
OCCUPATION-BASED INTERVENTION IN STROKE REHABILITATION: PERSPECTIVES OF OCCUPATIONAL THERAPY PRACTITIONERS
ABSTRACT
BACKGROUND AND AIMS
The occupation-based intervention has shown effective recovery in overall disability of stroke survivors, yet the concept is unexplored among Pakistani occupational therapists. Therefore, this study is aimed to explore their perception regarding occupation-based intervention in stroke rehabilitation.
METHODOLOGY
A self-administered questionnaire designed in Google Docs was distributed online via email and social media applications to record participants’ responses regarding occupation-based approaches in post-stroke rehabilitation.
RESULTS
A total number of 150 occupational therapists were enrolled in the study comprised 135 females and 15 males from 18 to 44 years of age. It was revealed that 53.3% therapists had taken an average of 45 minutes of clinical practice sessions on occupation-based intervention, 64.7 % believed to be well trained in the occupation-based approach. Moreover, 69.3% stated that their professional practice in post-stroke rehabilitation is generally based on the biomedical model, yet 39.3% of therapists have no clarity of this concept.
CONCLUSION
It was concluded that most occupational therapists understand the concept of occupation-based intervention. However, only a few were trained and implementing the approach in stroke rehabilitation, while the rest were found to have insufficient knowledge regarding this practice.
KEYWORDS
Occupational Therapy, Stroke, Therapy, Rehabilitation, Activities of Daily Living, Disability
Faizan Jameel Khanzada
Lecturer Occupational Therapy Sindh Institute of Physical Medicine and Rehabilitation DUHS
Karachi, Pakistan.
[Khanzada JF. Occupation-Based Intervention in Stroke Rehabilitation: Perspectives of Occupational Therapy Practitioners. Pak.j.rehabil.
2021;10(2):60-69]
DOI: 10.36283/pjr.zu.10.2/009
This is an open-access article distributed under the terms of the Creative
Commons Attribution Licence (CC BY) 4.0 https://creativecommons.
The stroke has been considered as a prevailing Non-Communicable Disease (NCD) affecting 80% of the individuals worldwide, particularly in the lower-middle-income countries1 with a burden that is estimated to be continuously rising1-3. This burden is most likely to be associated with risk factors like Diabetes, Hypertension, and Cardiovascular Diseases that are increasing at a tremendous rate, specifically among Asian population4. Strokes differ in seriousness and later functional effect depending upon the degree of the neurological harm and expected improvement. After a stroke, numerous survivors experience some type of functional impairment that will require a time of restoration. For those with gentle impairment, recovery can be achieved through a brief time of inpatient rehabilitation or through homebased or outpatient programs 36.Long term symptoms may involve hemiparesis, balance deficiencies, mobility challenges, visual changes, sensory loss, psychological deficiencies, speech disruption, exhaustion, and sensory processing issues 35 .Any or all of those deficits might need in progress help and in some cases require institutionalized care38 .However, stroke has a significant impact on the survivors’ quality of life as it contributes to a high level of long-term adulthood disability, morbidity, mortality5. Moreover, it has also imposed an economic and social burden on families within communities5. Moreover, the survivors experienced a wide variety of cognitive-motor, visual-perceptual and psychological deficits6-7 that may dramatically cause a substantial change in their lifestyle and participation in daily living activities8. Despite of the fact, occupational therapy is well-recognized in stroke rehabilitation to provide occupation-based intervention in order to cope with the consequences of functional deficits after stroke9. According to the World Federation of Occupational Therapists (WFOT)10, the profession of occupational therapy is concerned with the promotion of health and well-being through occupation. It has classified the profession’s primary goal as enabling people to participate in activities of daily living11. Moreover, it has also demonstrated the minimum standards of education for occupational therapists regarding its role and relationship with health-related outcomes12-13.
