
ABSTRACT
BACKGROUND
Trauma is globally encountered in the emergency department on regular intervals placing a burden on the economy through an increase in the mortality and morbidity. Multiple types of fractures have been notified leading from moderate to severe disability.
OBJECTIVE
The aim of the study is to assess different types of fracture entering the emergency department, the risk of these fractures and also to find the association between genders.
STUDY DESIGN AND SETTING
A cross sectional survey was conducted on 450 participants in different Emergency Departments of tertiary care units of Karachi.
RESULT
It has been observed that fracture cases are increasing in emergencies in Karachi. Road Traffic Injuries (RTA) with 41.6% is the most dominant cause of fracture whereas fall or slip injuries and brawl/fight show 22.2% and 14.7% respectively. Generally, alcohol and cigarette smoking has adverse effect yet 91.6% population revealed no relationship. Regional distribution of fracture shows lower limb fracture with 40.9% as most commonly occurring fractures where male percentages is higher than females. The selected population presented no idea about BMD and Vitamin D test which causes fractures in old age commonly.
Keywords
Fractures, Accidents, Trauma, Emergency Department, Violence, Fall, Upper Extremity, Lower Extremity
Pawan Rekha
Student PPDPT
Ziauddin College of Physical Therapy
Ziauddin University
Sheena Kumari
Student PPDPT
Ziauddin College of Physical Therapy
Ziauddin University
Amna Aamir Khan
Assistant Professor
Ziauddin College of Physical Therapy
Ziauddin University
[Rekha P, Kumari S, Khan AA.Frequency and type of Fracturesentering the Emergency Units of Orthopedic Hospitals. Pak. j. rehabil.2013;2(2):21-26]
INTRODUCTION
Trauma, the leading cause of mortality is globally encountered in the emergency department on regular intervals1. In United States (US), it is considered as the leading cause of death for those under the age of 35 and accounts for 10 percent of all deaths between both men and women2. In addition, injuries from accidental trauma worldwide leave over 45 million people each year with moderate to severe disability1 and annually receiving medical care for more than 50 million patients. It also accounts for admission of approximately 30 percent of patients in all intensive care unit3,4.
In the first national injury survey in Pakistan, revealed the yearly overall incidence of traumatic injury was found to be 41 injuries for every 1000 persons5. The survey also identified Road Traffic Injuries (RTA) as one of the major causal factors for injury presenting to emergency. Moreover terrorism, nutritional deficiencies, domestic violence, growing number of elder populations is also contributing to life time disability. Road traffic injuries have a yearly incidence of 15 injuries for every 1000 persons5. It has been interesting to know that children injured in road traffic accident tend to have uneducated mothers when compared to non-injured controls6. In addition to the road traffic accident violence plays an essential role also, primarily affecting wage earners and can include intimate partner vehemence to war. Researchers have been keen to assess the magnitude of intimate partner violence in Pakistan on multiple occasions. It has been indicated that 44% of women experience lifetime marital physical abuse7. During the last five years in the city of Karachi 58 bomb blasts in this city alone has been reported, resulting in 689 injuries and 164 deaths resulting in several musculoskeletal problems and disabilities8. These injuries comprise of approximately 12 percent of the 10 million annual visits to US pediatric Emergency Departments (EDs)9 resulting in skeletal fractures and causing considerable cost and morbidity for the children. Despite of aggressive campaigns for injury prevention, the overall rate of fractures has been increasing 10,11, and approximately half of all children would fracture a bone during childhood12. It has been observed and documented that the periosteal of pediatric bone has significant osteogenic potential and is comparatively more metabolically active, thicker, and stronger than the adult. Which limits in fracture displacement, reducing the likelihood of open fractures, and maintaining stability 13,14. These qualities and function of periosteal are responsible for some of the unique fracture patterns including buckle, greenstick, and plastic deformation (or bowing) 13,15,16. However Upper extremity fractures in adults are also documented on high account in approximately 2 million emergency departmental visits annually in USA 17. 8 percent of the visits are for humeral fractures; 31 percent for radial /ulnar fractures; and 51 percent for carpal, metacarpal, or phalangeal fractures. Interestingly, falls has been acknowledged as the leading cause of upper extremity fractures18. No significant work has been conducted to assess the frequency of different types of fractures entering the emergency units of tertiary care hospitals. Keeping in mind the cosmopolitan status of the city it is imperative that research leading to the beneficial in identification of common fractures and improvising the preliminary care should be given in these scenarios.
