
ABSTRACT
OBJECTIVES
To compare the effectiveness of Maitland technique (Grade IV) and Mulligan technique for the treatment of frozen shoulders.
STUDY DESIGN
Experimental Study.
STUDY SETTINGS & PARTICIPANTS
This study has been conducted at Ziauddin Hospital with 50 volunteers who participated in the study that were equally divided into two groups (pre and post treatment groups). Subjects were randomly assigned to each group.
INTERVENTIONS
Intervention given to Group A was Maitland Technique (Grade IV) and Group B, Mulligan Technique.
OUTCOME MEASURES
Functional activity of shoulder is measured by using Shoulder Pain and Disability Index (SPADI) score, Pain is measured by VAS Score, and Range of motion, measured by Goniometer both before and after treatment.
RESULTS
Both the treatments showed positive results but Mulligan technique was found to be more effective. The total SPADI score was 15.48 before and 11.92 after the Mulligan technique and 15.32 before and 13.16 after the Maitland technique.
CONCLUSIONS
It is evident that Mulligan technique is more effective for the treatment of frozen shoulder compared to Maitland technique.
Key Words
Frozen Shoulder, Maitland Technique, Mulligan Technique, Shoulder Pain And Disability Index (SPADI), Range of Motion (ROM), Visual Analogue Scale (VAS)
Syed Abid Mehdi Kazmi
Manager
Department of Physiotherapy
Ziauddin Hospital
Jharna Devi
Senior Physiotherapist
Department of Physical Therapy
ZIauddin Hospital
Faisal Yamin
Senior Lecturer
Institute of Physical Medicine and Rehabilitation
Dow University of Health Sciences
Sunil Kumar
Fellow Infectious Disease SIUT
[Kazmi SAM, Devi J, Yamin F, Kumar S. Comparative Study on the Efficacy of Maitland Technique (Grade IV) and Mulligan Technique, in the Treatment of Frozen Shoulder. Pak. j. rehabil. 2013;2(1):10-14]
INTRODUCTION
Adhesive capsulitis is one of the most common causes of all peripheral joint disorders. The shoulder is made to stretch and produce a large amount of movement, where few movements take place through the shoulder blade and chest wall; however, many movements come about through ball and socket joint1. The frozen shoulder also known as adhesive capsulitis is a situation where shoulder joint becomes very stiff, painful and tight, further the shoulder joint is also inflamed that ultimately leads to shoulder pain and restricted Range of Motion (ROM) of shoulder in capsulitis pattern2. The patient initially suffers from the situation of pain or freezing, later the condition of frozen and finally defrosting condition characterized by the limited ROM3,4. The capsular pattern in the shoulder is characterized mostly with the limitation of passive lateral abduction and rotation.
The presence of capsular pattern referred to diagnosis of shoulder capsulitis. Whereas, ROM differs on the condition of the patient, on which stage of capsulitis the patient is, yet he or she still has limitations of passive ROM in a capsular pattern5. The Adhesive capsulitis is categorized through insidious & progressive loss of active and passive mobility in glenohumeral joint likely because of capsular contracture, however the researches have been conducted in last century, etiology and pathology of frozen shoulder remain enigmatic6,7.
According to Reeves, Adhesive capsulitis has three stages of disease:
Stage 1: Characterized by pain lasting 2 – 9 months.
Stage 2: Pain sub-sides, but stiffness is marked lasting 4 – 12 months.
Stage 3: Pain resolves an improvement in the range of motion.
Where II and III stages of adhesive capsulitis and ROM are considerably restricted, where restriction of movement is in the capsular pattern i.e., external rotation is most limited, followed by limitation in abduction and internal rotation respectively8.
However, some authors have describes the frozen shoulder in primary frozen shoulder, that leads to which corresponds to idiopathic. The secondary corresponds to traumatic capsulitis or if some other medical condition is present alongside9. Actually, it persist for longer period as compared to stated period, whereas, it does not completely recovers, it never gets full recovery. The purpose of the treatment is to get the relief, sustain the range of motion and ultimately to restore function. The clinical syndrome includes limited ROM, muscle weakness and pain. However, few researchers have debated that frozen shoulder is a self-restricting disease lasting as little as 6 months; further some more researchers recommended that frozen shoulder is more prolonged disorder causing long term disability. Adhesive capsulitis is more reactive in the; diabetic patients as compare to general population. It ranges from 10% to 20% in the diabetic patients10, whereas, in contrast to that it is only 2% to 5% in the general public11. Furthermore, it is more common in the females as well with age range of about 40 to 70 years, where the probability of recurrence is very minimal.