Occupation-based intervention is an activity-based treatment in which occupational therapy practitioners use therapeutic approaches as per patient body function and health to promote well-being and prevent other dysfunction14. Moreover, these approaches are intended to facilitate neuroplasticity in stroke patients to improve impaired body function, social participation, relaxation and cognition15. Occupational therapy related treatment centers are helping individuals to take part in everyday life exercises that they find significant 34. In 1997, Law, Polatajko, Baptiste, and Townsend characterized occupation as each action individuals do to possess themselves—including exercises of everyday living (ADLs), getting a charge out of life, and social investment—that has meaning what’s more, worth to them. For the objective behind this review occupation-based interventions are described as tasks that help performance in following aspects of occupation ADLs, instrumental exercises of everyday living (IADLs), rest and rest, training, work, play, relaxation, and social cooperation 34
Occupational therapy practitioners across all settings can aid stroke individual to improve their work performance through several methods. At times, practitioners use a skills remediation, or bottom-up, approach during which particular sensory and motor loss are forward with a goal of general function return across occupations. At other times, practitioners may use an occupation-based, or top down, approach that emphasizes observing all components of a personal, determining how they relate, and developing a holistic view of the patient that’s considered altogether aspects of treatment37.The purpose of this evidence-based review was to provide occupational therapy practitioners with the current evidence supporting the use of occupation-based interventions to improve areas of occupation and social participation after stroke.Skill remediation–based interventions, although relevant part of occupational therapy treatment of stroke patients, were not considered in this evidence-based review.
Consequently, at the beginning of 20th century, occupational therapy is realized to have core competency as profession-based practices and interventions in physical and mental disability16. Besides, the profession of occupational therapy has a paradigm shift to that of the year 1940 due to its objective orientation and practical intervention in healthcare16. However, this has also led to the mechanistic paradigm period due to its increased focus on biomedical explanations for practice16. Moreover, the use of occupation to address the impact on health-related quality of life is the core of occupational therapy, and practice pattern regarding the use of occupation-based approaches was then established and distributed worldwide17. In addition to it, the use of occupation-based intervention in stroke rehabilitation is well documented. However, there is no such evidence to uncover an occupational therapist’s perspective using daily occupation-based intervention into their practice with stroke patients. Therefore, this study is aimed to explore the perspective of Pakistani occupational therapists regarding occupation-based intervention in stroke rehabilitation to find out the depth of understanding related to implementation and challenges in post-stroke rehabilitation.
METHODOLOGY
Study Setting
Data was collected from rehabilitation institutes of Karachi included Dr. Ziauddin Hospital, North and Clifton campuses, Liaquat National School of Physiotherapy and Institute of Physical Medicine & Rehabilitation.
Target Population
Occupational Therapists.
Study Design & Duration
A cross-sectional survey was conducted from September to December 2020.
Sample Size
n=150
Sample Selection
Inclusion & Exclusion Criteria
Occupational Therapists aged 25 to 45 years working in stroke rehabilitation unit having an experience of at least 1 year were included. Therapists with insufficient knowledge of stroke rehabilitation or refusal to participate were excluded.
Data Collection Procedure
A self-administered questionnaire was designed on Google Docs, distributed online via e-mails and social media platforms (Facebook, WhatsApp and Instagram). The questionnaire was comprised of 15 questions on demographics and occupation-based intervention on 5-point Likert scale of Strongly Agree, Agreed, Neutral, Disagree, and Strongly Disagree.
Prior to data collection, all participants will be given informed consent forms to ensure their voluntary participation in the study. Afterwards, responses on the questionnaire were recorded that were further analyzed for results.
Data Analysis Strategy
Data was entered and analyzed on IBM Statistics Software version 20. The demographic characteristics and responses of the participants were represented through mean, standard deviation, frequency and percentage whereas bar graphs were used for the representation of responses.
Ethical Considerations
All information of the participants was kept anonymous under the investigator’s supervision. Moreover, participants were allowed to leave any question they did not want to answer while considerable to respond biased free.
RESULTS
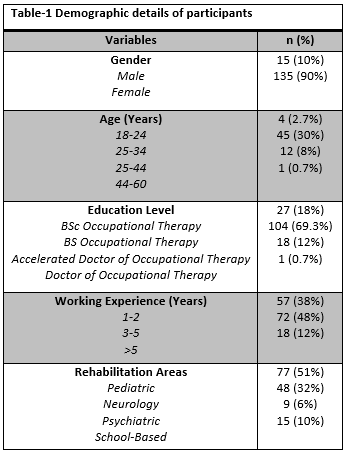
The total number of 150 occupational therapists enrolled in the study with mean age of 25.5±4.3 with maximum number of respondents attained from BS Occupational Therapy practitioners (69.3%) practicing in Pediatrics (51%) or Neurology (32%) with an experience of 3-5 years in their respective fields. The details are depicted in Table-1.
