
ABSTRACT
OBJECTIVES
To assess the effectiveness of lumbar manipulation (high velocity low amplitude) for the treatment of low back pain in comparison to back stretching exercises.
STUDY DESIGN
Randomized Control Trial (Experimental Study)
METHOD
The study was conducted on 200 patients at the Physiotherapy Department of Ziauddin Hospital among patients with history of low back pain of acute, sub-acute or chronic origin. In this study, patients were divided into two groups, group A and group B equally. Group A of 100 patients received Lumbar Manipulation (High Velocity Low Amplitude) and at the same time Group B of 100 patients were treated by back stretching exercises. A pre tested and structured questionnaire was used to collect data. Data was entered and analyzed by using SPSS.
OUTCOME MEASURES
Pain was measured on Visual Analogue Scale before and after the given treatment.
RESULTS
The study showed significant results for both the interventions in the treatment of low back pain but Lumbar Manipulation has been more effective in different types of low back pain while stretching exercises are less effective.
CONCLUSIONS
On the basis of this study, we are very confident that lumbar manipulation is more effective for the treatment of low back pain compared to back stretching exercise
Key Words
Low Back Pain, Lumbar Manipulation, Stretching Exercises, Visual Analogue Scale, High Velocity, Low Amplitude
Syed Abid Mehdi Kazmi
Manager
Department of Physiotherapy
Ziauddin Hospital
Nabiha Mujahid Faruq
Senior Physiotherapist
Department of Physiotherapist
Ziauddin Hospital
Sumaira Imran Farooqui
Principal
College of Physical Therapy
Ziauddin University
Jharna Devi
Senior Physiotherapist
Department of Physical Therapy
Ziauddin Hospital
[Kazmi SAM, Faruq NM, Farooqui SI, Devi J, Effectiveness of Lumbar Manipulation (High Velocity Low Amplitude) For the Treatment of Low Back Pain in Comparison to Back Stretching Exercises. Pak. j. rehabil. 2012;1(1):23-27]
INTRODUCTION
Low back pain (LBP) refers to pain felt in the lower back. Such pain or discomfort affects the low back as it supports most of our body’s weight. Risk factors of developing LBP include old age, family history, pregnancy, compression fractures of the spine, back surgery, congenital deformity, prolong sitting, sedentary lifestyle, smoking, poor posture and stress 1,2. LBP is usually divided into acute LBP (i.e., persisting for less than 6 weeks), sub-acute LBP (i.e. persisting for 6 to 12 weeks) and chronic LBP (i.e. persisting for more than 12 weeks)3. It has been proposed that LBP has a point prevalence of 6% to 33% and 1‐year prevalence of 22% to 65% and Lifetime prevalence ranged from 11% to 84%4-7. Hoy D et al in their article regarding epidemiology of low back pain mentioned point prevalence range from 1.0% to 58.1% with a mean prevalence of 18.1%7.
The European Guidelines for Management of LBP recommend supervised exercise therapy as a very effective first-line management for LBP8. Exercise therapy appears to be slightly effective in decreasing pain and improving function in adults with chronic LBP, particularly in healthcare populations. In sub-acute LBP there is evidence that a graded activity program improves absenteeism outcomes, though evidence for other types of exercise is unclear9,10.
Spinal manipulation is a safe intervention that is applied to patients with different types of low back pain. It can be defined as a localized or globally applied, single, quick, and forcible movement, alternately termed “high‐velocity thrust”, of small amplitude, following careful positioning of the patient11. The procedure is differentiated from mobilization in that a thrust is applied during the technique, versus lower velocity repetitive oscillations or sustained holds12. Spinal manipulation has been advocated in clinical practice guidelines for low back pain13, with evidence that exists to support the use of spinal manipulation for improvement of pain and function in patients with acute LBP4,14.
Spinal manipulative therapy is not only being used by physiotherapist but also by a number of other healthcare professions, such as chiropractors, osteopathic physicians, and medical physicians. The use by physical therapists (PT) has been challenged regarding whether manipulation falls within their scope of clinical practice15. Although initially underutilized by physical therapists, momentum and adherence to evidence‐based practice have enhanced the efforts to improve clinical reasoning for selection and delivery of such techniques16. Concurrent with the increased use in the clinic have been published contributions by physical therapists on the effectiveness of spinal manipulation, and the recognition of these publications by other healthcare professions17. Despite of all the research done so far, yet not enough successful attempts have been made to effectively and comprehensively define outcomes associated with physical therapy manipulation and describe the effectiveness of this intervention for patients with low back pain.
