
ABSTRACT
BACKGROUND AND AIM
The objective of my project was to determine the impact of facility characteristics on patient safety, patient experience, and service availability for procedures in hospitals.
METHODOLOGY
This study was a cross sectional survey and sampling technique used was convenient sampling. Population of 105 individuals with age 21- 50 was taken. In order to collect data, the self-developed questionnaire was used. The obtained data were analyzed by using SPSS 25.0.
RESULTS
Among 105, many participants have experience of stay in hospitals. 10% strongly agree that staff response is satisfactory to patients who reached the hospital in an emergency. Many of them were agree that Doctors are available for patients admitted to the hospital. 30% of them agree that a comfortable environment is maintained in wards for patients. Half of them were agree that counseling by the doctor to patients and caregivers for treatment procedures is satisfactory.
CONCLUSIONS
Doctors are available for patients and counselling by them is satisfactory. Lab test results are valid and timely. Pharmacy, bed facility and ambulances are easily available. Lab tests cost is not affordable. Moreover, most of the people prefer private hospitals than government hospitals due to their best services availability.
KEYWORS
Safety management, patient experience, Diagnostic equipment, medical staff, hospitals.
Muhammad Tahir Khan
Department of physical therapy, The University of Lahore, Lahore, Pakistan. ORCID ID: 0000-0002-1280-0529
Dr. Faiza Shareef
Assistant Professor Department of physical therapy, The University of Lahore, Pakistan.
ORCID ID: 0000-0002-9186-858X
Umar Farooq
Department of physical therapy, The University of Lahore, Pakistan.
ORCID ID: 0000-0001-8822-5850
Aqsa Tahir
Department of physical therapy, The University of Lahore, Pakistan.
ORCID ID: 0000-0002-0478-4581
[Khan MT, Shareef F, Farooq U, et al. Impact of Facility Characteristics on Patient Safety, Patient Experience, and Service Availability for Procedures In Hospitals
Pak.j.rehabil. 2022; 11(1):136-144]
DOI: 10.36283/pjr.zu.11.1/017
INTRODUCTION
Patient safety is preventing harm to the patients. Highlighting the building a culturally safe system of care involving health care professionals, organizations, and patients to prevent errors and learn from errors when they occur. The provision of health care is safe when there is no avoidable harm to a patient during the process and there is no risk of unnecessary harm to a patient1. The process of caring a patient contains some degree of safety risk at every point. Comprehensible policy, organizational management, safety improvements, experienced health care professionals and efficient participation, significant improvement in patient safety requires them to care for patients2.
World Patient Safety Day is celebrated on 17th September annually in order to enhance awareness of patient safety as it is the first health priority globally3. Hospitals are facing many challenges daily. Some of these challenges are Medical errors in hospitals are 3rd leading came of death in the ME after heart disease and cancer. Internationally it is supposed that medical errors kill more people than HIV, Malaria and TB4. There are many other ways to solve this worldwide problem of medical errors in the hospitals on the large scale. It can also be possible by becoming the part of healthcare ecosystem which includes Healthcare Professionals, healthcare technologists, partners, stakeholders, patients and their families5.
Patient experience is the series of interactions that patients have with the health care system including doctors, nurses and staff in hospitals6. It is the important component of health care system including several aspects of health care quality that patients value highly when they look for and treatment, such as getting well-timed organized appointments, effortless access to information, and good communication with health care providers 7,8.
Operational definition of “The degree to which nursing care satisfies patients’ expectations in terms of art of care, technical quality, physical environment, availability and continuity of treatment, and efficacy/outcomes of care,” according to the operational definition of patient satisfaction [26] and Patient safety is a health-care field that applies safety science principles to the goal of developing a reliable health-care delivery system. Patient safety is another feature of health-care systems; it reduces the occurrence and effect of adverse events while also maximizing recovery27.
Hospital services are medical and surgical services and the supporting labs, apparatus and staff that make up the medical and surgical mission of hospital system. Hospital services cover a series of medical contributions from basic health care training and research for major medical school centers 2.
