
ABSTRACT
BACKGROUND
Back pain is one of the most frequently seen health problems, affecting 9 out of 10 people in a population at some point during their lives1. The lower back is the region most commonly affected. Low-back pain can be debilitating, and it is often challenging to treat Low Back Pain.
OBJECTIVE
The objective of this review is to evaluate the efficacy of High-Velocity Low-Amplitude (HVLA) Spinal Manipulative Therapy (SMT) for Non-Specific Low Back Pain (NSLBP).
STUDY DESIGN
Systemic review
METHODS
Only articles that had adult (18 years and above) participants were included in this review and studies that classified the intervention as HVLA spinal manipulation were included. Studies that included spinal manipulation other than HVLA or studies of spinal manipulation under anesthesia were excluded.
RESULTS
Eight full text papers and three systemic reviews justifying the inclusion criteria are reviewed which revealed that high velocity low amplitude spinal manipulative therapy have significant effect in alleviating low back pain.
CONCLUSION
Spinal manipulation therapy is a distinctive approach that considerably decreases nonspecific low back pain however there is need of further clinical trials into this subject focusing solely on high velocity low amplitude spinal manipulation.
KEY WORDS
High Velocity Low Amplitude (HVLA), Spinal Manipulation Therapy (SMT), Non-Specific Low Back Pain (NSLBP), Osteopathic Spinal Manipulation(OST), Acute Low Back Pain (ALBP), Chronic Low Back Pain (CLBP).
Sadaf Shafqat
Lecturer
Ziauddin College of Physical Therapy
Ziauddin University
[Shafqat S. Efficacy of High-Velocit Low-Amplitude Spinal Manipulation for Non Specific Low Back Pain – A Systemic Review Pak. j. rehabil. 2014;3(1):4-14]
INTRODUCTION
Low back pain (LBP) is one of the most common health disorders and cause of disability1,2. It is estimated that worldwide, nine out of ten adults experience low back pain (LBP) once in lifetime1. It results in a major individual and fiscal burden globally. While it affects both the genders of all ages it is estimated that it is more common amongst adults of working age and hence it is also a major cause of functional disability and work absenteeism1. However, in elderly as well low back pain (LBP) is one of the most frequently reported symptom3-7. It is defined as the pain and muscle stiffness localized below the costal margin and above the inferior gluteal region, with or without sciatica8.
There are multiple etiologies of low back pain (LBP); excessive repeated activity, disk injury or degeneration, spondylolisthesis, spinal stenosis, scoliosis etc. Consequently, the characteristic of pain also varies; it may be sharp or stabbing, dull or achy. Activities such as jogging or running on cement roads instead of cinder tracks, heavy lifting, and prolonged sitting (especially in cars, trucks, and poorly designed chairs) can provoke back pain9,10.
The onset of low back pain (LBP) varies it may be acute or chronic. Acute low back pain (ALBP) is of a time period less than 3 months however, it is classified as chronic low back pain (CLBP) if it persists beyond the normal phase of healing i.e. more than twelve weeks. Low back pain (LBP) is thus more disabling if it is chronic and causes more physical and psychological impediment10. The term nonspecific means that the pain is not characteristic to an identifiable pathology (e.g., tumor, infection, inflammation, fracture, osteoporosis, rheumatoid arthritis)8. Almost 85% of people suffer from non-specific low back pain (NSLBP)11.
Despite this lack of knowledge, regarding underlying pathology, a number of interventions exist for the treatment of non-specific low back pain (NSLBP) and spinal manipulation therapy (SMT) is one of them.
Spinal manipulation (SM) is practiced by health care professionals and some medical doctors as well12.In clinical setting, the selection of a manipulation technique varies widely among therapists. Spinal manipulation therapy (SMT) may be given with thrust; high velocity low amplitude (HVLA) or without thrust; low velocity high amplitude (LVHA). High velocity low amplitude (HVLA) is performed through pain and is usually associated with an audible sound, a cavitation pop whereas there is no audible sound in low velocity high amplitude (LVHA) which is applied in relatively acute conditions of less than three months13.