MATERIALS AND METHODS
Study Design
A cross sectional, study was conducted in tertiary care hospitals of Karachi by one year survey after the acceptance from the ethical review committee. A sample of convenience was used to collect the data was collected by two therapists by personal interview. It was considered that the interviewer has no language barrier.
Inclusion/Exclusion Criteria
All the conscious patients entering the ED were selected for the study. These patients represented of single fractured bone. The questionnaires for children and old aged patients were completed by their guardians and representatives. The patients on ventilators, with blast injuries cases were excluded from the study as most of them were expired in intensive care unit and others are non-responsive to questions or multiple complications were excluded from the study.
Data Collection Procedure
384 subjects were included in the study for which the sample size was calculated on the basis of prevalence which was taken at 50% because no relevant data was available. The bound of error has been taken at 5% with 95% of confidence. As it was a cross-sectional survey so in order to avoid the non-response of the participants the sample size is inflated to 450, to exclude non-response and incompletely filled questionnaires.
The questionnaires were administered to the 450 participants aged between 10-90 years, to determine the demographic information such as (age, gender, and occupation). While filling the interview based questionnaire the medium of language was taken into account to be easily understandable to both the researcher as well as subjects to provide a comfortable and secured ambience.
All participants personal details such as area of residence and economic conditions were also inquired. The type of fracture, history of any disease and previous fracture was used to audit the frequency of fracture. The RTA by vehicles included both the drivers and passengers whereas others involved fall slip. The trauma caused by pathology and due to deficiency of Vitamin D was also documented in the questionnair Fractures resulting from domestic violence were also included. The study also checked to see the effect of alcoholism and smoking on bone mineral density and n fracture. The outcomes of variables were incorporated in performa and analyzed.
Data Analysis Procedure
Data was entered using the SPSS version 20. Before the start of analysis the data was cleaned for possible data entry errors. Frequencies and percentages were taken out for categorical variables. Association between gender and type of fracture was assessed through application of Chi Square test.
RESULTS
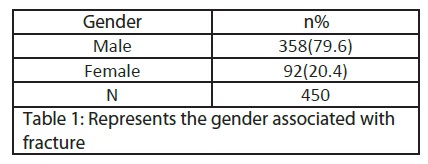
A total of 450 cases of fracture were assessed during 12 months of period with 79.6% males and 20.4% of females showing a vast difference between both the genders. The average age is documented to be 35.8 years.
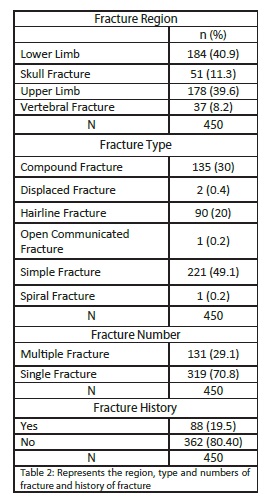
The questionnaire basically focused on the region and type of fractures and the results are summarized in Table 2. It was noted that 40.9% of fractures were of lower limb whereas vertebral fractures were only 8.2%. The estimated percentage of simple fracture among both the gender was 49.1%. Fracture of other types such as displaced, open communicated and spinal in total occurred only 0.8% in the ED. Compound fracture 135 (30%) and hairline fracture 90 (20%) were also noted. Interestingly, only 19.5% of people revealed previous fracture history.
Interestingly, drivers/labors, women and students were the mostly common among occupations entering the ED. Among 92 women 56% of women were noted to be housewives.