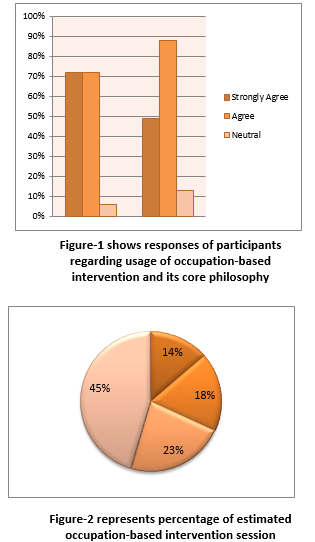
It was observed that majority of the therapists (72%) thought to use occupation-based intervention in practice of occupational therapy in post-stroke rehabilitation while (70%) reported that sufficient theories and training time are provided in their degree program while (88%) agreed that occupation-based intervention is the core philosophy of their profession with an estimated time duration of 45 minutes sessions in any setting in post-stroke rehabilitation in which (45%) agreed to practice 50% of it as illustrated in Figure-1 and 2.
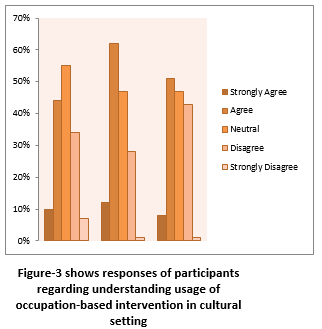
There are certain challenges that are faced by occupational therapists in implementing the occupation-based approach. Figure-3 represented that (36.7%) therapists agreed that the practice is not relevant in Pakistani cultural settings, (41.3%) agreed that occupational therapy sessions have limited time therefore therapists are reluctant to practice it moreover, (84%) therapists have clear understanding about it however (36%) respond on neutral as shown in Figure-3.
Majority of therapists (84%) agreed for CME’s on occupation-based practices as limited information is known, (64%) thinks that occupation-based intervention should be taught as a separate module at institutions/clinical settings. Moreover, (70%) agreed to enhance the usage of occupation-based approaches in post-stroke patients to improve patient’s quality of life.
DISCUSSION
The findings of this study revealed the varying perceptions and insights of Pakistani occupational therapists in implementing the occupation-based intervention in post-stroke rehabilitation. It was revealed that 53.3% occupational therapist has an average 45 minutes of clinical practice sessions on occupation-based intervention. In comparison, 91.4% understand the philosophy of occupation-based intervention as the core of the profession, while 64.7 % believed to be well trained in occupation-based approaches. Moreover, 69.3% stated that their professional practice in post-stroke rehabilitation is generally based on the biomedical model, yet 39.3% of therapists have no clarity on the concept of occupation-based intervention and its practice with post-stroke survivors and facing difficulty to achieve this goal.
According to the World Federation of Occupational Therapy, occupational therapy evaluation and intervention should mandatorily use purposeful and meaningful activities for individual and social context rather than the impairments of body structure18. Our study results also showed that most Pakistani occupational therapists’ teaching, practices, and research are based on occupation-based intervention and understanding the client needs, valuing, explanations, and finding out the difficulty patient’s face in the community19. Unfortunately, some occupational therapists reported that they often face difficult situations to implement the occupation-based intervention in post-stroke patients in the medical setting because Pakistani culture and health system do not reflect the values of occupation-centered practice20. In addition to it, certain client factors do not realize the occupational intervention concept that may affect their recovery process21 also create confusion and challenges to Pakistani occupational therapists22.
Occupation-based interventions focus on the client’s occupation, whereas they are less attractive, have low interest, and have poor patient motivation23. In Pakistan, contexts like illiteracy among patients, poverty, lack of cooperation with the therapist, the severity of illness, an increased number of patients demanding occupational therapy services shall be considered before imposing occupation-based intervention in practice. Another challenge is the limited number of occupational therapist service over 10000 head of population in Pakistan which is very low24. Moreover, most occupational therapist practices based on medical settings have restrictions, shortage of time, and substantial no-patient caseloads in their daily schedules25. In addition to challenges, Pakistani cultural values, where the family members feel obligated to help the clients in their daily occupations26. Consecutively, the health system of Pakistan with bureaucratic culture policy in hospitals leads to difficulty in occupation-based intervention usage27.