High velocity low amplitude spinal manipulation (HVLA-SM) is performed with the participant in the lateral recumbent position. Patients achieve a side-lying position with the free hip and knee slightly flexed and adducted while the lumbar spine and pelvis remain roughly perpendicular to the treatment are. On the weight bearing side, the hip and knee, are extended or very slightly flexed. The therapist stands in front of the patient while stabilizing the free thigh and leg with their own thigh. The patient’s shoulder is stabilized with the therapist’s hand stabilizing hand while the patient’s forearms rest across his chest or abdomen. A precise high velocity low amplitude manipulative thrust (HVLA-MT) is applied with the therapist’s other hand on specific areas of the patient’s lumbar vertebrae (mamillary process, spinous process) or pelvis (posterior superior iliac spine, ischial tuberosity, sacral ala, 1st sacral segment, 3-4th sacral segment), depending on the condition and treatment objectives. Brief controlled movements of the therapist’s upper limb and body, often combined with a slight falling or body-drop movement creates the momentum and position for high velocity low amplitude spinal manipulation thrust (HVLA-SMT) that is provided through the contact hand. The direction of thrust varies with therapeutic intent and point of contact. Thrust is not provided with the stabilizing hand; nonetheless, to maintain patient’s stability on the treatment couch, slight counter pressure is often essential 14,15,16.
A large number of evidence on non-biomechanical effects of spinal manipulative therapy (SMT) in people who are healthy and in people with symptoms of low back pain (LBP) has been published in the past decade, having said that the effectiveness of spinal manipulative therapy (SMT) in decreasing low back pain (LBP) is still uncertain17,18,19,20,21. Previous systematic reviews also proposed that high velocity low amplitude (HVLA) spinal manipulative therapy (SMT) will improve clinical outcomes, however its efficaciousness compared to different common intervention has not been clearly demonstrated. Thus, the objective of this review is to assess the efficacy of High velocity low amplitude (HVLA) spinal manipulative therapy (SMT) for nonspecific low back pain (NSLBP) as it is still notoriously indefinite.
METHODS
Study Design
This systemic review used the Preferred Reporting Items for Systemic Reviews and Meta Analyses (PRISMA) guidelines22 which is a 27-item checklist intended to improve eminence of systemic reviews and meta-analyses of randomized controlled trials, in particular, but can be used for other study designs as well23.
Eligibility Criteria
The eligibility criterion comprises of population, intervention, control, outcomes, and study design (PICOS) principles as follows:
Population: Adults, 18 years and above, participants presenting with sign and symptoms of Non-Specific Low Back Pain (NSLBP). Intervention: High velocity low amplitude (HVLA) spinal manipulation therapy (SMT) intervention was eligible for inclusion in this review.
Control: Any group that did not receive HVLA spinal manipulation or a group determining efficacy of technique other than HVLA.
Outcomes: The outcomes could include but were not limited to patient reported pain reduction and improved quality of life (QoL). For inclusion the outcome measures must have been obtained at least once post treatment.
Study Design: Only randomized controlled trials (RCTs) and systemic reviews are eligible to be included in this review.
Search Procedure
Using MeSH terms such as Low Back Pain (LBP), Non-Specific Low Back Pain (NSLBP), Spinal Manipulation Therapy (SMT), Osteopathic Spinal Manipulation (OST), High Velocity Low Amplitude (HVLA), High Velocity Low Amplitude Spinal Manipulation (HVLASM), and Chronic Back Pain (CBP) systemic searches were conducted in the following electronic databases (from their origin up to February 2014): MEDLINE, EMBASE, AMED, CINAHL, PEDro, APTA, MANTIS, OSTMED, ScienceDirect and Cochrane database. Initially the MeSH terms were searched individually and then later using Boolean logic OR and AND the search was carried out. Moreover, reference lists of all articles were also searched for further literature.
