
ABSTRACT
OBJECTIVE
To find out the frequency of work, related to Low Back Pain (LBP) among physical therapist of tertiary care hospital of Karachi. To analyze the effects of physical activity level, sub-specialty areas and Body Mass Index (BMI) on Work Related Low Back Pain (WRLBP) as well.
STUDY DESIGN AND SAMPLING TECHNIQUE
A cross-sectional survey was conducted with non-probability convenience sampling technique was used.
STUDY SETTINGS & PARTICIPANTS
The study included 265 Physical Therapist working in Tertiary Care Hospitals of Karachi.
DATA COLLECTING TOOL AND DATA ANALYSIS
Data was collected through pre-tested, structured and self-administered questionnaire and then, was analyzed on SPSS version 17.
RESULT
This study reported that prevalence of WRLBP was 66.4%. The rate was higher in female physiotherapist, that is, 42.6%. Data revealed that, 69% of respondents experienced WRLBP within 2 years of their practices. Moreover, the manual therapy was found to be the most common cause for WRLBP. No significant association was found between BMI and physical activity level of physical therapist, but interestingly, it was found that sub-specialty area of work was correlated with WRLBP.
CONCLUSION
The rate of WRLBP has been found to be high in physical therapists due to their profession. It is therefore, required to build up an effective ergonomic strategy, strengthen training for prevention at undergraduate level in order to reduce and prevent WRLBP.
Keywords
Musculoskeletal Disorder, Work Related Musculoskeletal Disorder, Low Back Pain, Body Mass Index, Physical Therapist, Physical Activity Level
Saima Javed
Physiotherapist
Anum Jawaid Sultan
Physiotherapist
Dr. M. Usman Khan
Senior Lecturer
Ziauddin College of Physical Therapy
Maria Rahim
Senior Lecturer
Ziauddin College of Physical Therapy
[Javed S, Sultan AJ, Khan MU, Rahim M. Frequency of work-related low back pain among physical therapists.
Pak. j. rehabil. 2013;2(2):38-44]
INTRODUCTION
Occupational health hazards are frequently becoming very common with promotion of industrial life and among these hazards; the prevalence of musculoskeletal disorders has marginally increased. One of the main reasons for this escalation is work related activities1. Health care professionals consistently rank among the most commonly injured occupational groups by musculoskeletal disorders. The U.S. Department of Labor Bureau of Labor Statistics (BLS) indicates that, healthcare support occupations rank first among all professions in terms of sustaining on the job musculoskeletal injuries involving days away from work. The occupational groups (rehabilitation, nurses and other professional healthcare occupations) with musculoskeletal injuries shows absenteeism during working days and are ranked seventh in musculoskeletal injuries. In addition, a growing body of evidence demonstrates significant injury rates among rehabilitation professionals2. Salsi and Ozkan define work related musculoskeletal disorders among physical therapist as a musculoskeletal injury that results from a work related event causing physical disability. Musculoskeletal disorders can affect the body’s muscles, joints, ligaments, tendons and nerves. Work related musculoskeletal disorders can be acute or chronic; mostly they develop over time and are due to work nature directly or develop by the employee’s working environment3,4.
Although Work Related Musculoskeletal Disorders (WRMDs) are common in other anatomical areas like neck, elbow, wrist and hand, but studies reported a high prevalence of LBP5. Several studies have documented that, work related LBP is frequently experienced by physical therapist and they highlighted the prevalence and risk factors of LBP among physical therapist 1,4,5,6. Worldwide, 37% of LBP is related to occupational risk factors6 and in physical therapist, there has been 29% prevalence of work related LBP7. Several studies provided the definition of LBP, the most comprehensive definition accepted is, the pain between the lower margin of 12th rib and gluteal folds whether or not it extends from there to one or both legs 8,9. Cormie et al define work related LBP as, job related ache, pain in low back, and they reported its prevalence as 62.5%. Studies also reported the highest prevalence in younger therapist and the prevalence of initial onset most commonly within first 4 years was reported10.
Work related LBP cases associated with an initial episode could be resolved within 2-4 weeks. It had been observed that, individuals who suffered from WRLBP problems might develop multidimensional disruptions, which could affect their occupations. Physical impact includes the loss of physical function and deteriorated general health. Social impact included decreased participation in social activities. Psychosocial impacts are manifested through insomnia, irritability, anxiety and depression1.