In order to improve patient experience, health care providers can adjust their own behaviors and actions when responding to patients’ concerns and goals. It can be done by giving clear explanations, listening gently, and acknowledging patients with empathy. It can restore a degree of kindness to patient care allowing patients to treat them 9,10.
It was in the 80s that patient experience measures were first used, and today they are used worldwide. Nevertheless, they have been questioned as to their effectiveness11. In general, a quantitative, qualitative or mixed approach can be used to measure patient experience based on reviews in the literature12.
A patient-reported experience measure (PREM) is a questionnaire filled out by the patient regarding their experience. English NHS introduced the Friends and Family Test in 2013. One of the questions in this study asks patients whether they would recommend treatment or care they received through the NHS to friends and family who are in need of similar care13. The question is like, if you have friends or family who need similar treatment, are you likely to recommend our ward to them? Patients can answer as “extremely likely”; “likely”; “neither likely nor unlikely”; “unlikely”; “extremely unlikely”; or “don’t know”14 Patients must feel that everyone is doing all they can do for them and working well together15.
Berglas et al., 2018 conducted a study with potential consequences for patient outcomes, surgical practices have moved from hospitals and into freestanding outpatient surgery centers (ASCs) and medical offices. In response, states have introduced legislation for office-based surgeries, private organizations have set requirements for facility accreditation, and clinical guidelines have been established by professional associations. Few more work needed to be done to know which facility is not provided to patients and will work to improve them16.
Piccardi et al., 2018 conducted a study that patient safety is a primary care quality measure that should be based on individual needs and vary across different social classes. The findings of this systematic analysis indicate that vulnerable social groups in primary care are likely to encounter adverse patient safety incidents enhancing the understanding of these inequities by family doctors is a crucial first step in tackling them and improving patient safety for all patients. Using socioeconomic metrics, such as income and education, future studies should concentrate on social inequalities in patient safety17.
The objective of study was to determine the impact of facility characteristics on patient safety, patient experience, and service availability for procedures in hospitals.
METHODOLOGY
This survey was done online who visited or admitted in the hospital at any time of their life. The sample size was taken as 105. Participants were selected on the basis of inclusion criteria and simple random sampling. Population of 105 individuals with age 21- 50 was taken. In order to collect data, the self-developed questionnaire was used. The questionnaire consisted of 25 questions including demographic data.
Content analysis
This was cross sectional survey.
Target population
Reference population of this study was people in Lahore, Pakistan of age 21-50 years who may or may not visited / admitted in the hospital.
Sample size
The final sample size was taken as 105.
Sampling technique
Our sampling technique was “convenient sampling” in which we had randomly chosen the individuals.
Duration
This study was conducted in almost 4 months.
Sample selection criteria
Inclusion criteria
- Male and female both were included.
- Age 21-50 years
- Patients visiting hospitals with minor problems.
Exclusion criteria
- Patients with any serious illness are excluded.
Data collection
Data was collected from the hospital of university of Lahore, Lahore. This survey based quantitative study consisting of two parts. I informed the participants about the objective of study. Questionnaires were sent to them and given instructions thoroughly about how to fill the questionnaire. We used self- developed Questionnaire to evaluate the effects of hospital’s facility characteristics on the patient. The participants were assured that information taken from them will be confidential. Those who were not interested were excluded from the research study. The study protocol was reviewed and accepted by our instructor at University of Lahore, Lahore.
Survey for evaluation of patient’s satisfaction level
Subjects were selected by voluntary response sampling and then were evaluated by a self-reported quantitative questionnaire. A survey was conducted to evaluate patient satisfaction; the questionnaires were filled randomly by respondents of age 21 to 50 years. Our questionnaire consists of two components: A) The demographic profile section B) questions specified for evaluating the effects of hospital’s facility characteristics on the patient.
ETHICAL CONCERNS
Approved from Ethical & Research committee of my institution The University of Lahore and teaching hospital of University of Lahore. Consent was also taken from patients.
RESULTS
Among 105, many participants have experience of stay in hospitals. 10% strongly agree that staff response is satisfactory to patients who reached the hospital in an emergency. Many of them were agree that Doctors are available for patients admitted to the hospital. 30% of them agree that a comfortable environment is maintained in wards for patients. Half of them were agree that counseling by the doctor to patients and caregivers for treatment procedures is satisfactory.