Study Selection
The searched articles were reviewed to identify the studies as randomized control trials (RCTs) fulfilling the inclusion criteria. Full texts of the articles, that met the inclusion criteria, were extracted to further assess whether they fulfilled the eligibility criteria. Studies that involved manipulation under anesthesia (MUA) or studies involving hospitalized patients as participants were excluded from this review. Non-English language articles, animal and cadaver studies were not included. Case reports, case series, editorials, comments, letters, abstracts, guidelines and protocols were also excluded, from this review, due to risk of bias associated with these designs.
Data Collection
Eight eligible trials were reviewed and data was collected. The items that were extracted from studies were: study design, description of sample size, number of treatments provided, description of comparison interventions, assessment measures and results as shown in Table 1.
Risk of Bias
Risk of bias was assessed using the Cochrane Collaboration’s Tool for Assessing Risk of Bias24 that comprises of following domains:
a) Was the allocation sequence adequately generated?
b) Was the allocation adequately concealed?
c) Was information of the allocated interventions adequately prevented during the study?
d) Were incomplete outcome data sufficiently addressed?
e) Are reports of the study free of suggestion of selective outcome reporting?
f) Was the study apparently free of other problems that could put it at a risk of bias?
The completed risk of bias tool is displayed in Table 1. Possible approach for summary assessments outcome (across domains) within and across studies was given by Yes (Y) i.e. Low Risk of Bias, No (N) i.e. High Risk of Bias, Unclear (U) i.e. Unclear Risk of Bias.
Additionally, the Physiotherapy Evidence Database PEDro- Scores25 for papers in this review was summarized as well that contains the following list of criteria:
a) Eligibility criteria were specified.
b) Participants were randomly allocated to groups.
c) Allocation was concealed.
d) The groups were comparable at baseline regarding the most important prognostic indicators.
e) There was blinding of all subjects.
f) Blinding of all therapists who administered the therapy was performed.
g) Blinding of all assessors who measured at least one key outcome was performed.
h) Measures of at least one key outcome were attained from more than 85%of the subjects initially allocated to groups.
i) Subjects for whom outcome measures were available received the treatment or control condition as allocated or, where this was not the case; data for at least one key outcome was analyzed by intention to treat. j) The results of between-group statistical comparisons are reported for at least one key outcome.
k) Both point measures and measures of variability are provided for at least one key outcome.
These evaluators were employed as they have been shown to be reliable and valid for the assessment of randomized controlled trials.
Synthesis of Results
The results of the search strategy are presented in a PRISMA (Preferred Reporting Items for Systemic Reviews and Meta Analyses) flow chart22 (Fig. 1) which demonstrates, a total of 434 citations were identified through the search strategy out of which 309 articles were not relevant to the subject matter and thus were not considered.125 records were screened and after the removal of duplicate records only eight papers satisfied the eligibility criteria of this review; Hoehler et al.26, Cherkin et al.27, Andersson et al.28,Descarreaux et al.29, Bronfort et al.30,Balthazard P et al.31,de OliveriaRF et al.32, Haas et al. 33 Out of these the trial by Haas et al. is a forthcoming article in press. Three systemic reviews, by Licciardoneetal.34, Ferreira et al.35, Kuczynski et al.36, were also procured that fulfilled the inclusion criteria.