The objective of this research was to analyze the effectiveness of physical therapy spinal manipulations for the treatment of patients with LBP. Effectiveness was determined by analyzing studies that compared physical therapy spinal manipulations with stretching exercises.
OBJECTIVE OF THE STUDY
To find the effectiveness of Lumbar Manipulation (HVLA) for treatment of low back pain in comparison to Back Stretching Exercises.
METHODOLOGY
Study Design
It is a randomized control trial, experimental study conducted on 200 patients suffering from Low Back Pain.
Study Duration
The study has been conducted in duration of one year.
Sampling Method
A sample size of 200 patients was calculated through Epi with a point prevelance 18.1%7 at 95% confidence level and margin of error is 0.05. 200 Patients were a part of this study equally divided into two groups.
Group A: 100 patients were given Lumbar Manipulation.
Group B: 100 patients were given back stretching Exercises
Study Setting
Physiotherapy Department of Ziauddin Hospital, Karachi, Pakistan.
Data Collecting Procedure
The study is being conducted on the 200 patients including male and female, with age range of 18-65 years. All participants were suffering from Low Back Pain. The consent was sought from the subject before participating into the study, thereafter; the subjects were randomly divided into two groups, Group A and Group B, each consisting of 100 patients. Both groups received same protocol of treatment, including hot pack and Transcoetaneous Electrical Nerve Stimulation (TENS) before applying the main treatment intervention. Pain intensity was examined by a visual analogue scale (VAS) both pre-treatment and post-treatment which was recorde on a self administered questionnaire. The questionnaire was pre tested and structured for the collection of data. Data was analyzed on SPSS version 20.
Inclusion Criteria
Patients diagnosed with low back pain within age of 18 – 65 years were included in this study.
Exclusion Criteria
Patients with history of Spinal fracture, Neurologic signs and symptoms, Tumor, malignancy, bone tissue infection, Pregnancy, Post-surgical were not included in the study.
Ethical Consideration
According to ethical consideration Patient privacy, Patient hygiene factor, Patient therapist relationship and Environment of the place where we treat the patient were given due importance.
RESULTS
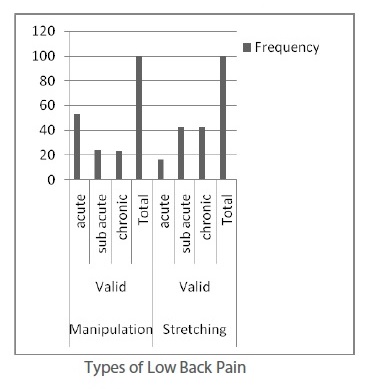
This study shows analysis of both treatment protocols given to a sample of 200 patients suffering from Low Back Pain where group A consisting of 100 patients was given lumbar manipulation while group B of 100 patients was given back stretching exercises for the pain management. Mean age of the total sample was 37.67 + 9.56 years. Out of 200 patients, 52.5% were male while 47.5% females. Out of 100 patients of Group A, who were given lumbar manipulation, 53 complained of acute low back pain while 24 were sub-acute and 23 chronic. In group B it was seen that 16 patients were of acute origin and 42 each of sub-acute and chronic low back pain.
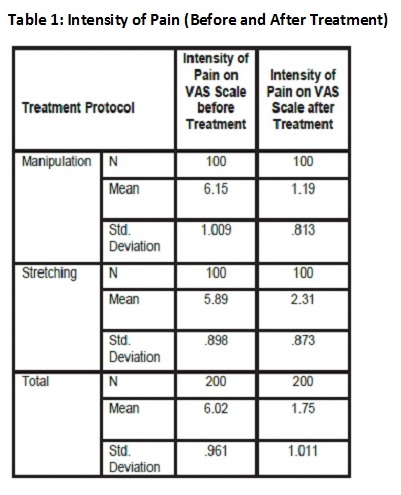
Intensity of pain was measured on VAS Scale before and after treatments. It was observed that mean intensity of pain in patients of Group A was 6.15 ± 1.009 and after the treatment it was reduced to 1.19 ± 0.813. While in Group B, intensity of pain on VAS Scale before the treatment was 5.89 ± 0.898 and after treatment it was reduced to only 2.31 ± 0.873 (Table 1) The data was analyzed to find out the effectiveness of lumbar manipulation in comparison to back stretching exercises for the management of low back pain. Paired Sample test was applied to found the effectiveness of these interventions and it was seen that both are effective (sig 0.00) for the management of low back pain. It was also observed that Lumbar manipulation has been more effective in all types of low back pain including acute, sub-acute and chronic LBP (Table 2).