Although physical therapists have expert knowledge about prevention and treatment of musculoskeletal disorder but still, they have higher frequency of LBP and related conditions11. The major cause of LBP in physical therapy profession is the nature of job. The physical therapy practice involves repetitive tasks, high force manual techniques bending/twisting postures, patient transfer assisting with mat activities, lifting heavy equipment. Among them, three most common factors have been documented in previous studies: uncomfortable postures, repetitive task and high force level4-6. Apart from nature of job, WRLBP also relates with specific sub-specialties, gender of physical therapist, body mass index, work experience and working cultures11.
The area of practice for the physical therapist is an important factor for understanding the occurrence of back pain in work related musculoskeletal disorders. Certain sub-specialties contribute LBP more than others and it includes musculoskeletal out patient, neurological rehabilitation, geriatric rehabilitation. Molumphy et al reported that, 18% of physical therapist with WRLBP changed their work setting and that 12% of the physical therapist reduces their patient care hours10.
There is scanty information about the association of WRLBP, BMI and physical activity level of physical therapist. Very few researches are available which provide data on BMI association but the results are in contrast with one another11. No previous researches are available about the association of physical activity level and WRLBP in physical therapist.
Previous researches identify self-protective behavior which include outsourcing, preventive and reactive strategies used by physical therapist to minimize effects and risk of developing Work-related Musculoskeletal Disorder like change in posture, adjust bed height, use of aids and equipment, using a different body part and substituting electro therapy etc7. There have been many studies conducted worldwide on prevalence of WRLBP in physiotherapist. While gathering literature research it was found that, there is no such study conducted in past focusing particularly on this issue in Pakistan. So, the aim for this study is to find out the prevalence of WRLBP among physiotherapist in Karachi, to explores how physical therapist see themselves when they experience WRLBP and to establish information on influencing factors specifically BMI, sub-specialty areas and physical activity level of physical therapist on the occurrence of WRLBP.
METHODOLOGY
Study Design and Setting
A cross-sectional survey was conducted on Physiotherapist in the Physiotherapy Departments of Tertiary Care Hospitals of Karachi from 2012 till 2013 to see the frequency of work-related LBP from occupational hazards.
Sample Size and Technique
Sample size was calculated as 265 by using WHO sample size determination software with 80% power of the test and 95% confidence interval and taking prevalence of LBP among physiotherapist as 29% and margin of error (d) of 6%7. Sample was selected through Non-probability convenience sampling technique.
Inclusion Criteria
All physiotherapists, working in selected settings for at least three months having graduate or post-graduate degree included in the study.
Exclusion Criteria
Those physiotherapists that are not working at present and those who did not give consent were excluded from the study.
Data Collection Procedure
Data was collected through pre-tested, structured and self-administered questionnaire.
Data Analysis Procedure
All qualitative variables are presented as frequency and variables are presented as mean and standard deviation. Chi square test of association is applied with the P value less than 0.05 was considered significant.
Ethical Consideration
All data was handled confidentially and subjects were fully informed about the study objectives. A verbal consent was obtained from the participants after explaining the study prior to their inclusion in the study.
RESULT
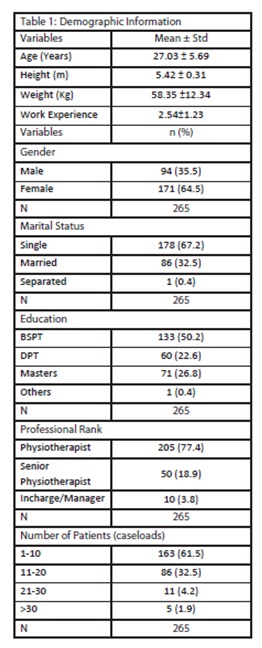
Comprising 64.5% female and 35.5% male physical therapist,in Karachi. Table 1 shows the demographic information ofthe entireparticipant where average age of respondents was 27.03±5.69 year ranging from 21 to 56 years with mean height of 5.42± 0.31 m ranging 4.11 to 6.4 and weight 58.35± 12.34 kg ranging 35.0 to 108. The mean years of experience was observed 2.54± 1.23. The data revealed that, out of 265 respondents, 50.2% had Bachelor in Physical Therapy, 26.8% had Masters’ and only 22.6% pursued Doctor of Physical Therapy Degree. The most common professional rank was Physical Therapist.