Fig.1 PRISMA Flow Chart
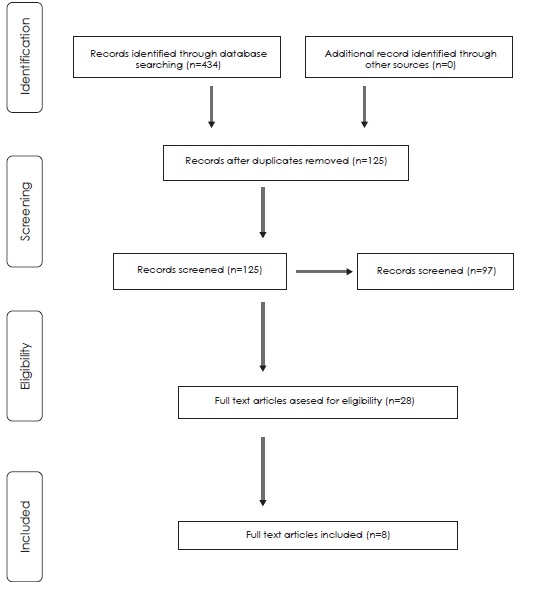
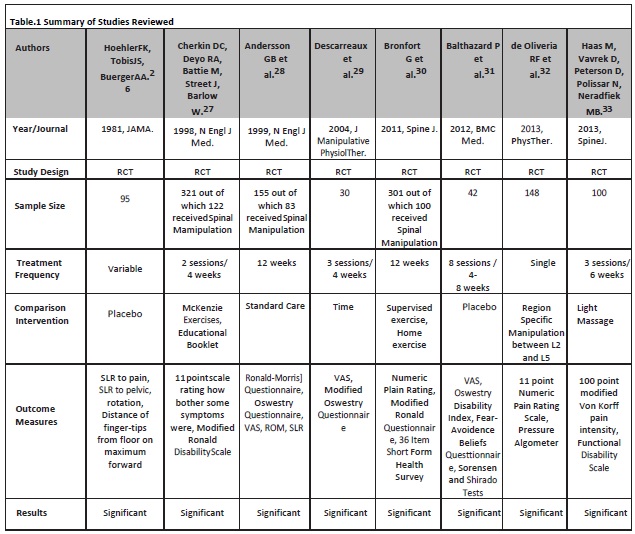
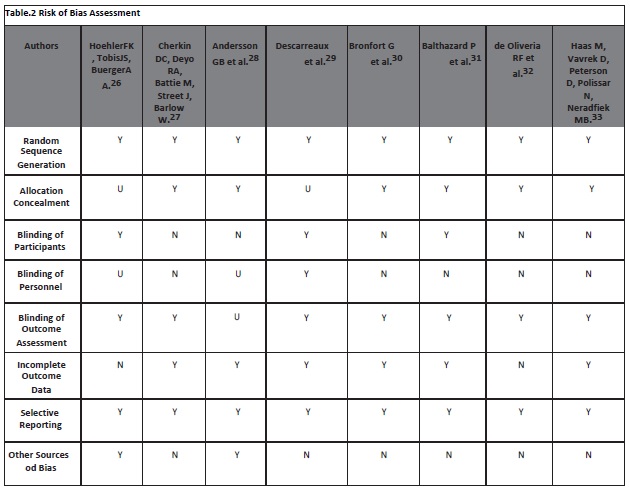
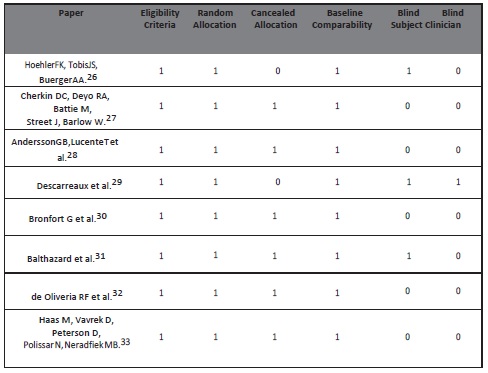
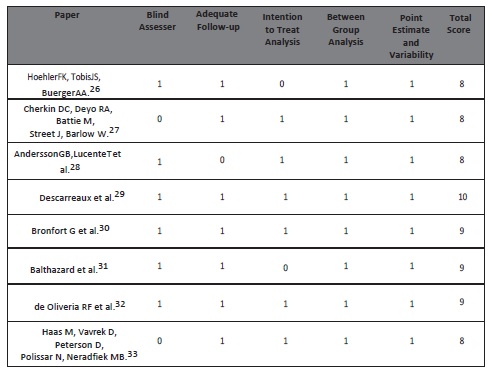
Table. 3 The Physiotherapy Evidence Database (PEDro) Score for papers in this review
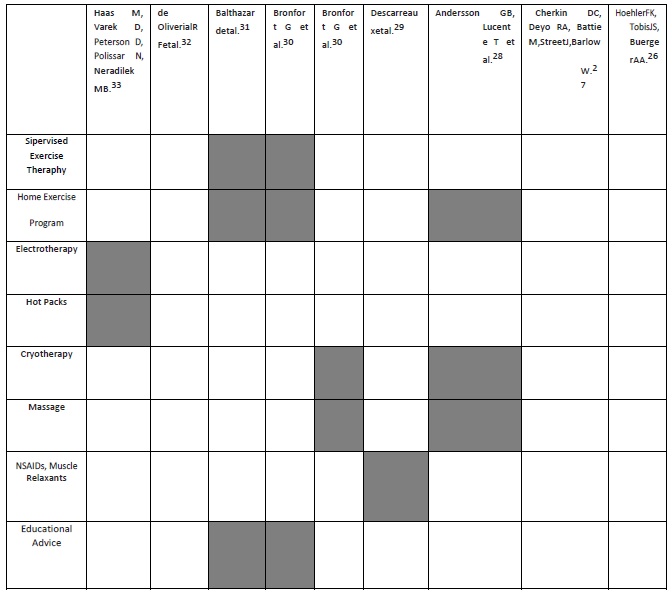
Table. 4 Adjuvant Conservative Treatment Strategies Used
DISCUSSION
This systemic review intended to determine the efficacy of high velocity low amplitude spinal manipulative therapy (HVLA-SMT) in nonspecific low back pain (NSLBP), by an updated literature review, identified that low back pain (LBP) conditions are reduced after spinal manipulative therapy (SMT). The Physiotherapy Evidence Database (PEDro) scores of the studies included in this review shows that the methodological quality of this topic and of the trials included was generally high and the study by Descarreaux et al.29,with three fold blinding, scored 10 out of 11 on Physiotherapy Evidence Database (PEDro)scale. However, amongst all other randomized controlled trials, this was the only study that had the lowest sample size of 30. Moreover, this was also the only study that examined the sole effect of time on pain and disability levels and the study was divided into two phases.