The findings of this study proposed a need to devise several strategies to overcome the challenges to implementing the occupation-based intervention in Pakistan. Therefore, patients, caregivers, and multidisciplinary rehabilitation team members should be given a piece of adequate knowledge about its use in their post-stroke rehabilitation practice28. Moreover, updating the occupational therapy educational curriculum at the national level and training related to occupation-based intervention practice in various disability conditions is crucial29-30. Furthermore, expert occupational therapists must be highlighted as reflective practitioners to diminish the challenges of OBI31-33. Stroke or Cerebrovascular Accident is caused by the reduced blood supply to the brain due to infarction or a hemorrhage, categorized as a major or minor stroke. The symptoms after post-stroke vary depending upon the size of the injury and affected vessel. Therefore this may lead to cognitive, sensory, and physical impairments presented following stroke. In Pakistan, the ideal age of stroke patients is 57-62 years; in particular, males are more commonly affected than females constituting a 60% to 40% ratio. Occupational therapists investigate, gather information, and create a collaborative environment related to patients to set goals and select occupation-based interventions34.
Occupation-based intervention is described as the task performed by stroke patients in interaction with the environment to improve overall cognitive, perceptual, motor control functions and maximize the patient’s ability to perform personal self-care and domestic tasks at home and work35. Occupation-based practice in rehabilitation is a practical approach for clients to improve the quality of life following health events or diseases. Moreover, it provides the occupational therapist with a unique, holistic, and more client-centered approach. Occupation-based practice in their cultural clinical settings may face specific logistic issues; therefore, the credibility of occupation and contextual factors are required for occupation-based practice in their clinical setting to provide in-hand rehabilitation36. A study conducted in Iran inspected and examined the Iranian occupational therapists in implementing occupation-based practice in their clinical settings showed that occupational therapists have sound knowledge in their education program about occupation-based intervention and is effective to provide meaningful intervention based on the client’s interests, needs, health and participation in daily life37. Furthermore, specific weaknesses in their current occupational therapy bachelor curriculum related to occupation-based practice need to be revised according to faculty and student’s requirements38. Occupation-based intervention effectively achieves the desired therapy outcomes that are proved in various practice settings, including hand therapy, neurological and burn injury rehabilitation. Moreover, positive patient perceptions were recorded on occupation-based treatments that intrinsically motivated them and gave a sense of ownership. Furthermore, there is a need to allocate some funds and creative work to develop and evaluate occupation-based interventions in natural contexts. It has been shown in the literature that there are numerous pieces of evidence available in developed countries in this context yet unexplored in Pakistani occupational therapists.
Despite of the fact, number of studies revealed work-related stress among occupational therapists in comparison to other healthcare professionals as they involved in multi-disciplinary rehabilitation therefore are exposed to repetitive exposure to physical effort, difficult behavior, home based services and prolonged interventions, particularly in stroke based-interventions. This might leads to the risk of encountering occupational pressure, reduces their quality of life and increase stress29-30. Moreover, it was addressed that the risk factor of physical stress and strain faced by occupational therapists contribute to stress are physical challenging role. Also in home based therapy sessions where the patient is completely depended on therapist so the physical work load increase in home therapy session which decreases the therapist quality of life32-34.
Strength
To the best of the author’s knowledge, this type of study on occupation-based practice in post-stroke disability is the first to be conducted in Pakistan, clearly representing the core philosophy’s occupational therapy profession and its authentic practice. The study also highlights the challenges occupational therapists face in their practice and needs to upgrade the intervention context concepts to promote effective health-related outcomes.
Limitations
This study has some limitations that included selected occupational therapists practicing in stroke rehabilitation according to inclusion criteria. The sample size was not achieved to the fullest due to the ongoing COVID pandemic, while limited male responses were received compared to females. Furthermore, specific questions did not attempt that may exhibit some biases in the results.
Future Directions
According to epidemiological study in Pakistan, it was identified that risk factors related to stroke are prevalent in which hypertension is most commonly evident (68.88%) whereas urban population is more prone to all risk factor except heart disease. Moreover, an overall incidence of stroke is much higher in Pakistan than any other developed country. Therefore there is a need for occupational therapy professionals, leaders, and researchers to plan large-scale studies related to occupation-based intervention practices in various disability conditions for possible prevention in Pakistan following the core ideology of the occupational therapy profession in multidisciplinary rehabilitation.