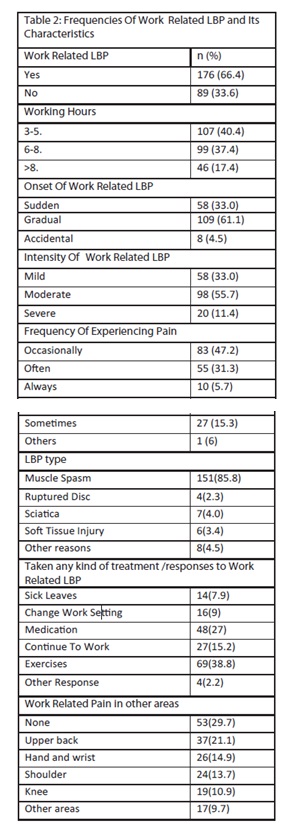
To analyze the frequency of WRLB Pand its characteristics, it was observed that, 66.4% respondents reported that, they had experienced WRLBP at some time in occupational life. In which 42.6% were female and 23.8% were male physical therapist. Upon questioning about, how many hours respondent worked per day in direct patient care, the results indicated that, 40.4% spend 3 – 5 hours per day, and only 17.4% spend more than 8 hours per day.
Majority of participants, that is, 69% experienced their WRLBP within the first two years of clinical practice, 14.2% had first experienced during 2-4 years of practice while 5.7% had it within 4-6years of work. Only 2.3% had their first encounter of WRLBP after 6 years of graduation.
Mostly, the onset of LBP was gradual, for 61.1% participants. On a Visual Analog Scale (VAS), 55.7% described their pain as moderate, 33% as mild and 11.4% as severe. Regarding the frequency of experiencing pain, 47.2% responded occasionally while 31.3 % often experience the pain.
It was observed that, physical therapists are more likely to have WRLBP due to muscle spasm that is 85.8%, which persist for 24 hours or less according to 76.1% respondents. In response to any kind of treatment taken who had suffered from WRLBP,38.8% respondents used their knowledge of exercise while 27% used medication, 15.2% continued their work without any response and 9% changed their work setting due to the risk of sustaining injury.
Figure1: Illustrate proportion of respondents reported contributing factors for LBP
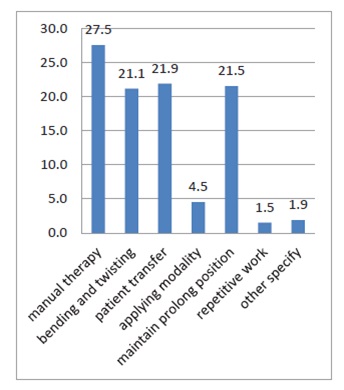
Regarding the Work-Related Pain in other areas, 29.7% clients did not experience any pain. In response to the contributing factors for WRLBP as shown in Figure 1, 27.5% of total participants reported the manual therapy as one of the major causes of LBP while other 21.9% reported due to patient transfer whereas 21.1% felt pain with regards to bending and twisting. Lastly, patients of about21.5% maintained a prolonged position.
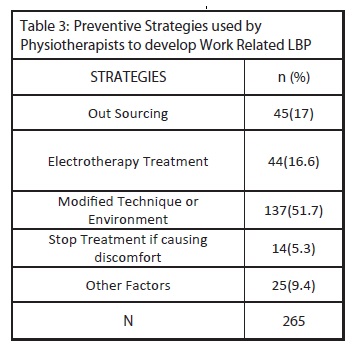
Table 3 exhibits the result of questions stated about preventive and reactive coping strategies from all participants. The most common strategy reported by physical therapists was, modified technique or environment in 51.7% participants while out sourcing strategy was used of about 17%. The use of electrotherapy treatments was recorded to be 16.6% whereas, 5.3% has left the treatment because of discomfort.
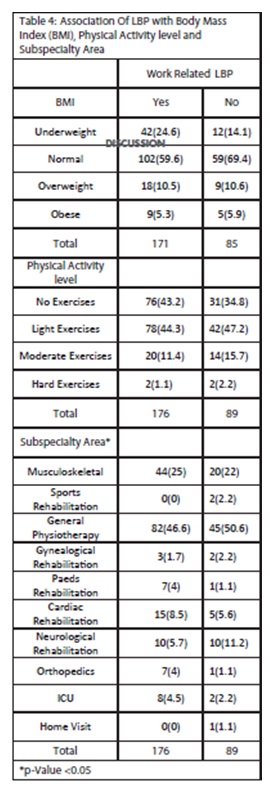
While the significant association was observed between Work related LBP and Subspecialty Area. To analyze the data intensively, the Pearson chi-square method was applied. Firstly, the test was applied to Work related LBP with respect to BMI, apparently, no association was found.
