
Afaq shaikh1, Bushra Ovais2, Sheeba Shahid3, Amna Yaseen4*, Umema Tariq5
1Assistant Professor, Baqai Medical University, Karachi, Pakistan![]()
2Assistant Professor, Abu Zafar Institute of Medical Science, Karachi, Pakistan![]()
3Lecturer, Baqai Medical University, Karachi, Pakistan![]()
4*Lecturer, Baqai Medical University, Karachi, Pakistan![]()
5Student, Baqai Medical University, Karachi, Pakistan![]()
ABSTRACT
Aim of study: To identify the effectiveness of particular trunk stabilization versus a general exercise in low back pain management.
Methodology: An experimental study was conducted at the physiotherapy department of Dow University of Health Sciences, 52 participants with low backache were enrolled and assessed for pain intensity using Visual Analog Scale (VAS) and disability by using the Modified Oswestry Low Back Disability Index (MOLBDQ-I). Through equal randomization one group got their low back pain treated through trunk stabilization exercises while the other with general exercises, 3times/week* 4weeks. Data were analyzed using SPSS version 25.0 by applying non-parametric Mann-Whitney U-test.
Results: This study demonstrated that males and females are equally affected by chronic low back pain. Trunk stabilizing and general exercise regimes both significantly reduced the pain and disability in the study population but the effectiveness of trunk stabilizing exercises were significantly superior in reducing pain.
Limitations and Future Implications: Study did not include a control group that received no intervention. It would be valuable to assess the cost-effectiveness of trunk stabilization exercises compared to general exercises or other interventions.
Originality: Trunk stabilizing exercises are superior in reducing pain, disability, and restoring functional mobility than general exercises in chronic back pain.
Conclusion: Trunk stabilizing exercises are superior in reducing pain, disability, and restoring functional mobility than general exercises in chronic back pain.
Keywords: Low back pain, visual analog pain scale, spine, trunk stabilization, core stability, exercise therapy, strengthening program.
Introduction
Low back pain is non-specific, owing to defective movement synchrony of the back1. Its high prevalence has led to higher utilization of health and social welfare facilities. Impaired alignment of muscular, articular, and neural factors result in insufficient spinal stability during vertebral movement with development and recurrences which is recognized as a number one cause of global disability2.
In a large number of patients, only 15% of fewer cases are reported because of some specific etiology like compression of the nerve root, vertebral fracture, neoplasia, infection, or inflammatory disease3. Invariably, 25% of individuals suffer from low back pain (LBP) in a year 4. Roughly 40% of individuals are affected at some point during their lifetime and this rate further rises to 80% among the developed countries5, 6.
Lower back pain has a major share amongst various musculoskeletal pathologies. Increased activity of superficial trunk muscles, along with decreased activity of the lumbar multifidus muscles, are major contributing factors in these patients7. Treatment plan for these patients focus on maintaining the activity of deep muscles to prevent their atrophy and strengthen the stability of the lumbar segments of the vertebral column8. Lumbar stabilizing exercises which involve both global and local trunk muscles rehabilitate by improving the strength, power, and adaptability of the spine9.
Both, acute and chronic lower back pains respond to exercises therapy. Numerous regimes of lumbar stabilization exercises are recommended as a therapeutic tool to improve lumbar function. These exercises boost muscular function during usual daily activities for the spine10.
Stabilization exercises employ muscles like transverses abdominals, internal oblique, and lumbar multifidus and help in regaining the control and stability of the spine11.
For constant low back pain, exercise therapy is considered as a more efficient and credible way by the experts12. Less researches are conducted on pain management in male and female patients, who were not involved in any strenuous physical work and acquired this pain during their daily routine (minimal physical exertion) work. Therefore, this study has been conducted to examine the effectiveness and its level for the Trunk Stabilization Exercises and General Exercises in Chronic Lower Back.
Methodology
The randomized control trial study was done to evaluate the efficacy of trunk stabilizing exercises compared to the general exercises in relieving pain and disability in patients with non-specific chronic lower back pain with routine physical activity, without any hard work. Study setting was IPM&R, DUHS. Those who were aged between 25- 45 years of both genders, with non-specific chronic LBP and visiting Neurosurgery Department of Civil Hospital Karachi and reported pain on VAS score from 3-8 were enrolled in the study. Whereas participants with a history of neoplasm, disc prolapse, osteoporosis, fracture, pregnancy were excluded from study.