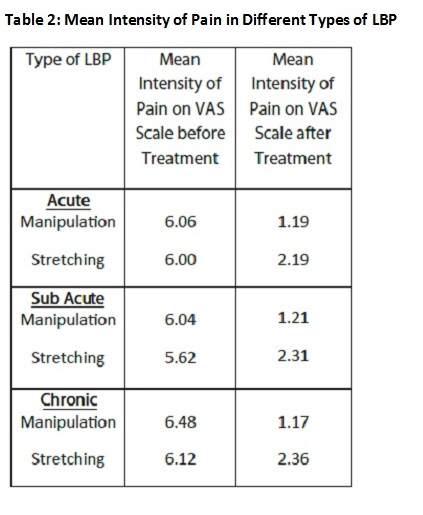
Mean intensities on VAS Scale before and after the given interventions evidently show that there is remarkable difference in pain after lumbar manipulation in all types of low back pain compared to back stretching exercises. In Acute LBP, intensity of pain 6.06 before Lumbar manipulation and was reduced to 1.19 while in Sub acute LBP, pain intensity was 6.04 earlier and 1.21 after lumbar manipulation. In chronic patients of LBP, pain intensity was 6.48 before the said treatment and 1.17 after manipulation. On the other hand, stretching exercises have shown less effectiveness on VAS scale.
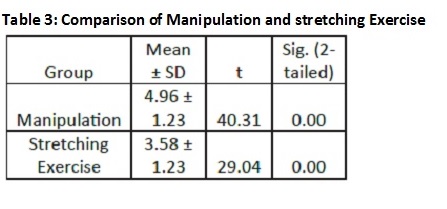
This study has found that Lumbar Manipulation (HVLA) and back stretching exercises are effective in the management of low back pain but when compared lumbar manipulation (HVLA) has shown to be more effective in management of LBP of all types on the basis of VAS Scale.
DISCUSSION
All the patients in this study were between the age group of 18-55 years with Low Back Pain without any history of spinal fracture, neurologic signs and symptoms, pregnancy or post-surgical complications.
In our study, the patient’s response to specific treatment was assessed on Visual Analogue Scale (VAS). All patients felt relief in pain after the given treatment but there was prominent reduction in pain in patients who underwent manipulation compared to stretching exercises.
According to Evans et al. manipulation is beneficial in reducing low back pain but for a shorter period18. It was evident in our data that manipulation showed better results in patients with acute low back pain.
IIn another article by Koppenhaver SL et al stated that if a patient has LBP that is fairly acute without any focal and irritable symptoms, may be the best candidates Spinal Manipulative Therapy treatment approach19. In our study we had similar patients and the Manipulative therapy has been extremely effective as a treatment option.
According to Bronfort G et al suprvised exercise was more significant for the management of chronic low back pain compared to spinal manipulation20. In the same way, in our study stretching exercise was seen to be slightly more effective in management of low back pain of chronic origin.
Other treatment options for managing low back pain include other exercise plans as well such as William Flexion Exercises or McKenzie Extension Exercises which are given to patients for home. These exercises might be effective if done for longer duration but manipulation and stretching exercises show immediate results which might be for shorter duration but are more effective in managing pain.
Manipulative Therapy is effective for the treatment of chronic nonspecific LBP. Researches also suggest that lumbar manipulation may be extremely effective to obtain long-term benefit, after the initial intensive manipulative therapy21-24.
Rubinstein S. et al suggests that High- quality evidence is present that there is no clinically relevant difference between SMT and other interventions for reducing pain and improving function in patients with chronic low-back pain25-26.
In my experience, spinal manipulation has been more effective in treating acute low back pain while stretching has shown better results in chronic low back pain.
CONCLUSION
We are 95% confident that the effectiveness of lumbar manipulation (high velocity low amplitude) for the treatment of low back pain is not equal to stretching exercises. But statistics obtained from the table 1, 2 and 3 we could suggest that the lumbar manipulation treatment is better than the stretching exercises for the management of low back pain.
REFERENCE
- Black KM, Korn H, Nordin M. Association between sitting and occupational LBP. Eur Spine J 2007;16(2):283-298.
- Ehrlich G E. Bulletin of the WHO 2003;8:671-676.
- van Tudler M, Becker A, Bekkering T, Breen A, Gil de Real M, Hutchinson A et al: Chapter 3 European guidelines for the management of acute nonspecific low back pain in primary care. European Spine J. 2006;15: s169-s191.