While the significant association was observed between Work related LBP and sub-speciality areas of physical therapy practice, in particular. Those therapists who were occupied in general physical therapy, had high percentage of Work-related LBP 46.6% while the other subspeciality area was 25.0% of musculoskeletal, dominantly.
Analysis of physical activity levels display that; 40.4% physical therapist was not physically active while 45.3% did light exercise. Along with this, 12.8% did moderate exercise and only 1.5%was found to be engaged in hard level of physical activity. Among the respondents, 43.2% were not physically active they were dealing with WRLBP during their work as compared to those who were physically active at low, moderate or hard level respectively.
Table 4 further explains the overall percentage of WRLBP, that is, slightly higher in physically active respondents but the result did not correspond to statistical significance in terms of association between WRLBP and physical activity level. Apparently, it is observed that physical activity is helpful in reducing WRLBP.Interestingly,a major proportion of groups, those who opted to exercise and those who did not, were mutually agreed upon the statement that physical activity is staunchly helpful to reduce WRLBP.
DISCUSSION
Physical therapy is the only profession that demands direct patient care. Although, physical therapists have been trained in bio-mechanical and ergonomics working principal during their undergraduate level program, but the fact cannot be denied that WRLBP is experience regularly by a significant number of physical therapists. The aim of this study is to investigate the frequency of WRLBP all over Karachi and to find out the association between WRLBP and physical activity, Body Mass Index and sub-specialty area. Literature reviews have demonstrated various results from studies that WRLBP in physical therapists have generally been similar, however, some have differed according to region to region.
The results from our study that revealed the prevalence rate of WRLBP for physical therapists was 66.4%, Karachi. On the other hand, the prevalence rate of WRLBP was reported in a range between 22%-74%4. The following percentages of WRLBP were recorded in literature reviews as, in India 36.84%1,4, Saudi and Egypt 23.4%, 33%5,Malaysia 48%11. Whereas in theAfrican region, literature reviews showed52% in Lusaka, 91.3% in Nigeria3,12,13. Furthermore, in Turkey it was notably about 26%14, Korea 53.5%15, Canada 27% and Brazil 78.58%. On the contrary, various other authors have also studied the frequency of Work-related Musculoskeletal Disorder, thus indicating the low back as the most effected part of work-related injury. Moreover, Cormie et al reported 62.5%, Bork et al 45%10 whereas, Mierzejewski and Kumar 49.2%, Scholey and Hair 57%10,16 has their own respective point of views. 36% of WRLBP has been found according to the study done by APTA12. The prevalence rate of our study was much higher in comparison to various other studies, but it was much lower than the prevalence reported in Nigeria.
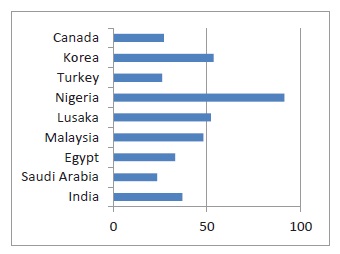
Figure 2: Prevalence of WLBP reported internationally.
The findings showed that, there were more female physical therapists in the survey reported that WRLBP was consistent with responses to similar studies1,5,11. A study of Swedish on a prevalence of work-related musculoskeletal disorders included only female physical therapists who claim low back as the most affected region (56.5%) by work injuries 17,18,19. Previous studies suggested that, this was due to natural body differences in males and females. Generally,
it is found that females are weaker than males, so the factor that causes disadvantage in the task is manual therapy. Females have low pain threshold, this is why, complain about pain more than males1,11. The result of our study shows that there were more females than male physical therapists in the survey with respect to the population from which our sample was drawn.
It is found that the majority of physical therapists experienced first episode of WRLBP within 2 years of practice, this was related to findings of previous researches 5,10. One of the researchers concluded that newly graduated physical therapist had WRLBP in first few years of clinical practice, because they entered in profession with existing risks of LBP from undergraduate trainings. Physical therapist should be alerted to the Work-related LBP risks and its potential causes during their training at student level so they entered in profession with reduced risk of LBP8.
The proportion of 61.9% respondents indicated gradual onset of WRLBP, this outcome was very comparable to those reported in other study3. One of the important findings of our research was most physical therapists 85.8% that reported WRLBP due to muscular spasm which resolved within 24 hours.