TABLES
1. Distributive statistics of duration of stay at the hospital?
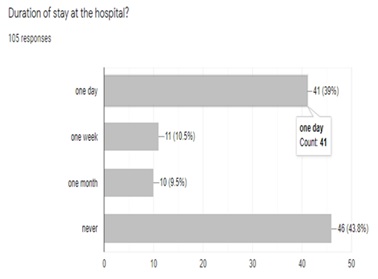
Among 105, 39% stayed at the hospital once one day, 10% stayed at the hospital one week, 10% stayed at the hospital one month and 43% never stayed at the hospital
2. Distributive statistics of staff response is satisfactory to patients who reached the hospital in an emergency?
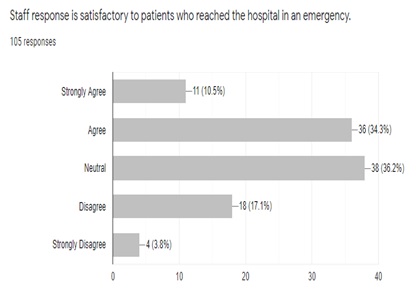
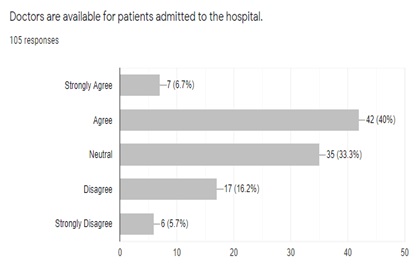
7% strongly agree, 40% agree, 33% neutral, 16% disagree and 6% strongly disagree that Doctors are available for patients admitted to the hospital.
3. Distributive statistics of Doctors are available for patients admitted to the hospital:
4. Distributive statistics of a comfortable environment is maintained in wards for patients
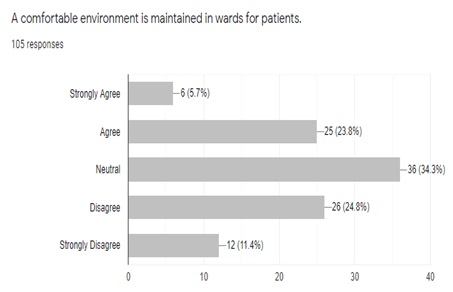
Among 105 responses, 6% strongly agree, 24% agree, 34% neutral, 25% disagree, 11% strongly disagree that a comfortable environment is maintained in wards for patients.
5. Distributive statistics of counseling by doctor to patients and caregivers for treatment procedures is satisfactory:
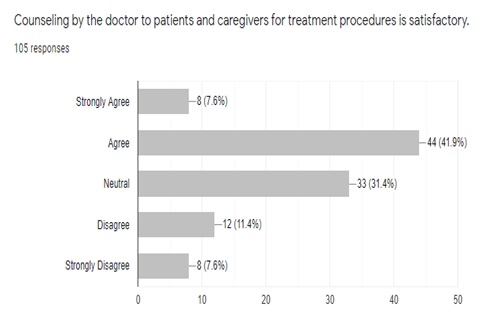
8% strongly agree, 42% agree, 31% neutral, 11% disagree, 8% strongly disagree that counseling by the doctor to patients and caregivers for treatment procedures is satisfactory.
DISCUSSION
This study was conducted in hospital of university of Lahore. My aim was to determine the procedures of facility provided to the patients and their experience in hospitals and the staff, diagnostic equipment were available for them or not and the results of my study was satisfying. The medical equipment were present for the patient’s safety. Overall environment of hospital were kept quiet and calming for the patients.
Outpatient research on procedures must focus on outcomes associated with patient-centered care, as well as concerns about safety. As previous review demonstrates, little research has been conducted regarding the role outpatient facility characteristics play in patient satisfaction or service accessibility18.
Hospital services cover a series of medical contributions from basic health care training and research for major medical school centers19. The range of services may be imperfect in specialty hospitals as cardiovascular, cancer treatment centers, or very wide to meet the requirements of the society20. Health care set-up accessibility can be a matter of life or death. It is critical for hospitals implementing electronic health records21,22.