- Dagenais S, Gay RE, Tricco AC. NASS contemporary concepts in spine care: spinal manipulation therapy for acute low back pain. Spine J. 2010;10:918‐
- Bekkering GE, Hendriks HJM, Koes BW, Oostendorp RAB, Ostelo RWJG, Thomassen JMC, van Tulder MW: Dutch Physiotherapy Guidelines for Low Back Pain. Physiotherapy 2003;89(2):82-96.
- Hayden JA, van Tulder MW, Malmivaara A, Koes BW: Exercise therapy for treatment of non-specific low back pain. Cochrane Database Syst Rev 2005,(3)
- Hoy D, Brooks P, Blyth F, Buchbinder R. The Epidimiology of Low Back Pain. Best Pract Res Clin Rheumatol. 2010;24(6):769-81
- Pengel LH, Herbert RD, Maher CG, Refshauge KM: Acute low back pain: systematic review of its prognosis. BMJ 2003,327:323.
- Walker BF. The prevalence of low back pain: a systematic review of the literature from 1966 to 1998. J Spinal Disord. 2000;13:205‐
- Airaksinen O, Brox JI, Cedraschi C, et al. European guidelines for the management of chronic nonspecific low back pain. Eur Spine J. 2006;15 (2):S192‐
- Sizer PS, Felstehausen V, Sawyer S. Eight critical skill sets required for manual therapy competency: a Delphi study and factor analysis of physical therapy educators of manual therapy. J Allied Health 2007;36(1):30‐
- Mintken PE, Derosa C, Little T. American Academy of Orthopaedic Manual Physical Therapists. J Man Manip Ther. 2008;16:50‐
- Chou R, Huffman LH. American Pain Society. American College of Physicians Non-pharmacologic therapies for acute and chronic low back pain: a review of the evidence for an American Pain Society/American College of Physicians clinical practice guideline. Ann Intern Med 2007;147(7):492‐
- Woodhead T, Clough A. A systematic review of the evidence for manipulation in the treatment of low back pain. J Orthop Med 2005;27(3):99‐
- Huijbregts PA. Chiropractic legal challenges to the physical therapy scope of practice: anybody else taking the ethical high ground. J Man Manip Ther. 2007;15(2):69‐
- Flynn TW, Wainner RS, Fritz JM. Spinal manipulation in physical therapist professional degree education: a model for teaching and integration into clinical practice. J Orthop Sports Phys Ther. 2006;36(8):577‐
- Meeker W. Wake up: We’re in a race for scientific ownership of manipulation. FCER Advance. 2005;25(1):1-13.
- Evans DP, Burke MS, Lloyd KN, Roberts EE, Roberts GM. Lumbar Spinal Manipulation on Trial. Part 1 – clinical assesment. Rheumatol Rehabil. 1978;17:46-53.
- Koppenhaver SL, Fritz JM, Hebert JJ, Kawchuk GN, Parent EC, Gill NW, Childs JD, Teyhen DS. Association between history and physical examination factors and change in lumbar multifidus muscle thickness after spinal manipulation in patients with low back pain. J Electromyography Kinesiol 2012;22(5):724–731.
- Bronfort G, Maiers MJ, Evans RL, Schulz CA, Bracha Y, Svendsen KH, Grimm RH Jr, Owens EF Jr, Garvey TA, Transfeldt EE. Supervised exercise, spinal manipulation, and home exercise for chronic low back pain: a randomized clinical trial Spine J. 2011;11(7):585–598.
- Senna, Mohammed K, Machaly, Shereen A. Does Maintained Spinal Manipulation Therapy for Chronic Nonspecific Low Back Pain Result in Better Long-Term Outcome? J Spine; 15 August 2011;36(18):1427–1437.
- Rubinstein S, van Middelkoop M, Willem JJ., de Boer, Michiel R , van Tulder, Maurits W. Spinal Manipulative Therapy for Chronic Low-Back Pain: An Update of a Cochrane Review. Spine 2011;36(13): E825–E846.
- Bronfort G, Goldsmith CH, Nelson CF, et al. Trunk exercise combined with spinal manipulative or NSAID therapy for chronic low back pain: a randomized, observer‐blinded clinical trial. J Manipulative Physiol Ther 1996;19:570‐
- Ernst E, Canter PH. A systematic review of systematic reviews of spinal manipulation. J R Soc Med 2006;99:192‐
- Rubinstein SM, van Middelkoop M, Assendelft WJJ, et al. Spinal manipulative therapy for chronic low‐back pain. Cochrane Database of Sys Rev.2011; 2
- Boissonnault W, Bryan JM, Fox K. Joint manipulation curricula in physical therapy professional degree programs. J Orthop Sports Phys Ther 2004;34:4171‐81.