A large number of potential studies were excluded and studies using clearly defined high velocity low amplitude spinal manipulative therapy (HVLA-SMT) as treatment were included. There was no gender restriction in any of the trials included. The maximum sample size measured, in any of the eight randomized controlled trials (RCTs), was 321 in the study by Cherkin DC et al. out of which 122 patients received spinal manipulative therapy (SMT)27. Cherkin DC et al. had two comparison groups out of which one was a minimal intervention control group that received an educational booklet that discussed causes of low back pain (LBP), prognosis, appropriate use of imaging studies and activities for promoting recovery and preventing recurrences. Since the booklet group did not receive care during follow up, the group showed low levels of satisfactions with care whereas main benefit of spinal manipulative therapy (SMT) in contrast, according to the authors, was increased levels of satisfaction with care27.
Outcome assessors of the studies included; 100 point modified Von Korff Pain Intensity, 11 Point Numeric Pain Rating Scale, 36 Item Short Form Health Survey,11 Point Scale of Bothersomenessrating how bothersome symptoms were, Functional Disability Scale, Modified Roland Disability Scale, Oswestry Disability Index, Pressure Algometer, Fear Avoidance Beliefs Questionnaire, Range of Motion (ROM), Straight Leg Raising (SLR) to Pain, Straight Leg Raising (SLR) to Pelvic Rotation, Distance of Finger-tips from floor on maximum forward flexion, Sorensen and Shirado Tests.