By Simple convenient sampling technique sample size was calculated for each group it was 21 (n=21). After adjoining an expected drop rate of 25%, the total number of subjects per group was 26. Therefore, for the two groups, the total number of participants was 52. Sample size estimation was done using two independent sample size formula with 95% confidence interval & 99% test power and movement control for groups A & B as 3.2 + 1.2 and 1.3 + 1.2. Respectively. The overall duration of the study was from 2018 to 2021.
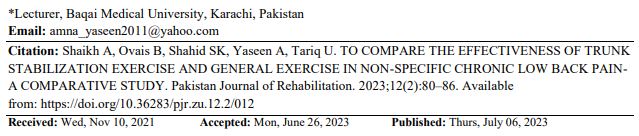
Patients were recruited after recording consent. They were required to complete the Oswestry questionnaire and VAS scale score before the commencement of the exercise module. Patients were divided into groups randomly. Group A completed the exercise module for trunk stabilization, and group B, did the general exercise module. Group A received, solitary lumber stabilizing exercise during the first two weeks. In week three these patients were exposed to light dynamic functional tasks by coordinating lumbar stabilizing muscles. Group B patients during the first two weeks received exercises involving the extension of the spine and pelvic during sitting and standing positions. During week three these patients received the same exercise with higher magnitude. During the 4th week the patient, received coordination exercises with challenges involving coordination or multiple groups of muscles. Either group carried a particular set of exercises from the commencement till the end of the study8.
Thirty minutes’ spell with three spells per week. A sum of twelve spells over the four weeks. Each exercise was repeated twenty times in ten minutes. Patients were examined for pain and disability and data was recorded using VAS and MODQS-I after four weeks by a qualified rehabilitation expert who was blind about the study groups. SPSS (statistical package for social sciences) version 23.0 was used for data analysis and variations among two groups were recorded by non-parametric test.
Results
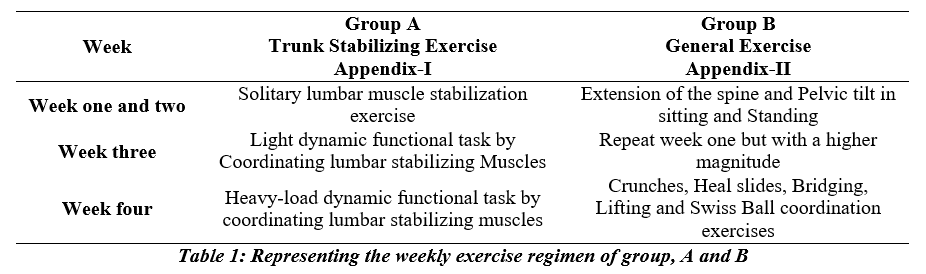
Fifty-two patients were enrolled in this study. Group A included 11 (42%) male and 15 (58%) female patients. Group B had 16 (61.5 %) male & 10 (38.5%) female participants. The average age of participants was 31± 8.45 years in group A and 32.42 ±11.21 years in group B (Table 1).
In the 25-30-year age group were 04 in group A & 05 in group B. In 31–35-year, age group was seven & nine patients in group A & B sequentially. In the 36–40-year of age group were 11 and 07 patients in group A & B respectively. In the 41-45 age group were four & five participants in group A & B. Ten (38.5%) & sixteen (61.5%) study participants from groups A & B respectively, complained to have full-time pain.
The 76.9% participants in either group reported pain aggravated in sitting position either group and few 15.4% and 7.7% mentioned this position as a relieving position. In group A, 11.5% and 7.7% in group B patients has mentioned that while standing there pain aggravated and relieved pain in 03 (11.5%) patients in each group. Whereas, 11.5% patients in group A and 7.7% patients
in group B marked, lying position as an exacerbating factor of pain and only 57.7% patients in group A and 89.2% patients in group B marked as a relieving factor. (Table 1). The mean pre-VAS score before the commencement of exercise was (7.34± 1.35) in Group A and (7.5 ± 7.6) in Group B. The analysis showed no statistical significance (P>0.05) of pre-VAS score between Group A and B (Table-2 & Figure-1).