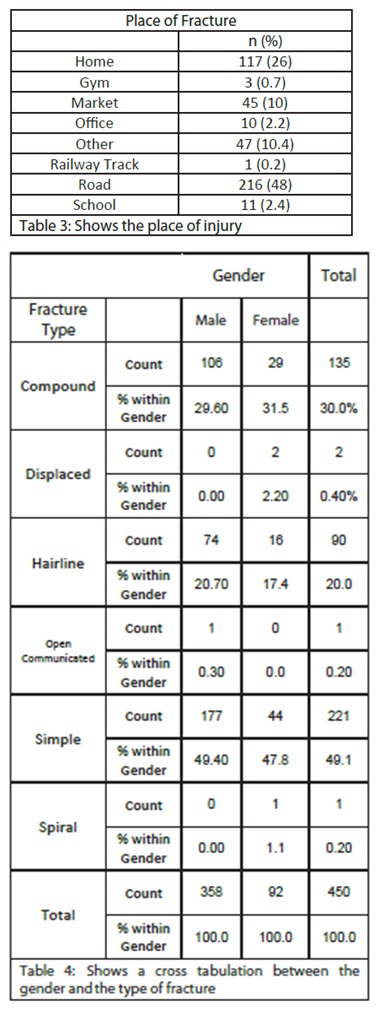
The prevalence of Road Traffic Accident was noted to be highest in both the genders 48% as compared to other factors of fractures. Marked difference was observed among home injuries 26% and other factors; gym 0.7% and railway track 0.2% yet market fractures were still experiential 10%.
Interesting results are obtained while performing a cross tabulation between the type of fracture and the gender (Table 4). Simple fracture was dominant both in males (49.4%) and females (47.8%). Compound fracture showed the dominancy in female gender (31.5%). The remaining fractures were all higher in males. A Pearson Chi-square test was performed and Significant association between the type of fracture and gender P=0.02 (P<0.05) was obtained.
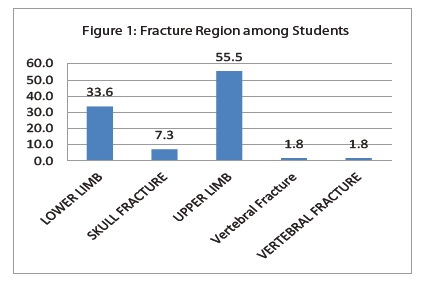
Figure 1 represents students were highest in the population 110, interesting results were drawn from it. The prevalence of upper limb fracture was highest (55.5%) when compared with lower extremity (33.6%) and skull fracture (7.3%).
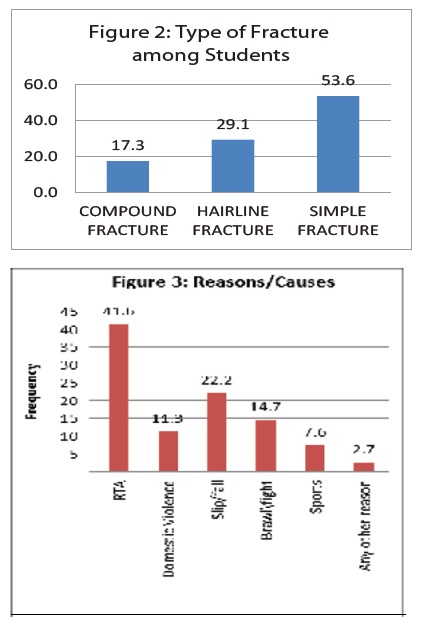
`However simple fracture as being the highest in the results is also dominant among students 53.6% (Figure 2). After RTA fall brawl seems most common reasons. Study also shows that most falls took place at home with hard flooring 38.9 % others including wet area 9%, rough surface 29.3%, and smooth surface 19.3% (Table 5, Figure 3)
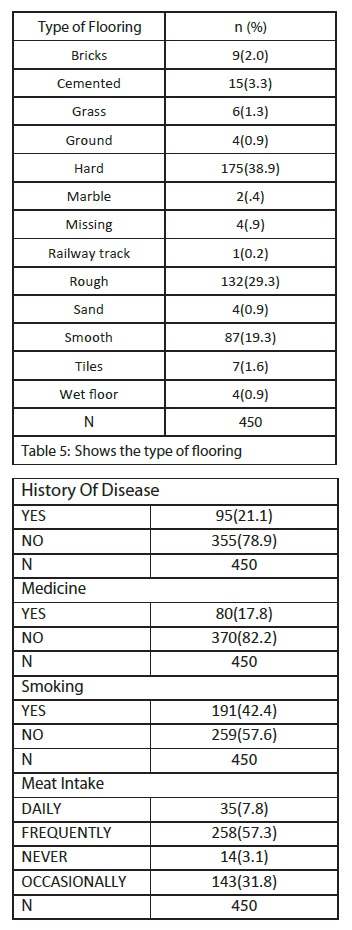
Table 6 shows only 20% of women participated in the study but no significant changes were observed for calcium and vitamin D levels between the genders. However, good protein diet is one of the most important factors which can decrease the overall fracture ratio selected samples were showing following percentage of protein intake in their diet on daily bases; milk 32%, eggs 14%, meat 7.8 %. Although frequent intake of milk, meat, and egg was highest in all the categories; milk: 36.9%, egg: 43.3% and meat: 57.3%. 78.9% had no any previous history of any chronic disease and 82.2% of all not taking any medicine that may cause any adverse effects on their bones.