The study by Haas M et al.assessed dose response of spinal manipulation (SM) and revealed that 12 sessions of spinal manipulative therapy (SMT) in 6 weeks, from a therapist, yielded the most favorable pain and functional disability improvement for chronic nonspecific low back pain (CNSLBP)33. Whereas according to the study of Bronfort et al. patients who received supervised clinical exercise, for the management of chronic nonspecific low back pain (CNSLBP), reported to be more satisfied with care given during the treatment and in follow up periods when compared with the patients who received spinal manipulative therapy (SMT) however the short and long term differences were small and not statistically significant. The distinctive feature of this trial was that it included patient’s preferences at different levels using quantitative and qualitative methods and assessed the preferences through comprehensive interviews and according to this study the outcome that was most important to the patients was pain. This study also assessed trunk muscle strength and endurance by blind examiners30.
A systemic review that included studies pertaining to only pain outcomes also stated spinal manipulative therapy (SMT) effective in reducing pain34. They also concluded that the level of pain reduction is greater than expected from placebo effects alone and persists for at least three months.
The study by Balthazard P et al. confirms the immediate analgesic effects of spinal manipulative therapy (SMT) and compared it to a true placebo intervention in which they provided ultrasound treatment and the patient did not know the device is not turned on and that the treatment was ineffective31.
Only one trial reported no significant difference in clinical outcomes between standard care and spinal manipulative therapy (SMT) amongst patients with low back pain (LBP)of at least three weeks in duration28.The main areas of weakness in this study were the size of the study groups; 72 in the smaller group, as compared with an ideal size of more than 100, the lack of a placebo control group, and the lack of blinding of the patients. The study by Ferreira et al. also concluded spinal manipulative therapy (SMT) not to be much effective when compared to non-steroidal anti-inflammatory drugs (NSAIDs) in improving disability of patients with chronic low back pain (CLBP)35.
The effect of spinal manipulative therapy (SMT) on pressure pain threshold (PPT) was assessed by de Olivera RF et al.32 in the study comparing region specific and non region specific manipulation at lumbar level. No changes were observed on pressure pain threshold in region specific manipulation whereas increase in pressure pain threshold (PPT) was reported, at lumbar level, in the non region specific group receiving manipulation.
The review by Kuczynski JJ et al. stated spinal manipulative therapy (SMT)to be a safe intervention that improves clinical outcomes for a variety of patients with low back pain (LBP)36.The overall results of all trails, included in this review, ascertained the efficacy of spinal manipulative therapy (SMT) though the extent of efficaciousness is variable amongst the studies.
STRENGTHS AND LIMITATIONS
The studies included in this review used ample outcome measures furthermore the quality of trials included was also respectable and the risk of bias assessment was, on average, low as well however there were some limitations in this review.
Alike in any systemic review there is a possibility that there may be clinical trials that were missed in the search process furthermore the search strategy was limited to include only those articles which were published in English language. Moreover, there were only two trials in this review that focused only on high velocity low amplitude spinal manipulation (HVLA-SMT) without any adjuvant conservative treatment (Table. 4)and this is mentioned in only one out of them. One more consistent feature across all studies, except one, is a failure to blind the care giver and a majority of the studies did not integrate blinding of participants which does not eliminate the risk of bias and thus appends to the limitations of this review.
IMPLICATIONS FOR PRACTICE
Despite the aforementioned limitation there appears to be a trend suggesting high velocity low amplitude spinal manipulation (HVLA-SMT) has a useful role to play in the management of non- specific low back pain (NSLBP) neither any of the reviews conclusively demonstrates that spinal manipulative therapy (SMT) is ineffective. Furthermore, spinal manipulation (SM) has been associated with frequent but minimal adverse effects and with serious but possibly rare complications so the risk benefit ratio should be considered prior to beginning spinal manipulative therapy (SMT)37,38. However its efficacy in chronic conditions compared to acute conditions is still uncertain.
