
Taliah Bashir Sandhu1, Ayesha Jamil2*
1Post-graduate student of Master of Philosophy in Physical Therapy, Faculty of Allied Health Science, University of Lahore, Pakistan![]()
2*Assistant Professor at University Institute of Physical Therapy, Faculty of Allied Health Science, University of Lahore, Pakistan![]()
ABSTRACT
Aims of Study: Planter fasciitis (PF) is a common cause of heel pain. Muscle energy technique (METs) and passive soft tissue therapies are widely used for its management. The objective of this review was to evaluate the comparative effectiveness of METs and passive soft tissue therapies on PF.
Methodology: An extensive electronic literature search was made using different databases and search engines. Studies regarding METs and soft tissues therapies were investigated according to the eligibility criteria, using extracted data form and assessed for risk of bias. Outcome measures were pain and functional status. Quality assessment was done with Downs and Black, Cochrane risk of bias tool, PEDro scale and Critical Appraisal Skill Program (CASP) tool.
Results: Five articles met the selection criteria, were systematically reviewed for quantitative synthesis on comparative effects of METs and passive soft tissue therapies on PF. The quality of studies was moderate to high.
Limitations and Future Implications: Less evidence on desired interventions and outcome measures was the limitation. Relative efficacy helps in clinical decision making and improves patient’s related outcomes.
Originality: This review is the independent creation of authors.
Conclusion: Manual soft tissue techniques are more effective than METs on improving pain and function in planter fasciitis.
Keywords: Ischemic compression, musculoskeletal manipulations, soft tissue therapy, myofascial release therapy, plantar fasciitis, static stretching, muscle stretching exercises.
Introduction
Heel pain is one of the most prevalent musculoskeletal diseases of the lower limb, affecting both physically active and sedentary people1. Amongst the possible causes, planter fasciitis is one of the most common causes of heel pain2. Planter Fasciitis (PF) affects people of all ages, ethnicities, and levels of activity. It seems to be common in physically active people like runners and military personnel, as well as in general population, especially among women in their 40s and 60s3.
A study reported that more than two million people in the United States are treated for PF each year, accounting for 11-15 % of all professional visits for foot pain4. A study in Pakistan presented that about 13.2 % of the security population is affected with PF, another study reported prevalence among teachers is 34.7 %5.
Planter fasciitis is a degenerative syndrome caused by the overuse or repeated injury at the level of calcaneum6. Tightness of Achilles tendon, soleus, and gastrocnemius and weakness of intrinsic foot muscles are the functional risk factors that strains the plantar fascia and limits the dorsiflexion7. As planter fascia serves to provide dynamic shock absorption and help in the longitudinal arch,8 so the risk of developing PF are increased in individual with pes planus (flat feet or low arch), pes cavus (high arches) and other anatomical risk factors are excessive femoral anteversion, excessive lateral tibial torsion, over-pronation and leg length discrepancy9.
Discomfort in the plantar region of the foot, more notably in the inferior heel and the anteromedial calcaneus typically gets worse with prolonged standing or weight-lifting activities. When the plantar aponeurosis is stiff, as in the morning or after a period of inactivity, pain is felt by stepping on the tips of the toes, forcing the foot and toes dorsiflex, and extending the knee10. It is not connected to paresthesia or nocturnal discomfort11.
The usefulness of various electrotherapy modalities, including contrast baths, cryotherapy, phonophoresis, laser, ultrasound, and microwave diathermy, has been shown in various studies12. Different physiotherapy treatment conventions help in pain relieving for example, rest, taping, stretching, night brace, silicon heel pads and myofascial release techniques13. Among therapeutic techniques, numerous active and passive interventions are applied. Muscle Energy Technique (MET) is an active manual technique, in which the patient is actively participate in producing muscular contractions, used to extend shortened structures, increase range of motion, and resolve trigger points in a variety of musculoskeletal problems including plantar fasciitis14. There are different passive manual soft tissue techniques are provided by therapist to alleviate the discomforts of PF. Chronic disorders that produce tightness and constriction in soft tissues is being treated by myofascial release (MFR) 15. By applying the MFR it low load, prolonged stretch to the myofascial complex with the goal of restoring ideal length, reducing discomfort, and enhancing function16. The Ischemic Compression Technique (ICT) is also a non-invasive passive manual approach used for decades to treat myofascial pain syndrome17. The method to release myofascial trigger point with 90-second pressure on MTrPs18. Likewise, Cyriax’s transverse friction massage is believed to normalize soft tissue fibre alignment, increase scar tissue mobility, and promote healing through controlled micro trauma19. Static stretching applied to the muscles also aids to reduce symptoms by easing the strain on the plantar fascia, and resulting gain in ankle range of motion may lessen the discomfort20.