Various treatment exists for the treatment of adhesive capsulitis, which ranges from rest and analgesics, physical therapy, electrotherapy, arthroscopic/open surgery, injections, acupuncture, manipulation under anesthesia and Corticosteroid, exercise, Transcutaneous electrical nerve simulation (TENS), Ultrasound, deep heat and ice, whereas, as such no treatment is being considered as standard treatment12.
Maitland Grade IV Technique
The Maitland concept is a process of analyzing, investigating and also for the treatment of neuromusculoskeletal disorder through manipulative physiiotherapy13. There are V grades of Maitland Techniques, discussed as follows:1
I: Minor amplitude in the start of ROM
II: Large amplitude could not touching end of ROM
III: Large amplitude touching restricted ROM
IV: Minor amplitude at end of restricted ROM
IV: Minor amplitude and high speed at end of restricted ROM
Whereas, the Grade I & II are mainly applied for the treatment of the joints limited with pain. The vacillations can have inhibitory effect on perception of painful stimuli through frequently motivating mechanoreceptors which block nociceptive pathways at the brain stem levels or spinal cord. Those no stretch motions can help in moving synovial fluid in improving nutrition of cartilage. Appropriate selection of mobilization technique for treatment can only take place after a thorough assessment and examination15. As mentioned above, the capsulitis is challenging for therapeutic as well as rehabilitation purposes.
Mulligan Technique
Mulligan’s Mobilization with Movement (MWM) is nowadays getting reputation in the treatment of the musculoskeletal situations. Mulligan in 199316 explained it is a manual therapy, where the force is being applied in the form of Glide, on the motion position and it is applied in the condition when the impaired joint could freely move along pain/impediment. It has been highlighted that the treatment through the MWM yields its impact by rectifying the faulty positions of the joints, which occurred due to strains or the injuries17,18. Mulligan technique is applied for reducing the pain and improves functionality in the patient of adhesive capsulitis and reduces stiffness of shoulder.
Mulligan’s technique is being applied in flexion, elevation and internal rotation, where 3 sets of ten repetitions can be applied having rest intervals of 30’s during each set. Patients were treated for 5 days per week for 3 weeks19.
Kochar and Dogra (2002) concluded through quasirandomized- clinical Mobilization in addition to Mulligan & adding with the ultrasound (US), by randomizing the 66 subjects into three groups, one group is unable to visit hospital for the physiotherapy. Where, the 10 treatment sessions were arranged for the treatment, where the treatment was given through MWM and US, it was delivered within 1st three weeks & continued with a progressive exercise regime till next 9 weeks. The measurement was evaluated through Pain Visual Analogue Scale (VAS) of 10 cm, a weight lifting test, grip strength and self-assessment of patients. It concluded that the combination of MWM and US yields better results as compared to US only. The group who got the treatment through the combination of MWM and US showed 07% improvements as evaluated through PVAS scale20.
Poonam and Neeti (2010) conducted the study that Maitland technique yields immediate pain relief along with increase in ROM. The study was conducted on the 50 randomly selected patients suffering from the frozen shoulder to check the efficacy of the two treatments; one is Maitland glide & hot pack while other is Active Exercise & hot pack. They concluded that there is significant improvement in the patients got treatment of Maitland with hot pack as compared to active exercise with hot pack21. Teys et al. stated that clinically meaningful improvements in both ROM and pressure pain threshold occur immediately after the application of Mulligan’s technique in the pain-limited shoulder22.
METHODS
Convenience sampling design is used on the OPD patients at Ziauddin Hospital. The study has been conducted on the 25 random patients suffering from Adhesive capsulitis that include both male and female patients. The consent was taken from each subject before participating into the study, thereafter; the subjects were randomly divided into groups after evaluating the inclusion and exclusion criteria. Where, randomization was executed with the help of random numbers in each group.
Group A
25 patients were selected with age range of 35 to 60 years. Group A was treated with the Maitland technique IV.
Group B
25 patients were selected with age range of 35 to 60 years. Group B was treated with the Mulligan technique.