IMPLICATIONS FOR RESEARCH
Due to paucity of research and aforementioned limitations associated with present researches the ambiguity regarding the efficacy of high velocity low amplitude spinal manipulation therapy (HVLA–SMT) still exists. There is a need of quality evidence with random, adequate, concealed allocation and with three fold blinding, adequate follow up and between group analyses to reach to a definite conclusion. The studies should consider the role of spinal manipulation (SM) in acute, sub-acute and chronic long standing conditions individually with variation in manipulation techniques in accordance to the condition. Clinical trials analyzing the mechanism of action of the techniques of spinal manipulation (SM) are also needed intensely.
CONCLUSION
This review indicates the scarcity of clinical trials assessing the efficacy of high velocity low amplitude spinal manipulation therapy (HVLA-SMT) in nonspecific low back pain (NSLBP) however its significance in treating it cannot be repudiated but further research is warranted to fully evaluate the likely benefit.
ACKNOWLEDGEMENT
I am grateful to Allah – The Supreme, for granting me with the blessing of education and enlightening me with the power of knowledge. I express my heartfelt gratitude to the academic staff of Ziauddin College of Physical Therapy and the team of Pakistan Journal of Rehabilitation for their assistance. Finally, I profoundly thank my parents, family and friends for their unconditional support and encouragement. Ethical approval: Not applicable.
Conflict of interest: None declared.
REFERENCES
- Shafqat S. Efficacy of High-Velocity Low-Amplitude Spinal Manipulation for Non Specific LBP Rafique MK, Taqi A. The causes, prevention and management of post spinal backache: an overview. Anaesth Pain and Intensive Care. 2011;15(1):65-9.
- Balague F, Mannion A, Pellise F. Cedraschi C. Clinical update: low back pain. Lancet. 2007;369:725-28.
- Andersson GB. Epidemiology of low back pain. ActaOrthopScand Suppl. 1998;281:28–31.
- Dionne CE, Dunn KM, Croft PR. Does back pain prevalence really decrease with increasing age. A systematic review. Age Ageing. 2006;35:229–34.
- Rapoport J, Jacobs P, Bell NR, Klarenbach S. Refining themeasurement of the economic burden of chronic diseases inCanada. Chronic Dis Can. 2004;25:13–21.
- Deyo RA, Cherkin D, Conrad D, Volinn E. Cost, controversy, crisis: low back pain and the health of the public. Annu Rev PublicHealth. 1991;12:141–56.
- Cassidy JD, Côté P, Carroll LJ, Kristman V. Incidence and course of low back pain episodes in the general population. Spine. 2005; 30: 2817–23.
- Newswanger DL. Osteopathic medicine in the treatment of low back pain. Am Fam Physician. 2000;62(11):2414-15.
- Low back pain [online] 2013 Dec [cited 2014 Feb 1]. Available from: URL: http://orthoinfo.aaos.org/topic.cfm?topic=a00311
- Ehrlich GE. Bulletin of the World Health Organization. 2003;81:671-676.
- Airaksinen O. European guidelinesfor the management of chronic nonspecific low back pain. Eur Spine J. 2006;15(2):192-300.
- National Center for Complementary and Alternative Medicine. Spinal manipulation for low-back pain. [online] 2013 Apr [cited 2014 Feb 4]. Available from:URL: http://nccam.nih.gov/health/pain/spinemanipulation. htm
- Pizzorno J Jr. Naturopathic Physical Medicine: Theory and Practice for Manual Therapists and Naturopaths. Europe: Elsevier Limited; 2008.
- Evans DW, Lucas N. What is manipulation. A reappraisal. Man Ther. 2010;15(3):286-291.
- Hondras MA, Long CR, Cao Y, Rowell RM, Meeker WC. A randomized controlled trial comparing 2 types of spinal manipulation and minimal conservative medical care for adults 55 years and older with subacute or chronic low back pain. J Manipulative 2009;32(5):330-343.
- Van ZoestGG, Gosselin G. Three-dimensionality of direct contact forces in chiropractic spinal manipulative therapy. J Manipulative PhysiolTher. 2003;26(9):549-556.