The mean post VAS score after 04 weeks at the end of exercise sessions was (2.23± 1.56) in Group A and (4.23 ± 1.03) in Group B. The analysis showed that it was significantly (P<0.05) lower in Group A as compared to Group B (Table-2 & Figure-2). When comparing the pre and post score of VAS of Group A, it was found that the post-VAS score was significantly (p<0.05) lower than pre–VAS Score. Similar results were obtained in Group B indicating an extensive reduction in pain (Table-2) & Figures 3 & 4.
Discussion
Lower Back Pain (LBP) is a typical issue including the muscles, nerves, and bones of the back. Pain can evolve from a consistent discomfort to a rapid sharp expression. Approximately, 9 to 12% of individuals have LBP at any era of life, and almost 25% report it sooner or later during any month4. This study included patients between the ages of 25-45-year and the highest number of patients who reported low back pain was found in the age group of 36-40 years. This seems in partial agreement with the findings of Hoy, et al, who reported that the highest occurrence of LBP, is in people from 40–80 years of age and that its chance of occurrence increases as the population ages4. One explanation for this could be that low back pain initially strikes in the age group 36-40 years and afterward persists with a higher rate as the population ages. Gender preference of low back pain is still not clear or both sexes are equally affected13. A higher preference for men with a rate of 9.6% as compared to 8.7% for women has been reported.14 In contradiction to this another study has reported a higher preference for women and has suggested the presence of many physiological processes like menstruation, pregnancy, and osteoporosis, as a possible cause for this preference in females4.This study does not find any significant difference in the incidence of low back pain between the two genders. Maybe if this study could have included patients above the age of 45 years, results would have been a little different with a higher incidence in females, since sex steroidal hormones in women are pivotal in the causation and pathophysiology of many of the musculoskeletal degenerative diseases and greater disc degeneration in postmenopausal stage due to relative inadequacy of estrogen15.
In the majority of patients, LBP has no specific cause and is due to insufficient mobility control of the spine & lacks any particular pathology3. This pain is believed to be due to mechanical problems such as muscle or joint strain13,16. Pain management depends on the cause, either it is mechanical, non-mechanical, or referred pain17. For acute pain the goals are to restore normal function, return the individual to work and reduce pain. The condition is usually mild and, remits without any extensive efforts. Recovery is also helped by returning to the usual routine as soon as possible even with minimal pain18. Physical rehabilitation helps diminish pain and dysfunction in patients with chronic LBP19. It also diminishes recurrence rates for up to six months after the completion of the program and prolongs functional adequacy20,21. Some rehabilitation modules have shown significant, long-lasting, and clinically important results in every rehab. The module does not have the same practical value for every patient since rehab. Modules vary widely and the same applies to patient’s presentations22.
Our study examined and compared the impact of two different sets of exercise including a trunk stabilizing exercise (group A) and a general exercise (group B) on low back pain. The distribution of patients in two groups was more or less alike with associated demographic and characteristic factors of pain. According to the findings of this study the mean numeric pain intensity score (mean VAS score) of patients in trunk stabilization exercise group A, obtained at the end of the exercise module, was statistically highly significantly lower when compared to the mean score obtained at the beginning of the exercise module. Statistically, a similar result was also shown by patients in general exercise group B. Comparison of the post-exercise mean VAS scores of the two groups revealed that the trunk stabilization exercise has a significantly profound effect in improving the low back pain than general exercise though both the exercise modules were effective. This is consistent with the findings of Suh JH et.al, who concluded that the most significant intervention for dealing with non-specific chronic LBP and spinal instability is the rehab module which addresses lumbar stabilization23. Key factor in developing recurrent LBP is deranged stability of spinal motion segment, which normally is conferred by adaptability, adjustability, and coordination among the spinal segment and muscles around24. Modified Oswestry low back pain disability Questioner Index (MOLBQ-I) is an extremely important tool that measures a patient’s functional disability. This test is considered as a gold standard of low back functional outcome25. Comparison of the mean MOLBQ-I scores obtained at the beginning and the end of exercise modules in groups A and B showed a significant decrease in the score. This decrease indicates a reduction in the disability with an improvement in functional mobility. When the mean MOLBQ-I scores of groups A & B, obtained at the end of exercise modules were compared showed a significantly low mean score of the group A subjects. This indicates that trunk stabilization exercise is superior in restraining the disability and in improving functional mobility in low backache patients. The focus of the stabilization rehab modules are on the use of particular regional stabilizing muscles (transversus-abdominis, internal oblique, and lumbar multifidus) to regain strength, dynamism, and control of the back12. Exercise treatment is more substantial and convincing than the prevailing views of the experts and traditional physiotherapists. A similar inference has also been dictated by other researchers26.