Variable of the Study
In the study following variables are being tested:
- Shoulder pain and disability index (SPADI)
- Ranges of Motion (external rotation and abduction)
Inclusion Criteria
Patients fulfilling following criteria were included in the study:
- Patient within age bracket of 35 years to 60 years
- Pain in shoulder movement for the period of at least 2 months
- Diagnosed frozen shoulder or adhesive capsulitis
Exclusion Criteria
- The patients with radiological investigation were not included in the study
- Patients with Inflammatory arthritis were not included in the study.
- Post fracture complication, neurological involvement, diabetic patient or any cardiac disorder.
Study Setting
The study is being conducted on fifty patients including male and female, with age range of 35 years to 60 years. The patients were diagnosed Adhesive Capsulitis by the orthopedic doctor and recommended to the Physiotherapy department of North Nazimabad and Clifton Campus of Ziauddin Hospital, Karachi.
Study Duration
The study has been conducted on the outdoor (OPD) patients of Ziauddin Hospital; the study was conducted for the period of one month.
Statistics
SPSS version 20 software was used for analysis of the gathered data. Sample-test was done to analyze within-group variables for pain and disability on SPADI. External rotation and abduction range were analyzed by Wilcoxon Signed Ranks test for within-group and Mann-Whitney test for between-group variables. The Study was Significants resultant values were <0.05.
Reliability Procedure
Cronbach’s Alpha coefficient of the reliability for the measurements were found as 0.96 for the variable Abduction (pre and post), 0.99 for the variable External Rotation (pre and post treatment), 0.93 for the variable pain and for the variable Disability Index (SPADI) was 0.904.
RESULTS AND ANALYSIS
Sample of 50 patients were included in the study with mean age of 50.34 + 5.62. It was seen that out of 50 randomly selected patients 27 (54%) were male while 23 (46%) were females. Patients were divided into two groups equally i.e., 25 patient per group. Group A was treated by Maitland Technique while Group B was treated by Mulligan Technique. Pre and Post Range of motion of shoulder as well as pain and deformity were noted of the respective treatment given. It is transpired from the descriptive statistics that mean range of Maitland pre abduction and post abduction is 96.8 and 105.60 respectively, which shows an increase in range of 8.8 in Abduction. At the same time pre and post Mulligan Technique, ranges of abduction has shown an increase of 12 which was 103.80 before and 115.80 after treatments. In the same way, External rotation was also measured before and after each treatment in both groups. It was seen that external rotation before the treatment was 65.56 and afterwards 68.0 in Group A with a mean difference of 2.44 while in Group B external rotation before treatment was 64.24 and later 69.28, with significant difference of 5.04 in the range.
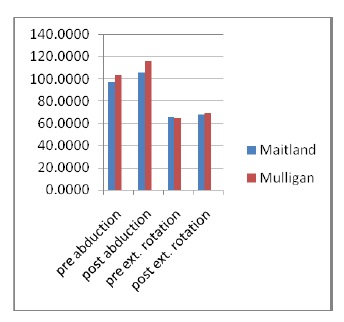
Fig 1 comparison between ROM of abduction and external rotation in both groups
Pain and disability were also calculated in patients along with comparison of total SPADI scores. It was found that in Group A, calculated pain was 7.60 and disability 7.72 before treatment and 6.36 and 6.80 after the treatment. While Group B Pretreatment pain was 7.84 and disability 7.64 but after treatment there is remarkable reduction in both pain and disability i.e., 5.96 each. The total SPADI score is 15.32 before and 13.16 after the treatment in Group A. In Group B, the total SPADI score is 15.48 before and 11.92 after the treatment.