- Bialosky JE, Simon CB, Bishop MD et al. Basis for spinal manipulative therapy: a physical therapist perspective. J ElectromyogrKinesiol. 2012;22:643-47.
- Pickar JG. Neurophysiological effects of spinal manipulation. Spine J. 2002;2:357-71.
- Bishop MD, BeneciukJM, George SZ. Immediate reduction in temporal sensory summation after thoracic spinal manipulation. Spine J. 2011;11:440-46.
- GeorgeSZ, Bishop MD, Bialosky JE et al. Immediate effects of spinal manipulation on thermal pain sensitivity: an experimental study. BMC MusculoskeletDisord. 2006;67:68.
- Bialosky JE, Bishop MD, Robinson JE et al. Spinal manipulative therapy has an immediate effect on thermal pain sensitivity in people with low back pain: a randomized controlled trial. Phys Ther. 2009;89:129-303.
- Moher D, Liberati A, Altman DG, the PRISMA Group. Preferred reporting items for systemic reviews and meta-analyses: the PRISMA statement. BMJ 2009;339:332-6.
- Swartz MK. The PRISMA statement: a guideline for systemic reviews and meta-analyses. J Pediatr Health Care 2011;25(1):1-2.
- Higgins J, Green S. Cochrane Handbook for Systematic Reviews of Interventions. The Cochrane Collaboration; 2011.
- PEDro Physiotherapy Evidence Database. PEDro Scale. [online] 1999 Jun [cited 2014 Feb 2]. Available from: URL: http://www.pedro.org.au/english/downloads/ pedro-scale/
- Hoehler FK, Tobis JS, Buerger AA. Spinal manipulation for low back pain. JAMA. 1981;245:1835-38.
- Cherkin DC, Deyo RA, Battié M, Street J, Barlow W. A comparison of physical therapy, chiropractic manipulation, and provision of an educational booklet for the treatment of patients with low back pain. N Engl J Med. 1998;339(15):1021-29.
- Andersson GB et al. A comparison of osteopathic spinal manipulation with standard care for patients with low back pain. N Engl J Med. 1999;341:1426-31.
- Efficacy of preventive spinal manipulation for chronic low-back pain and related disabilities. J Manipulative PhysiolTher. 2004;27(8):509-514.
- Bronfort et al. Supervised exercise, spinal Manipulation, and home exercise for chronic low back pain: A randomized clinical trial. Spine J. 2011;585-98.
- Balthazard P et al. Manual therapy followed by specific active exercises versus a placebo followed by specific active exercises on the improvement of functional disability in patients with chronic nonspecific low back pain: a randomized control trial. BMC Med. 2012;13:162-72.
- deOliveria RF et al. Immediate effects of region-specific and non-region specific spinal manipulative therapy in patients with chronic low back pain: A randomized controlled trial. PhysTher. 2013;93:748-56.
- Haas M, Vavrek D, Peterson D, Polissar N, Neradilek MB. Dose-response and efficacy of spinal manipulation for care of chronic low back pain: A randomized controlled trial. Spine J. Forthcoming 2013 July 22.
- Licciardone JG, Brimhall AK, King LN. Osteopathic manipulative treatment for low back pain: A systemic review and meta-analysis of randomized controlled BMC Med. 2005;6:43.
- Ferreira ML, Ferreira PH, Latimer J, Herbert R, Maher CG. Does spinal manipulative therapy help people with chronic low back pain.Aust J Physio. 2002;48:277-84.
- Kuczynski JJ, Schwieterman B, Columber K, Knupp D, Shaub L, Cook CE. Effectiveness of physical therapist administered spinal manipulation for the treatment of low back pain: a systematic review of the literature. Int J Sports Phys Ther. 2012;7(6):647-62.
- Cagnie B, Vinck E, Beernaert A, Cambier D. How common are side effects of spinal manipulation and can these side effects be predicted. Man Ther. 2004;9:151-6.
- Stevinson C, Ernst E. risks associated with spinal manipulation. Am J Med. 2002;112:566-7.