CONCLUSION
It was concluded that most occupational therapists understand the concept of occupation-based intervention, but only a few are trained and implementing the approach in stroke rehabilitation, while the remaining were found to have insufficient knowledge regarding it. Therefore, future studies should highlight the scope of occupation-based intervention in Pakistan to promote occupational therapy and better care of the disorder.
REFERENCES
- Khan MI, Khan JI, Ahmed SI, Ali S. The epidemiology of stroke in a developing country (Pakistan). Pakistan Journal of Neurological Sciences (PJNS). 2019;13(3):30-44.
- Khalid W, Rozi S, Ali TS, Azam I, Mullen MT, Illyas S, Soomro N, Kamal AK. Quality of life after stroke in Pakistan. BMC neurology. 2016 Dec;16(1):1-2.
- Schwertfeger, J.L., Thuente, L., Hung, P. and Larson, S.L., 2020. Post-discharge interventions to enhance coping skills for survivors of stroke and their caregivers: a scoping review protocol. JBI Evidence Synthesis, 18(2), pp.332-340.
- Blanton S, Clark PC, Cotsonis G, Dunbar SB. Factors associated with depressive symptoms of carepartners of stroke survivors after discharge from rehabilitation therapy. Topics in stroke rehabilitation. 2020 Nov 16; 27(8):590-600.
- Fallahpour M. Participation in everyday occupations among persons with stroke in Iran: An exploration of perceived participation, associated factors and lived experience. Inst för neurobiologi, vårdvetenskap och samhälle/Dept of Neurobiology, Care Sciences and Society; 2011 Sep 23.
- Krug G, McCormack G. Occupational therapy: evidence-based interventions for stroke. Missouri medicine. 2009 Mar 1;106(2):145-9.
- Sinclair K. International perspectives on occupation and participation. World Federation of Occupational Therapists Bulletin. 2004 Nov 1;50(1):5-8.
- Di Tommaso A, Isbel S, Scarvell J, Wicks A. Occupational therapists’ perceptions of occupation in practice: An exploratory study. Australian occupational therapy journal. 2016 Jun; 63(3):206-13.
- Carter MC. Parenting as Occupation: Occupational Therapists’ Perspectives on Working with Parents in Mental Health.2020
- Skubik-Peplaski C, Carrico C, Nichols L, Chelette K, Sawaki L. Behavioral, neurophysiological, and descriptive changes after occupation-based intervention. American journal of occupational therapy. 2012 Nov 1;66(6):e107-13.
- Lloyd K, Gee BM. Use of occupation-based practice by therapists: A national practice pattern analyzed. American Journal of Occupational Therapy. 2016 Aug 1;70(4_Supplement_1):7011505119p1-.
- Daud AZ, Judd J, Yau M, Barnett F. Issue in applying occupation-based intervention in clinical practice: a Delphi study. Procedia-Social and behavioral sciences. 2016 Jun 23;222:272-82.
- Kielhofner G, Hammel J, Finlayson M, Helfrich C, Taylor RR. Documenting outcomes of occupational therapy: The Center for Outcomes Research and Education. American Journal of Occupational Therapy. 2004 Jan 1;58(1):15-23.
- Mahani MK, Mehraban AH, Kamali M, Parvizy S. Facilitators of implementing occupation based practice among Iranian occupational therapists: A qualitative study. Medical journal of the Islamic Republic of Iran. 2015;29:307.
- Olsson L, Lundborg M. Occupational Therapy Process for Patients after Stroke in Thailand: a qualitative study.
- Asif M, Khalfe S A, Chughtai M R, Kumar M A, Khan V. The Barriers in Evidence Based Physical therapy with Stroke Patients. International Journal of Scientific & Engineering Research. 2017 march 3;8(3)966-970.
- Asif, M., 2017. The Barriers In Evidence Based Physical Therapy With Stroke Patients. [online] Ijser.org. Available at: <https://www.ijser.org/researchpaper/The-Barriers-in-Evidence-Based-Physical-therapy-with-Stroke-Patients.pdf> [Accessed 3 March 2017].
- Rowland TJ, Cooke DM, Gustafsson LA. Role of occupational therapy after stroke. Annals of Indian Academy of Neurology. 2008 Jan 1;11(5):99.
