemka A, Garino J. Internet-based exercise therapy using algo-rithms for conservative treatment of anterior knee pain: a pragmatic randomized controlled trial. JMIR rehabilitation and assistive technologies. 2016;3(2):e12.
- Korkmaz O, Malkoc M. Effect of anterior cruci-ate ligament reconstruction with hamstring tendons on Insall-Salvati index and anterior knee pain. Srpskiarhivzacelokupnolekarst-vo.2018;146(3-4):174-8.
- Manoharan A, Selvaraj A, Ramachandranath VA. Prevalence of anterior knee pain in 20-40 years old adults attending ortho OPD in a tertiary care hospital in Tamil Nadu. Int J Orthop Sci. 2016;2:244-7.
- Mason JS, Crowell M, Dolbeer J, Morris J, Terry A, Koppenhaver S, Goss DL. The effectiveness of dry needling and stretching vs. stretching alone on hamstring flexibility in patients with knee pain: a randomized controlled trial. Int. J. Sports Phys. 2016 Oct;11(5):672.
- Nuttall C, Winters BA. Understanding Anterior Knee Pain: Patellofemoral Pain Syndrome. J Nurse Pract. 2015 Nov 1;11(10):1032-5.
- Worsley PR, Kitsell F, Samuel D, Stokes M. Validi-ty of measuring distal vastus medialis muscle using rehabilitative ultrasound imaging versus magnetic resonance imaging. Man. Ther. 2014 Jun 1;19(3):259-63.
- Reich A, Chatzigeorkidis E, Zeidler C, Osada N, Furue M, Takamori K, Ebata T, Augustin M, Szepietowski JC, Ständer S. Tailoring the cut-off values of the visual analogue scale and numeric rating scale in itch assessment. Acta Dermato-Venereologica. 2017 Jul 1;97(6-7): 759-60.
- Pazzinatto MF, Silva DD, Briani RV, Ferrari D, Aragão FA, Albuquerque CE, Azevedo FM. Reliability of electromyography parameters during stair deambulation in patellofemoral pain syndrome. Motriz: Revista de Educação Física. 2015 ;21(2):207-13.
- Rathleff MS, Rathleff CR, Olesen JL, Rasmussen S, Roos EM. Is knee pain during adolescence a self-limiting condition? Prognosis of patellofemoral pain and other types of knee pain. Am J Sport Med.. 2016 May;44(5): 1165-71.
- Raeissadat SA, Rayegani SM, Sedighipour L, Bossaghzade Z, Abdollahzadeh MH, Nikray R, Mollayi F. The efficacy of electromyographic biofeedback on pain, function, and maximal thickness of vastus medialis oblique muscle in patients with knee osteoarthritis: a randomized clinical trial. J Pain Res. 2018;11:2781.
- Smith BE, Selfe J, Thacker D, Hendrick P, Bateman M, Moffatt F, Rathleff MS, Smith TO, Logan P. Incidence and prevalence of patellofemoral pain: A systematic review and meta-analysis. PloS one. 2018;13(1):e0190892.
- Huang L, Guo B, Xu F, Zhao J. Effects of quadri-ceps functional exercise with isometric contraction in the treatment of knee osteoar-thritis. International journal of rheumatic diseas-es. 2018 ;21(5):952-9.
- Furu M, Ito H, Nishikawa T, Nankaku M, Kuriya-ma S, Ishikawa M, Nakamura S, Azukizawa M, Hamamoto Y, Matsuda S. Quadriceps strength affects patient satisfaction after total knee arthroplasty. J Orthop Sci. 2016 ;21(1):38-43.
- Jeon K, Chun S, Seo B. Effects of muscle strength asymmetry between left and right on isokinetic strength of the knee and ankle joints depending on athletic performance level. Int. J. Sports Phys. 2016;28(4):1289-93.
- Freddolini M, Placella G, Gervasi GL, Morello S, Cerulli G. Quadriceps muscles activity during gait: comparison between PFPS subjects and healthy control. Musculoskeletal surgery. 2017 ;101(2):181-7.
- de Freitas FS, Brown LE, Gomes WA, Behm DG, Marchetti PH. No Effect of Kinesiology Tape on Passive Tension, Strength or Quadriceps Muscle Activation of During Maximal Voluntary Isometric Contractions in Resistance Trained Men. Int. J. Sports Phys. 2018 ;13(4):661.