DISCUSSION
Fractures are the misfortune or unexpected event which may cause life time problems. The basic focus of this study is to determine the expected and unexpected causes of fractures and their frequencies entering the ED. With the advent of time, the increasing numbers in emergencies has affected the economy of both the developed and under developed countries. The motive of this study is to create awareness among the people about the causes in order to control it. According to the 1996 World Health Organization report (WHO) injury ranks fifth among all causes of death and accounting for 5.2% of all mortality worldwide. It is a leading cause of death and disability for people under 45 years in the industrialized world. These rates are declining in developed countries but injuries are important and a largely neglected health problem in developing countries19.
Road Traffic Accidents (RTAs) and injuries related to them are the biggest threat coupled with a challenge to the upcoming world. Likewise, highest number of RTA; 48% were the causes of fractures entering the Emergency Department. Interestingly, the disproportionately high incidence in males 79.6% to 20.4% females is associated, to a significant extent, with greater exposure to driving as well as to patterns of high-risk behavior when driving. And ratio of males to females is high. Unfortunately, Karachi is facing one of the highest numbers of accidents in Pakistan, especially due to bike riders, resulting in fatal outcomes mostly leading to disability yet. Unfortunately, only fracture was part of this study so disability was not identified. Based on the facts and figures of accidents reported at the city`s trauma centers between Jan 1 and March 31 2013, the report stated that 304 people died in the accidents and 1,377 people received serious injuries, becoming almost paralyzed for life. “Of the total 304 fatalities, 48 per cent were pedestrians, 30 per cent motorcycle riders, 16 per cent passengers, and four per cent drivers.” Forecasting specify that these statistics will rise by about 65% over the upcoming 20 years if there is no new commitment to prevention.
In a study conducted by Verma and Tewari in Delhi, total number of injuries was more in the age group of 15-35 years (69% that is 470 out of 680). Similar results with different percentage were obtained in our study 20,21-24. Moreover, students were the most vulnerable group in our study (24.4% i.e., 110 students out of 450). The reason behind this could be the reckless driving of the students and most of them not following the traffic rules and others are unaware of it. On the other hand, lower limb fracture due to RTA and fall remains most common.