There is an ongoing debate on the effects of different manual therapy techniques on pain and functional disability in patients with planter fasciitis. However, the comparison between effects of active and passive manual therapy techniques on patient clinical outcomes need to be address. Therefore, the purpose of this review is to compare the effects of muscle energy technique with other passive manual therapies on pain and functional status in planter fasciitis patients.
Methodology
Search Strategy and Study Selection Criteria
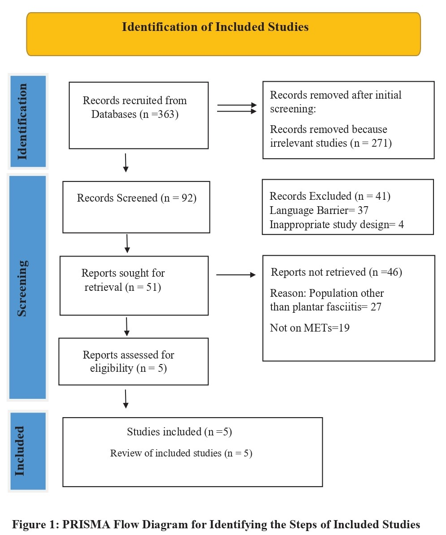
This review was done by following the guidelines of Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) 21. The protocol was registered in PROSPERO22 (ref id: CRD42022338370).
Two independent reviewers (AJ and TBS) conducted electronic search from databases including PubMed, Medline, CINAHL, PEDro, Google scholar and Cochrane database using medical subject heading and applying Boolean operators’ i.e. muscle energy techniques AND Ischemic Compression OR Myofascial Technique OR Trigger Point Release OR Cyriax Transverse Friction massage OR Static Stretching AND Planter Fasciitis. In the first round, study titles and abstracts were reviewed for identification and screening for eligibility, whereas, in second round full text of articles were studied for quality assessment and data synthesis.
The inclusion criteria were made using the PICO model. Only Randomized controlled trials (RCTs) published in English language from 2014-2022, conducted on patients with plantar fasciitis in which METs and any other passive manual soft tissue therapy, having at least one outcome variable of pain and functional status reported were included in the review. Studies which have used Visual Analogue Scale (VAS) for pain assessment, Foot and Ankle Ability Measures (FAAM) for assessing functional status were used for the systematic review23. Older studies other than RCTs in Non-English language, with non-validate outcome measures were excluded.
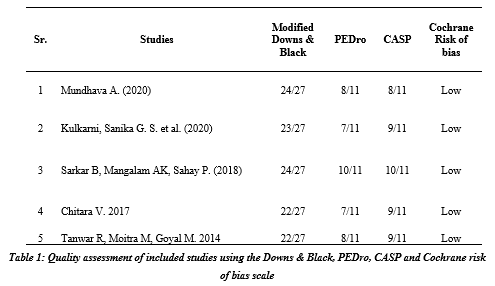
Quality assessment of RCTs was done with Modified Downs and Black checklist, Cochrane Risk of Bias Tool, PEDro scale and Critical Appraisal Skill Program (CASP). The Modified Downs and Black checklist was used for determining external validity of included studies24. The Cochrane risk of bias tool evaluates for risk of bias as low, unclear or high risk25. PEDro scale determines the methodological quality of RCTs26. Critical Appraisal Skills Programmer (CASP) was used to make a sense of randomized controlled trail (RCT) 27. The data was extracted separately using a data extraction form adapted from the Cochrane Collaboration.
Results
According to the accumulated articles, total 363 articles based on the effects of METs with other passive manual soft tissue therapies on planter fasciitis patients were identified in the search strategy in the databases. Appling the inclusion and exclusion criteria, around 92 articles were investigated and 41 articles were excluded because the study design was inappropriate. After reading the abstract 56 articles, only 46 were consider as a primary studied. When reading the full text articles only five studied are up to the inclusion criteria and they all were randomized control trails (RCTs) which were consider as the best evidence which were included in the systematic review.
The score of the randomized controlled trials on Downs and Black checklist was ranged from 22 to 24, on Pedro scale; score was ranged from 7 to 10, CASP score was from 8 to 10 and Cochrane risk of bias was low. To eliminate any potential sources of bias in randomized controlled trials, it’s critical to achieve baseline comparability between the intervention groups. Where it wasn’t obvious whether the traits of intervention groups were comparable, increasing the source of bias, all five of the investigations were able to establish baseline similarity in their groups.