People, who suffer injuries on the job, are more likely to be treated with complete bed rest and medication as the basic physiological principles that utter adequate rest after strenuous physical exertion for most favorable recovery20. Survey results indicated being healthcare workers; mostly physical therapists used their 38.8% knowledge of exercise for the relief of WRLBP and only 7.9% preferred to take rest by taking calling off from work. While studying about work related musculoskeletal disorders and behavior of physical therapist, Cromie at al also identified that, most physical therapists used their professional knowledge of relief for WRLBP10. A proportion of 15.2% physical therapists said in our research that, they continuously work without doing any care as acute LBP is self-limiting, but this also showed a reason that why LBP percentage was not declining. Only 9% of physical therapists changed their work setting whereas 17.7% was notably seen as comparison to previousstudy12.
Manual therapy 27.5%, bending and twisting 21.1%, patient transfer, maintaining prolonged position, in this order, were across cutting job tasks or work factors that respondents in the present study commonly identified as contributing to development of WRLBP. The finding of our study was consistent with prior to studies on work-related Musculoskeletal Disorders3,6,7,12,14,16,20.
Bork et al asserted that, physical therapists who apply manual therapy had WRLBP risk that was 3.5 times higher than of those who did not21,22. Bio-mechanical studies have demonstrated very high associated loads during patient handling23 and previous studies have also identified other factors as contributing in WRLBP, but most of them agreed on the point that, the WRLBP in physical therapy profession resulted in combination of factors and no single factor was the main specific cause of WRLBP.
It has been observed in our result that, most frequent preventive strategy was modifying technique and environment, that is, 51.7%. The findings of the study supports the conclusion of the other researchers like, Nkhata et al3, Crome et al, Adejoke et al13, Salik et al14, Chung et al15 and Scholey et al22. In our study, most physical therapists reported that the preventive measure strategy for WRLBP because it may easy for them to modify patient’s position, their own position and treatment techniques rather than to change ergonomics equipment’s use (modality, chair, plinth and so forth) in all working environment according to their own body mechanics. Further, other strategies reported by physical therapists were 17% of outsourcing and stop treatment remained 15.3%. Even though some physical therapists used electro therapy instead of manual therapy, perhaps recorded to be 16.6% but the proportion was not soaring. The previous researches mentioned high use of electro therapy as a preventive strategy for WRLBP19.
Interestingly, our survey found that, prevalence of WRLBP was not related to underweight or overweight of respondents as no significant difference was noted between proportion of physical therapists who had Work related LBP and those who had not in the groups of respondents with Body Mass Index that was greater than 25 and less than 18. In our study, the frequency of WRLBP was high in respondents with normal Body Mass Index. The results were dissimilar with past researches, reported higher occurrence of WRLBP in high Body Mass Indexgroup11.It can be computed that,WRLBP is not related to high and low Body mass index.
The only sub-spatiality areas of practice related to WRLBP were general physical therapy of about 30.9% and musculoskeletal remained 16.6% in our survey. Evidence of high occurrence of WRLBP among physical therapists working in musculoskeletal was documented as well11 but in general, physical therapy area was under reported. Cromie et al reported that, there is no relationship between WRLBP and any particular spatiality area7. Our result may be related to the fact that, in general clinics, the numbers of patients are very high and specialty units/clinics are low in Karachi.
Moreover, in our survey there is no considerable association was found between physical activity and WRLBP. The effects of physical activity on LBP are still controversial. One of the previous studies has shown that, exercise have protective role for WRLBP whereas, other reported sports activity as a risk factor for LBP1.Furthermore, Sitthipornvorakul et al in their systematic review states the association between neck & LBP and physical activity, thus, concluded that conflicting evidences were found about physical activity and its effects on LBP and further exertion is required to establish the clear result20.Likewise, Hendrick et al also mentioned in their systemic review that no evidence was found for detrimental effects from engaging in higher level of physical activity in LBP 21,24,25
CONCLUSION
After going through the hard-core analysis, we have drawn the conclusion that, the prevalence of WRLBP among physical therapist in Karachi is as high as those reported in other areas of developed and developing countries. Moreover, it was also found that females were more prone to get WRLBP than males and that of higher rate was projected for newly graduates of physical therapist in general physical therapy. Physical Therapy becomes the vast yet most demanding healthcare profession. As for now, considering above facts, it is required to build up effective ergonomics strategy, strengthen training programs for preventing health hazards at under-graduates’ level in order to reduce Work Related Low Back Pain.
REFERENCE
- Shah S, Dave B. Prevalence of LBP and its associated risk factors among doctors in Surat. IJHSR 2012;2(1):91–102.