Previous researches have revealed violence as primarily affecting fractures mostly due to partner violence. The magnitude of intimate partner violence in Pakistan indicated that 44% of women experience lifetime marital physical abuse25 but unfortunately only 11.3% was represented in our study. Moreover, violence against women is public health concern of considerable importance in developed and developing countries both. Muslim societies have been criticized for violating women right particularly. A study conducted by Fariyal et al, on the attitudes of Pakistani men towards abuse on wife and domestic violence a total of 176 married couple were interviewed, with hitting, punching and slapping, 8% fractures had sustained by their wives as consequence of physical abuse26. Our study also reveals the nature of more serious fractures. The main reason of this violence is poverty frustration and depression. Since Epidemiological studies suggest that lower vitamin-D {25(OH) D} status is associated with a higher risk for osteoporotic fractures, a study was conducted at various hospitals in Karachi from April 2007 to September 200727. It concluded that prevalence of hypo-vitaminosis D among healthy Pakistanis is high and duration of sun exposure is the most common predictor of it 27. Although Vitamin D deficiency and low BMD value are the one of the significant factors leading to fractures yet subject selected in our study were unaware of this as 94.9% had no scan done. The reason behind it is assumed to be lack of education and the second reason is poor financial status. Advancing age, longer duration of menopause, multi parity, low BMI, poor socioeconomic conditions were found to be significant risk factors in women presenting with hip fractures28. Our study indicates fall/fight as second most common cause of fracture. Falling on hard surface causes a serious head and lower limb vertebral injury that is clearly represented in our results. This may be fatal and cause life time disability. Beside other important factors dietary component was another outcome measure of this study. As most of the populations are consuming low calcium diet and no supplements are added to them. Our study clearly shows that 81.7% of respondents do not use calcium supplements in their diet especially among labors increasing the risk of fracture. A study was conducted for traumatic spine fracture incidence in Tehran, Iran, was 16.35 (95%CI: 3.4-48.0) per 100,00029. The incidence of TSF in males was more than twice that of females29. A prospective study was conducted in Ethiopia aimed at determining the causes, magnitude, radiological and clinical patterns of major limb fractures in adults. 422 orthopedic adult patients sustained a major fracture of their limbs. Mean age was 35 years with a male to female ratio was 3:1. Pathological fractures were encountered only in two (0.5%) patients. Nearly 48% of the traumatic fractures were due to road traffic accidents. The highest frequency of fracture occurred on the femur (68, 15%)19. Contrasting results were obtained while comparing to our present data where higher frequency was obtained when compared with vertebral fractures. Previously, a study was conducted to quantify the global burden of osteoporotic fracture worldwide in year 2000, where an estimated 9.0 million osteoporotic fractures of which 1.6 million were at the hip, 1.7 million at the forearm and 1.4 million were clinical vertebral fractures30. Pathological fractures are found to be uncommon in this study.
A number of contrasting results were obtained in our study when compared with previous researches. The basic reason was due to unequal gender difference male: female (4:1). In addition, the study should be conducted on larger scale and higher sample size to obtain better results.
CONCLUSION
Globally, the frequency of fractures is increasing with the passage of time, causing activity limitation and participant restriction. These are directly and indirectly affecting the activities of daily living. Higher scale researches should be conducted identifying types of fractures in both the study. Awareness programs are essential in the lower socio-economical class to improve their healthy diet that is beneficial to their bones and joints. Besides this there should be policies about traffic safety and common man should be responsive towards illiteracy having poor financial status disturbing their marital life and causing domestic violence on females that needs to be controlled.
REFERENCES
- World Health Organization. Global burden of disease. www.who.int/healthinfo/global_burden_ disease/en/ (Accessed on May 01, 2010).
- Feliciano DV, Mattox K, Moore EE. Trauma, 6th, McGraw-Hill, New York 2008.
- National estimates of the ten leading causes of nonfatal injuries, Centers for Disease Control and Prevention 2004. www.cdc.gov/injury/wisqars.html (Accessed on May 24, 2010).
- Mackenzie EJ, Rivera FP, Jurkovich GJ. The National Study on Costs and Outcomes of Trauma. J Trauma 2007;63:S54.
- Gaffer A, Hyder AA, Masud TI. The burden of road traffic injuries in developing countries: the 1st national injury survey of Pakistan. Public Health 2004;118:211-7.
- Singer MS, Gaffer A. Risk factors for road traffic injury in Pakistani children. J Coll Physicians Surg Pak 2004;14:709-12.
- Fikree FF, Jafarey SN, Korejo R, Afshan A, Durocher JM. Intimate partner violence before and during pregnancy: experiences of postpartum women in Karachi, Pakistan. J Pak Med Assoc 2006;56:252-7.
- Mehmood A, Razzak J, Khan S J. Blast injuries in Karachi. In: Health Sciences Research Assembly 2007, Abstract Book. The Aga Khan University, Karachi, Pakistan; 2007.