- Tomori K, Nagayama H, Ohno K, Nagatani R, Saito Y, Takahashi K, Sawada T, Higashi T. Comparison of occupation-based and impairment-based occupational therapy for subacute stroke: a randomized controlled feasibility study. Clinical rehabilitation. 2015 Aug;29(8):752-62.
- Wolf TJ, Chuh A, Floyd T, McInnis K, Williams E. Effectiveness of occupation-based interventions to improve areas of occupation and social participation after stroke: An evidence-based review. American Journal of Occupational Therapy. 2015 Jan 1;69(1):6901180060p1-1.
- Mulligan S, White BP, Arthanat S. An examination of occupation-based, client-centered, evidence-based occupational therapy practices in New Hampshire. OTJR: occupation, participation, and health. 2014 Mar;34(2):106-16.
- van Vuuren JJ, Okyere C, Aldersey H. The role of Occupational Therapy in Africa: A scoping review. South African Journal of Occupational Therapy. 2020 Dec;50(3):3-21.
- Parker DM. An exploration of client-centered practice in occupational therapy: perspectives and impact(Doctoral dissertation, University of Birmingham).2013
- Chisholm D, Dolhi CD, Schreiber J. Occupational therapy intervention resource manual: A guide for occupation-based practice. Cengage Learning; 2004.
- Colaianni D, Provident I. The benefits of and challenges to the use of occupation in hand therapy. Occupational Therapy in Health Care. 2010 Mar 1;24(2):130-46.
- Wressle E, Samuelsson K. Barriers and bridges to client-centered occupational therapy in Sweden. Scandinavian Journal of Occupational Therapy. 2004 Mar 1;11(1):12-6.
- Pierce D. How can the occupation base of occupational therapy be strengthened?. Australian Occupational Therapy Journal. 2003;50(1):1-2.
- Nilchaikovit T, Hill JM, Holland JC. The effects of culture on illness behavior and medical care: Asian and American differences. General hospital psychiatry. 1993 Jan 1;15(1):41-50.
- Coster WJ. 2008 Eleanor Clarke Slagle Lecture. Embracing ambiguity: facing the challenge of measurement. The American journal of occupational therapy: official publication of the American Occupational Therapy Association. 2008 Nov 1;62(6):743-52.
- Stack R, Barker D. Students as advocates for occupation-based practice. Occupational Therapy Now. 2011;13(3):13-5.
- Whiteford GE, Wilcock AA. Centralizing occupation in occupational therapy curricula: Imperative of the new millennium. Occupational Therapy International. 2001;8(2):81
- Ripat J, Wener P, Dobinson K, Yamamoto C. Internalizing client-centredness in occupational therapy students. Journal of Research in Interprofessional Practice and Education. 2014 Sep 24; 4(2).
- Fisher AG. Occupation-centred, occupation-based, occupation-focused: Same, same or different?. Scandinavian journal of occupational therapy. 2013 May 1;20(3):162-73.
- American Occupational Therapy Association. (2014). Occupational therapy practice framework: Domain and process(3rd ed.). American Journal of Occupational Therapy,68(Suppl. 1), S1–S48.
- Jørgensen, H. S., Nakayama, H., Raaschou, H. O., Vive-Larsen, J., Støier, M., & Olsen, T. S. (1995). Outcome and time course of recovery in stroke. Part I: Outcome. The Copenhagen Stroke Study. Archives of Physical Medicine and Rehabilitation, 76, 399–405.
- Teasell, R. W., Foley, N. C., Bhogal, S. K., Chakravertty, R.,& Bluvol, A. (2005). A rehabilitation program for patientsrecovering from severe stroke. Canadian Journal of Neurological Sciences, 32, 512–517.
- Christiansen IC, Baum CM, Bass-Haugen J. Person-environment-occupation-performance: An occupation-based framework for practice. Occupational therapy: Performance, participation, and well-being. 2005:243-59.
- Kelly-Hayes, M., Beiser, A., Kase,C.S.,Scaramucci,A.,D’Agostino, R. B., & Wolf, P. A. (2003). The influence of gender and age on disability following ischemic stroke:The Framingham Study. Journal of Stroke and Cerebrovascular Diseases, 12, 119126.http://dx.doi.org/10.1016/S1052-3057(03)00042-9.