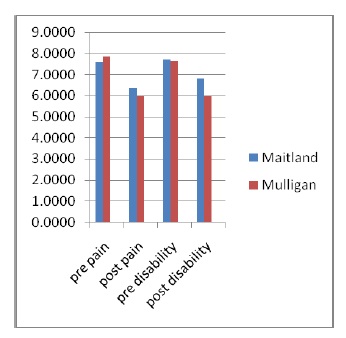
Fig 2 Comparison of SPADI score for both group
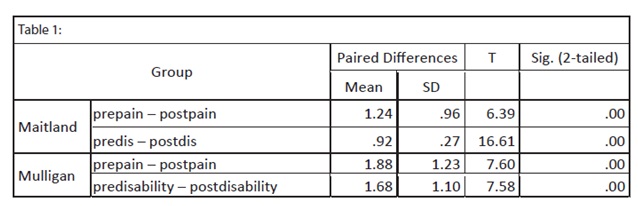
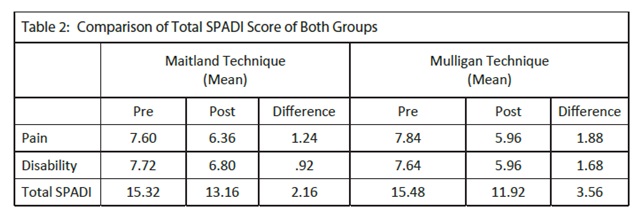
It was also transpired that both these techniques are effective in the management of frozen shoulder with p value 0.00 by applying paired sample test (Table 1). At the same time in comparison, it is evident that there is a prominent difference in the results of both techniques. It was observed that pain and disability reduction after Maitland was only of mean difference 2.16 on SPADI scoring while a difference of 3.56 in patients who underwent Mulligan Technique (Table 2).
DISCUSSION
The present study was designed to know the efficacy of Maitland mobilization techniques in the treatment of shoulder adhesive capsulitis by comparing with mulligan technique.
While analyzing the outcome measures of this study, it was observed that both the groups have shown significant improvement over time. Statistical analysis of the data in pre- and post-intervention SPADI values illustrated difference (shown by decreasing trends in Table 1 and Figure 2 for both groups). Though both groups have significantly reduced pain scores, the difference was found in favor of Group B in between-group comparison (Table 1). Both the groups shown reduction in pain scores, and this is in agreement with previous study suggesting that mobilization reduces pain23 due to neurophysiologic effects on the stimulation of peripheral mechanoreceptors and the inhibition of nociceptors. The activation of apical spinal neurons as a result of peripheral mechanoreceptor by the joint mobilization produces presynaptic inhibition of nociceptive afferent activity7.
Mechanical force during mobilization may include breaking up of adhesions, realigning collagen, or increasing fiber glide when specific movements stress the specific parts of the capsule24. Furthermore, mobilization techniques are supposed to increase or maintain joint mobility by inducing biological changes in synovial fluid, enhanced exchange.
Maitland’s rhythmic oscillations also have an effect on circulatory perfusion. The ongoing circulatory stasis may lead to ischemia and the potential for intraneural odema, inflammation, and fibrosis. Mobilization has an effect on fluid flow as blood flow in the vessels supplying the nerve fiber and synovial fluid flow surrounding the avascular articular cartilage. This, by a pressure gradient, is generated which helps in facilitating exchange of fluid, that is, increased venous drainage and dispersing the chemical irritants. This causes a reversal of the ischemia, edema, and inflammation cycle and reduces joint effusion and relieves pain by reducing the pressure over the nerve endings.
Mulligan’s technique and stretching exercise both strategies are effective in reducing pain and restoring ROM and function in patients with adhesive capsulitis in the stiffness phase. Compared with stretching exercises, Mulligan’s technique led to better improvements in terms of pain, ROM, shoulder scores. Mulligan’s technique was chosen for this study because it has the advantage of increasing ROM along with providing analgesia. Mulligan’s technique was compared with stretching because stretching exercises are the mainstay of exercises in joint limitations; however, in contrast to Mulligan’s technique they lack an analgesic effect25. Scaringe et al.26 have previously used the Mulligan’s technique in addition to chiropractic manipulations of the spine for a golfer with chronic shoulder, arm and neck pain. The authors followed the patient for 29 weeks; however, they used multiple techniques, which made it difficult to delineate the specific effects of a certain treatment.
CONCLUSION
The study revealed that the Mulligan technique is more effective to the patients as compared to the Maitland technique of the treatment of the frozen shoulder. The descriptive analysis shows that the post effects of the mulligan technique is more effective in comparison to the Maitland technique which means that the frozen shoulder should be treated by the Mulligan technique.
ACKNOWLEDGEMENTS
We are really thankful to Almighty Allah for granting me wisdom & understanding to add value through my learning process. My gratitue to Mr. Iqbal Ahmed Siddiqui for his keen interest & involvement in this study. He was always there to respond to my queries to make this activity truly different.
We are also thankful to administrative and supporting staff of Ziauddin University for relevant information and supporting me throughout the course of my research. I wish to express the deepest gratitude to my all-family members who encouraged and helped me to achieve this task. I must profound respect and regards to all of them who always make things easy and smooth for me.