- Chamberlain JM, Patel KM, Pollack MM. Recalibration of the pediatric risk of admission score using a multi-institutional sample. Ann Emerg Med 2004;43:461.
- Khosla S, Melton LJ 3rd, Dekutoski MB, Achenbach SJ, Oberg AL, Riggs BL. Incidence of childhood distal forearm fractures over 30 years: a population- based study. JAMA 2003;290:1479.
- Jónsson B, Bengnér U, Redlund-Johnell I, Johnell O. Forearm fractures in Malmö, Sweden. Changes in the incidence occurring during the 1950s, 1980s and 1990s. Acta Orthop Scand. 1999;70(2):129-32.
- Jones IE, Williams SM, Dow N, Goulding A. How many children remain fracture-free during growth? A longitudinal study of children and adolescents participating in the Dunedin Multidisciplinary Health and Development Study. Osteoporos Int 2002;13(12):990-5.
- Carson S, Woolridge DP, Colletti J, Kilgore K. Pediatric upper extremity injuries. Pediatr Clin North Am 2006; 53(1):41-67.
- Della-Giustina K, Della-Giustina DA. Emergency department evaluation and treatment of pediatric orthopedic injuries. Emerg Med Clin North Am 1999;17(4):895-992.
- Frost HM, Schönau E. The “muscle-bone unit” in children and adolescents: a 2000 overview. JPediatr Endocrinol Metab 2000; 13(6):571-90.
- Specker BL, Brazerol W, Tsang RC, Levin R, Searcy J, Steichen J. Bone mineral content in children 1 to 6 years of age. Detectable sexdifferences after 4 years of age. Am J Dis Child 1987;141:343
- American Academy of Orthopaedic Surgeons. Number (in thousands) of emergency department visits for fracture: 2006. http://www.aaos.org/research/ stats/ER_Visits_Fracture.pdf. Accessed July 28, 2009.
- Chung KC, Spilson SV. The frequency and epidemiology of hand and forearm fractures in the United States. J Hand Surg Am 2001;26(5):908–915
- Admasie D, Tekle YY, Wamisho BL. Radiological and Clinical Details of Major Adult Limb Fractures in a Teaching Hospital, AAU, Ethiopia. ECAJS March-April 2009;14(1):88-97
- Jha N, Agarwal Ch. Epidemiological Study of Road Traffic Accident Cases: ASt From E a s t e r n Nepal. Regional Health Forum, WHO South-East Asia region 2004;8(1):15-22
- Jha N. Road traffic accidents case sat BPKIHS, Dhahran, Nepal: One year in retrospect. J Nep Med Assoc 1997;35:241-244
- Mehta SP. An epidemiological study of road traffic accident Cases admitted in Safdar jang Hospital, New Delhi, Indian J Med Res 1968;56(4):456-66
- Ghosh PK. Epidemiological study of the victims of vehicular ac- accidents in Delhi. JIMA 1992;90(12):309-312
- Verma PK, Tiwari KN. Epidemiology of Road Traffic injuries in Delhi: result of a Survey. regional Health Forum, WHO South-East Asia region 2004;8:(1);1-10
- Singer MS, Gaffer A. Risk factors for road traffic injury in Pakistani children. J Coll Physicians Surg Pak 2004;14:709-12.
- Fikree FF, Razzak JA, Durocher J. Attitudes of Pakistani men to domestic violence. J Mens Health 2005;2(1):49-58
- Mahmood K, Akhtar ST, Talib A, Haider I. Vitamin-D status in a Population of Healthy Adults in Pakistan. Pak J Med Sci 2009;25(4):545-550.
- Mamgi MF, Hasan JA, Sabri MS. Risk Factors for Osteoporosis in Post- Menopausal Women with Hip Fractures. JSP (Int) April–June 2010:15(2);82-86
- Moradi-Lakeh M, Rasouli MR, Vaccaro AR, Saadat S, Zarei MR, Rahimi-Movaghar V. Burden of traumatic spine fractures in Tehran, Iran. BMC Public Health 2011;11:789. doi:10.1186/1471-2458-11-789
- Johnell O, Kanis JA. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int 2006;17(12):1726-1733.