- Arnold M, Radawiec S, Camop M, Nordin M. Changes in functional independence measure rating associated with safe pt. handling and movement program. Rehab. Nursing2011;36(4):138–44.
- Nkhata LA, Zyaambo C, Nzala SH, siziya S. Work related musculoskeletal disorder: prevalence, contributing factor and coping strategies among physical therapy personal in Lusaka, Kitwe and Ndola district, Zambia. Med J Zambia 2010;37(4):262-7.
- Buddhadev NP, Kotecha IS. Work related musculoskeletal disorders: a survey of physiotherapists in saurashtra region. National J Med Research 2012;2(2):179-81.
- Al Eisa E, Buragadda S, Shaheen AM, Ibrahim A, Melam GR. Work related musculoskeletal disorders: causes prevalence and response among Egyptian and Saudi physical therapist. Middle East J. Scientific research 2012;12(4):523–29.
- Falavigna A, Teles AR, Mazzocchin T, Braga GL, Kleber FD, Santin GT et al. Increased prevalence of LBP among physical therapy student compare to medical students. Euro spine J 2011;20(3):500–5.
- Cormie JE, Robertson VJ, Best MO. Work related musculoskeletal disorder in Physical Therapist: prevalence severity risk and responses. J. American Physical Therapy Assoc 2000;80:336-51.
- Nyland JL, Grimmer KA. Is undergraduate physical therapist study a risk factor for LBP? A prevalence study of LBP in PT student. BMC musculoskeletal disorders. 2003;4:22.
- Louw QA, Morris LD, Somers KG. The prevalence of LBP in Africa: a systematic review. BMC musculoskeletal disorders 2007;8:105.
- Cormie JE, Robertson VJ, Best MO. works related musculoskeletal disorder and culture of physical therapy. Phy Thera 2002;82(5):459–72.
- Nourdin NA, Leonard JH. The work related injuries among public hospitals – a South East Asian Picture. Clinic Sao Paulo 2011;66(3):373–78.
- Campo M, Weiser S, Koenig KL, Nordin M. Work related musculoskeletal disorder a prospective cohort study with one year follow up. Phys Ther 2008;88(5):608–19.
- Babatunde OA, Akodu KA, Oyeyemi AL. Workrelated musculoskeletal disorders among Nigerian Physiotherapists. BMC Musculoskeletal Disorders 2008;9:112.
- Salik Y, Ozcan A. Work-related musculoskeletal disorders: A survey of physical therapists in Izmir- Turkey. BMC Musculoskeletal Disorders 2004;5:27.
- Chung SH, Her JH, Ko T. Work related musculoskeletal disorders among Korean physiotherapist. J. of Phy ther Sci 2013:25:55-9.
- Marras WS, Davis KG, Kirking BC, Bertsche PK. A comprehensive analysis of low back disorders risk and spinal loading during the transferring and repositioning of patients using different techniques. Ergo 1999;42(7):904-26.
- Soket JH, Essendrop M, Hansen AF. A dynamic 3d bio mechanics evaluation of load on LB during different patient handling task. J. Bio Mech 2002;35(10):1357–66.
- Robertson VJ, Spurritt D. Implications of EPA availability and use in undergraduate clinical placements. Physiotherapy 1998;84:335-44.
- Mierzejewski M, Kumar S. Prevalence of low back pain among physical therapists in Edmonton, Canada. Disabil Rehabil 1997;19(8):309-7.
- Sitthipornvorakul E, Janwantanakul P, Purepong N. The association between physical activity and neck and low back pain: a systematic review. Eur Spine J 2011;20:677–89.
- Hendrick P, Milosavljevic L, Hate. The relationship between physical activity and low back pain outcomes: a systematic review of observational studies. Eur Spine J 2011;20:464–74.
- Scholey, M, and M Hai. Back pain in physiotherapist involved in back care education. Ergonomics 1989;32(2):179–90.
- Grooten WJ, Wernstedt P, Campo M. Work related musculoskeletal disorders in female Swedish physical therapist with more than 15 years of job experience: prevalence and association with work exposers. Physiother theory practice 2011;27(3):213-22.
- Andersen L, Clausen T, Persson R. perceived physical exertion during health care work and prognosis for recovery from long term pain in different body regions: prospective cohort study. BMC Musculoskeletal disorders 2012;13:253.
- Siqueira GR, Cahú FGM, Vieira RAG. Occurrence of low back pain in physical therapists from the city of Recife, Pernambuco, Brazil. Braz. J. Phys. Ther. Rev Bras Fisioter 2008;12(3):222-7.