REFERENCES
- Pope DP, Croft PR, Pritchard CM, Silman AJ. Prevalence of shoulder pain in the community: the influence of case definition. Ann Rheum Dis. 1997;56(5):308-12.
- Janjua UI, Ali S. Physical Therapy and Maitland’s Manual Joint Mobilization Technique, Journal ofContemporary Research.
- Leung MS, Cheing GL. Effects of deep and superficial heating in the management of frozen shoulder. J Rehabil Med 2008;40:145–150.
- Manske RC. And Prohaska D. (2008), Diagnosis and management of adhesive capsulitis. Current Review Musculoskeletal Med 2008;1:180–189
- Magee JD. Orthopedic Physical Assessment, Saunders, 4th edition (2002).
- Neviaser TJ. Intra-articular inflammatory diseases of the shoulder (1989).
- Bunker TD, Anthony PP. The pathology of frozen shoulder: a Dupuytren-like disease. J Bone Joint Surg Br. 1995;77:677–83.
- Reeves B. The natural history of frozen shoulder syndrome Scand. J. Rheumetol 1975;4:193–196.
- Kisner C. Colby LA. Therapeutic Exercises, 4th edition (2002).
- Aydogan A, Karan A, Ketenci A et al. Factors affecting therapeutic response of adhesive capsulitis in type II diabetes mellitus. J Back Musculoskeletal Rehabil. 2004;17:3–7.
- Siegel LB, Cohen NJ, Gall EP. Adhesive capsulitis: A sticky issue. Am Fam Physician. 1999;59:1843–50.
- Kibler WB. Shoulder rehabilitation: principles and practice, Medicine and Science in Sports and Exercise. 1998;30(4):40–50.
- Brotzman S, Wilk EK. Clinical Orthopedic Rehabilitation, Mosby, Philadelphia, Pa, USA, 2nd edition (2003).
- Maitland GD. Peripheral Manipulation. 4thed. Boston: Butterworth Henmann (2005).
- Vicenzino B, Wright, A. Effects of a novel manipulative physiotherapy technique on tennis elbow: a single case study. Manual Therapy. 1995; (1):30–5.
- Mulligan B. Mobilization with movement (MWM’s). Journal of Manual and Manipulative Therapy. 1993;1:154–6.
- Kumar A, Kumar S, Aggarwal A, Kumar R, Dass PG. Effectiveness of Maitland Techniques in Idiopathic Shoulder Adhesive Capsulitis, ISRN Rehabilitations. 2012; ID 710235
- Yang JL, Chang CW, Chen SY, Wang SF, Lin JJ. Mobilization techniques in subjects with frozen shoulder syndrome: randomized multiple-treatment trial. Physiotherapy. 2007;87:1307–15.
- Doner G, Guven Z, Atalay A, Celiker R. Evaluation of Mulligan’s Technique for Adhesive Capsulitis of the shoulder, Foundation of Rehabilitation Information. ISSN. 1977;1650-1977, Rehabil Med 2012.
- Kochar M, Dogra. Effectiveness of a specific physiotherapy regimen on patients with tennis elbow. Physiotherapy 2002;88:333–41.
- Rani P, Mishra N, Comparative study of the clinical outcome of Maitland and conservative treatment in the idiopathic adhesive capsulitis, Sport Medicine Journal. 2010(22).
- Teys P, Bisset L, Vicenzino B, The initial effects of a Mulligan’s mobilization with movement technique on range of movement and pressure pain threshold in pain-limited shoulders (2008).
- Simmonds FA. Shoulder pain with particular reference to the frozen shoulder, The Journal of Bone and Joint Surgery. 1949;31(3):426–32.
- Donatelli R, Wooden JM. Orthopedic Physical Therapy, Churchill Leving stone, New York, NY, USA, 2nd edition (1994).
- Gokhan D, Zeynep G, Ayçe A, and Reyhan C, (2012), Evaluation of Mulligan’s Technique for Adhesive Capsulitis of the shoulder, Faculty of Medicine, Department of Physical Medicine and Rehabilitation, İstanbul, Turkey J Rehabil Med 2012 Foundation of Rehabilitation Information. ISSN 1650-1977.
- Scaringe J, Kawaoka C, Studt T, Improved shoulder function after using spinal mobilization with arm movement in a 50 year old golfer with shoulder, arm and neck pain. Topics in Clinical Chiropractic. 2002;9:44–53.