In previous systematic reviews, they looked at the question of whether specific facilities or characteristics of outpatient facilities can impact patient safety, patient experience and access to care. Researchers found a lack of methodological clarity in the existing literature, with many studies prone to bias that limit their usefulness for determining policy and practice. Although there are methodological issues and study designs are heterogeneous, it does appear that: 1) the previous findings does not shows that procedures performed in ASCs differ from those performed in physician offices in terms of patient safety; 2) It appears that abortion providers with hospital admitting privileges or those who provide abortions in ASCs decrease service availability and 3) Conclusions cannot be drawn from research on general facility characteristics to know about how they affect patient safety23.
In this current study, I wanted to determine the effect of facility characteristics on patient safety, patient experience, and service availability for procedures in hospitals of Pakistan. The results were satisfying. Both genders were participated in this study. Population came to hospitals were from both rural and urban areas. They agreed that behavior of hospital staff was satisfactory. Hospitals now a days have all kind of equipment necessary for the treatments of patients. Nurses perform their duty efficiently in the wards and laboratory test cost is affordable to the patients in hospitals. All hospitals provide the service of pharmacies. One limitation of this study was that only the youngsters were studied. Other age groups have not been studied in this research.
Performing these types of studies can help determine whether a patient safety concern is related to a particular facility kind or characteristic, and if so, what type of intervention research which will be needed to find evidence-based solutions. Studies of patient safety in non-hospital outpatient settings are focused on other topics, such as medication errors, electronic health records, and office-based anesthesia, rather than questions relating to clinical qualification, facility design, and other procedures and characteristics24. Facilities that perform abortions outpatient and in a clinical setting, usually in a setting where the procedure is common and has a strong safety record, are an exception, and state legislatures have expected them to meet specific facility requirements 25.
CONCLUSION
The current study concluded that more women than men have visited or admitted to the hospital with majority population visits hospital once a month and had never admitted to the hospital. Most of the people are aware about the health system of the Pakistan. They admit that Doctors are available for patients and counseling by them is satisfactory. In addition, lab test results are valid and timely Pharmacy, bed facility and ambulances are easily available. However, for most of the participants, lab tests cost is not affordable. Moreover, most of the people prefer private hospitals than government hospitals due to their best services availability.
Acknowledgements
I would like to express my deep sense gratitude and appreciation towards DR. FAIZA SHAREEF and The University of Lahore for this invaluable supervision, guidance and constant encouragement throughout the study and assistance to bring this data in final shape and assisting in typing the study and analysis of the data.
Authors contributions
I would like to thank my colleagues Umar Farooq and Aqsa Tahir for helping me throughout my research work and helping me in data collection and in preparing this article.
REFERENCES
- Hefner JL, McAlearney AS, Spatafora N, Moffatt-Bruce SD. Beyond patient satisfaction: optimizing the patient experience. Structural Approaches to Address Issues in Patient Safety: Emerald Publishing Limited; 2019.
- Chang HY, Friesner D, Lee IC, Chu TL, Chen HL, Wu WE, et al. Openness to experience, work experience and patient safety. 2016;24(8):1098-108.
- De Moissac D, Bowen SJJoPE. Impact of language barriers on quality of care and patient safety for official language minority Francophones in Canada. 2019;6(1):24-32.
- de Lima Garcia C, Bezerra IMP, Ramos JLS, do Valle JETMR, Bezerra de Oliveira ML, Abreu LCdJPo. Association between culture of patient safety and burnout in pediatric hospitals. 2019;14(6):e0218756.
- Cheraghi-Sohi S, Panagioti M, Daker-White G, Giles S, Riste L, Kirk S, et al. Patient safety in marginalised groups: a narrative scoping review. 2020;19(1):1-26.
- Gomes ATdL, Ferreira MA, Salvador PTCO, Bezerril MdS, Chiavone FBT, Santos VEPJRbde. Safety of the patient in an emergency situation: perceptions of the nursing team. 2019;72:753-9.
- Jiang K, Tian L, Yan C, Li Y, Fang H, Peihang S, et al. A cross-sectional survey on patient safety culture in secondary hospitals of Northeast China. 2019;14(3):e0213055.