Conclusion
This study concludes that trunk stabilizing exercises and general exercises both significantly control the pain and disability in patients with non-specific chronic low back pain but trunk stabilization exercises are far superior in reducing pain, disability, and restoring functional mobility than general exercises.
AUTHORS’ CONTRIBUTION:
The following authors have made substantial contributions to the manuscript as under:
Conception or Design: Afaq shaikh
Acquisition, Analysis or Interpretation of Data: Data: Amna Yaseen, Sheeba Shahid, Bushra Ovais,
Umema Tariq
Manuscript Approval & Writing: Amna Yaseen, Afaq Shaikh
All authors acknowledge their accountability for all facets of the research, ensuring that any concerns regarding the accuracy or integrity of the work are duly investigated and resolved.
ACKNOWLEDGEMENTS: Support from Dow University of Health Sciences was gratefully acknowledged. All the authors are very grateful to the participating individuals. Also, efforts of all the authors were highly appreciated.
INFORMED CONSENT: It has two parts: (1) Details of the study (2) Consent sheet. Subjects were recruited after obtaining a signed informed consent.
CONFLICT OF INTEREST: The authors declare no conflicts of interest.
FUNDING STATEMENTS: This work was supported by Dow University of Health Sciences.
ETHICS STATEMENTS: The protocol of the present study was registered by the local ethics committee of Dow University of Health Sciences Institutional Reviewer Board approval code IRB-407/DUHS/13.
References
- Minobes-Molina E, Nogués MR, Giralt M, Casajuana C, de Souza DLB, Jerez-Roig J, Romeu M. Effectiveness of specific stabilization exercise compared with traditional trunk exercise in women with non-specific low back pain: a pilot randomized controlled trial. PeerJ. 2020 Nov 27;8: pp e10304.
- Bansal D, Asrar MM, Ghai B, Pushpendra D. Prevalence and Impact of Low Back Pain in a Community-Based Population in Northern India. Pain Physician. 2020;23(4): pp E389.
- Maher C, Underwood M, Buchbinder R. Non-specific low back pain. The Lancet. 2017 Feb 18;389(10070): pp 736-747.
- Edwards, J., Hayden, J., Asbridge, M. et al. Prevalence of low back pain in emergency settings: a systematic review and meta-analysisBMC Musculoskelet Disord .2017;(18): pp 143. https://doi.org/10.1186/s12891-017-1511-7
- Vos, T “Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010.”. Lancet. 2012.380 (9859): pp 2163–2196.
- Malhotra V, Yao, Fun-Sun F.; Fontes, Manuel da CostaYao and Artusio’s Anesthesiology: Problem-Oriented Patient Management. Hagerstwon, MD: Lippincott Williams & Wilkins.2011. Chapter 49. ISBN 1-4511-0265-8.
- Lutz Schega, Britta Kaps, Kim-Charline Broscheid, Robert Bielitzki, Martin Behrens, Katharina Meiler, Steffen Drange, Jörg Franke, Effects of a multimodal exercise intervention on physical and cognitive functions in patients with chronic low back pain (MultiMove): study protocol for a randomized controlled trial, BMC Geriatrics. 2021;(21): 1-3.
- Akhtar MW, Karimi H, Gilani SA. Effectiveness of core stabilization exercises and routine exercise therapy in management of pain in chronic non-specific low back pain: A randomized controlled clinical trial. Pak J Med Sci. 2017 Jul;33(4): pp 1002-1006.
- Shipton EA. Physical Therapy Approaches in the Treatment of Low Back Pain. Pain Ther. 2018;7(2): pp 127-137.
- Franca FR. Burke TN, Hanada ES Segmental stabilization, and muscular strengthening in chronic low back pain- comparative study; J, Therapeutic Exercise for Spinal segmental. 2010; 65(10): pp 1013–1017.
- Richardson C. Jull G. Hodges P. Hides J. Therapeutic Exercise for Spinal Segmental Stabilization in Low Back Pain. London: Churchill Livingston. 1999; pp 992-1001.
- Low Back Pain Fact Sheet”. National Institute of Neurological Disorders and Stroke. November 3, 2015: Retrieved 5 March 2016. https://www.synovationmedicalgroup.com/wp-content/uploads/2019/10/Low-Back-Pain-Fact-Sheet-_-National-Institute-of-Neurological-Disorders-and-Stroke.pdf.
- Casazza, BA “Diagnosis and treatment of acute low back pain”. American family physician.15 February 2012;85 (4): pp 343–350. https:// sjrhem.ca/ wp-content/ uploads/ 2017/ 01/ Diagnosis-and-treatment-of-low-back-pain_AAFP.pdf.
- YìXiáng J. Wáng Jùn-QīngWáng, and ZoltánKáplár. Increased low back pain prevalence in females than in males after menopause age: evidences based on synthetic literature review: Quant Imaging Med Surg. 2016; 6(2): pp 199–206.
- Shraim BA, Shraim MA, Ibrahim AR, et al. The association between early MRI and length of disability in acute lower back pain: a systematic review and narrative synthesis. BMC Musculoskelet Disord. 2021;22(1):983.
- Hendrick P, Milosavljevic S, Hale L, “The relationship between physical activity and low back pain outcomes: a systematic review of observational studies”. European Spine Journal. 2011 Mar: 20 (3): pp 464–474
- An updated overview of clinical guidelines for the management of non-specific low back pain in primary care.”. European Spine Journal. 19 (12): pp 2075–2094.
- Van Middelkoop M, Rubinstein SM, Kuijpers T, Verhagen AP, Ostelo R, Koes BW, van Tulder MW. “A systematic review on the effectiveness of physical and rehabilitation interventions for chronic non-specific low back pain”. Eur Spine J. 2011: 20 (1): pp 19–39.
- Smith C, Grimmer-Somers K. “The treatment effect of exercise programmes for chronic low back pain”. J EvalClinPract. 2010: 16 (3): pp 484–491.
- French, SD, Cameron, M, alker, BF,Reggars, JW.Esterman, AJ. “Superficial heat or cold for low back pain.”. Cochrane Database of Systematic Reviews (1):2006.
- Lehtola V, Luomajoki H, Leinonen V, Gibbons S, Airaksinen O. Efficacy of movement control exercises versus general exercises on recurrent sub-acute nonspecific low back pain in a sub-group of patients with movement control dysfunction. Protocol of a randomized controlled trial. BMC musculoskeletal disorders. 2012 Dec;13(1):1-9.
- Suh JH, Kim H, Jung GP, Ko JY, Ryu JS. The effect of lumbar stabilization and walking exercises on chronic low back pain: A randomized controlled trial. Medicine (Baltimore). 2019;98(26): pp 16173.
- Fairbank JC, Pynsent PB.The Oswestry Disability Index. Spine 2000:15;25(22): pp 2940-2953.
- Kumar T, Kumar S, Nezamuddin M, Sharma VP. Efficacy of core muscle strengthening exercise in chronic low back pain patients. Journal of back and musculoskeletal rehabilitation. 2015 Jan 1;28(4): pp 699-707.
- Abdellatif, M.M., Kamel, M.R., Ahmed, H.H., & Diab, H.R. Effect of Lumbar Stabilization Exercises Versus Kinesio taping on Chronic Mechanical Low Back Pain. Isotope and Radiation Research. 2016;48(2): pp 243-253.
- Kwon, Sung Ho, Oh, Seung Jun, and Kim, Do Hyun. ‘The Effects of Lumbar Stabilization Exercise on Transversus Abdominis Muscle Activation Capacity and Function in Low Back Pain Patients.2020: pp 147 – 152.
The Ziauddin University is on the list of I4OA, I4OC, and JISC.
This is an open- access article distributed under the terms of the Creative Commons Attribution License (CC BY 4.0).