- Sturm H, Rieger MA, Martus P, Ueding E, Wagner A, Holderried M, et al. Do perceived working conditions and patient safety culture correlate with objective workload and patient outcomes: A cross-sectional explorative study from a German university hospital. 2019;14(1):e0209487.
- Isbell LM, Tager J, Beals K, Liu GJBq, safety. Emotionally evocative patients in the emergency department: a mixed methods investigation of providers’ reported emotions and implications for patient safety. 2020;29(10):1-2.
- org ESoRcm, imaging EFoRSieeJIi. Patient safety in medical imaging: A joint paper of the European Society of Radiology (ESR) and the European Federation of Radiographer Societies (EFRS). 2019;10:1-17.
- Wood C, Chaboyer W, Carr P. How do nurses use early warning scoring systems to detect and act on patient deterioration to ensure patient safety? A scoping review. International Journal of Nursing Studies. 2019;94:166-78.
- Huang FF, Song JH. An assessment of the reliability and factorial validity of the Chinese version of the health professional education in patient safety survey (H-PEPSS). Frontiers in psychology. 2019;10:2183.
- Waterson P, Carman E-M, Manser T, Hammer A. Hospital Survey on Patient Safety Culture (HSPSC): a systematic review of the psychometric properties of 62 international studies. BMJ open. 2019;9(9):e026896.
- Gammon J, Hunt J, Williams S, Daniel S, Rees S, Matthewson S. Infection prevention control and organisational patient safety culture within the context of isolation: study protocol. BMC health services research. 2019;19(1):296.
- Holden J, Card AJJJoPS, Management R. Patient safety professionals as the third victims of adverse events. 2019;24(4):166-75.
- Berglas NF, Battistelli MF, Nicholson WK, Sobota M, Urman RD, Roberts SC. The effect of facility characteristics on patient safety, patient experience, and service availability for procedures in non-hospital-affiliated outpatient settings: a systematic review. PloS one. 2018;13(1):e0190975.
- Piccardi C, Detollenaere J, Vanden Bussche P, Willems S. Social disparities in patient safety in primary care: a systematic review. Int J Equity Health. 2018;17(1):114.
- Browne K, Roseman D, Shaller D, Edgman-Levitan SJHa. Measuring patient experience as a strategy for improving primary care. 2010;29(5):921-5.
- Kolodzey L, Trbovich P, Kashfi A, Grantcharov TPJAos. System factors affecting intraoperative risk and resilience: applying a novel integrated approach to study surgical performance and patient safety. 2020;272(6):1164-70.
- Simsekler ME, Gurses AP, Smith BE, Ozonoff AJSS. Integration of multiple methods in identifying patient safety risks. 2019;118:530-7.
- Uttley E, Suggitt D, Baxter D, Jafar WJFG. Multiprofessional in situ simulation is an effective method of identifying latent patient safety threats on the gastroenterology ward. 2020;11(5):351-7.
- Sargent SK, Waldman RJO, America gcoN. The Patient Experience and Safety. 2019;46(2):199-214.
- Berglas NF, Battistelli MF, Nicholson WK, Sobota M, Urman RD, Roberts SCJPo. The effect of facility characteristics on patient safety, patient experience, and service availability for procedures in non-hospital-affiliated outpatient settings: a systematic review. 2018;13(1):e0190975.
- DesRoches CM, Campbell EG, Rao SR, Donelan K, Ferris TG, Jha A, et al. Electronic health records in ambulatory care—a national survey of physicians. 2008;359(1):50-60.
- White K, Carroll E, Grossman DJC. Complications from first-trimester aspiration abortion: a systematic review of the literature. 2015;92(5):422-38.
- Oberst MT. Patients’ perceptions of care: Measurement of quality and satisfaction. Cancer. 1984 May;53:2366-73.
- [27] Emanuel L, Berwick D, Conway J, Combes J, Hatlie M, Leape L, Reason J, Schyve P, Vincent C, Walton M. What exactly is patient safety?. Journal of Medical Regulation. 2009 Mar;95(1):13-24.