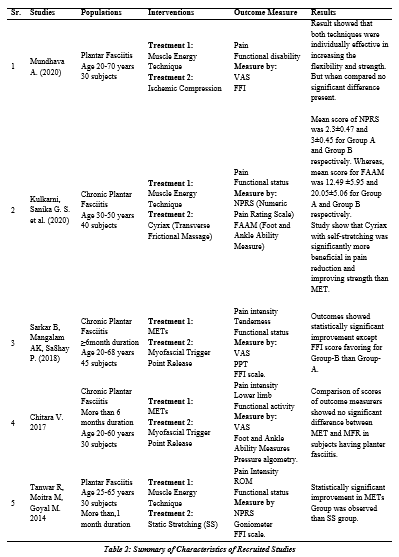
The total numbers of participants consisting in five studies 175 patients. Out of 175 patients 60 patients are suffering from unilateral planter fasciitis and 115 patients are suffering from bilateral planter fasciitis and they all are clinically diagnosed case of planter fasciitis. The females are more as compare to the males, 99 patients are females whereas 76 are males which means females suffering more with planter fasciitis then males. It presents 57% all over population, approximately two to one. The means age of participants ranged from 20 years old14, 15, 28 to 70 years old28. Participants who had no history of fracture, congenital foot deformity and pervious surgery of planter fasciitis are included. The types of techniques used in the studies: muscle energy technique14,15,19,20,28 and other passive manual therapy are ischemic compression28, static stretching20, myofascial trigger point release14, Cyriax transverse frictional massage 19 and myofascial release15.
In the included studies, only one concluded that muscle energy technique was more effective than the static stretching with p<0.0520 and two studies concluded that muscle energy technique, ischemic compression (p ˃ 0.05) and myofascial release (p ˃ 0.0001) are equally effective on planter fasciitis15, 28. Two studies including comparison of METs with that of Cyriax technique 14 and myofascial trigger point release therapy19 provided that Cyriax technique had statistically significant better effects on clinical outcomes over METs (p< 0.05), whereas myofascial trigger point release therapy produce significant reduction in pain, but not in functional status (p˃0.05).
Discussion
Patients suffering from planter fasciitis had complain of pain and difficulty in walking that affects their functional performance; impairing personal and social life. The aim of this review was to explore the comparative effects of different active and passive manual therapy techniques on planter fasciitis. A number of RCTs undergoing muscle energy technique on patients with plantar fasciitis were compare with passive interventions like ischemic compression, static stretching, trigger point release, Cyriax (transverse frictional massage) and myofascial release therapy. Using rigorous recruitment methods, five selected RCTs based on study selection’s criteria were investigated. The studies which were included in this review were of good quality range from “moderate to high” on quality assessment. Moreover, the recent studies on planter fasciitis, who meet the inclusion and exclusion criteria, based on the extensive literature search were the part of this review. All the findings, its reliability and treatment parameters like duration of intervention, frequency and intensities were observed. The results of these studies were compared on the basis of outcome variables, treatment session and follow-up period; reported that the passive manual therapies produce overall better outcomes than the muscle energy technique. Blinding greatly benefits the controlled trails and eliminate the chances of bias in the studies. Though, only in one study, double binding have been done in which patient, and assessor were blind.14 In the remaining four studies, researcher was unable to determine whether the blinding has been done or not15,19,20,27. However, all the five studies showed the same baseline similarity of Cochrane risk of biasness in the groups of intervention.
Out of five studies, one study resulted that muscle energy technique was more effective in reducing pain, increasing range of motion and improving functional activity of foot in planter fasciitis than the static stretching (p<0.05)20. The other two studies presented no significant difference between muscle energy technique, ischemic compression (p ˃ 0.05) and myofascial release (p˃ 0.0001), and all three techniques had yields equal improvement in pain, functional activity, flexibility and strength in patients with planter fasciitis15, 28. Studies on Cyriax technique and myofascial trigger point release therapy showed significant improvement in outcomes of patients with chronic PF than the METs with (p< 0.0001) and (p <0.05) respectively14,19. There are a specific guidelines or protocol for rehabilitation of planter fasciitis, the finding in this review suggested that other passive therapy combined with routine physical therapy is most efficient intervention used for rehabilitation of planter fasciitis and it should be applied from the very first session to gain maximum benefits on clinical outcomes.
This study addresses only a limited number of treatment outcomes, which is one of the limitations of this review. But to the researcher’s knowledge, a very less studies found with desired outcome variable of interest, that were published during 2014 to 2022, like only one study was found on ankle ROM20. Further research is recommended on the other outcomes like quality of life and satisfaction level towards treatment approach and effectiveness of other manual therapy techniques in patients with planer fasciitis.
Conclusion
This review provides evidence that overall passive manual soft tissue techniques are more effective in decreasing pain, improving range of motion, flexibility of muscles and functional status than the muscle energy technique in planter fasciitis patients.
AUTHORS’ CONTRIBUTION:
The following authors have made substantial contributions to the manuscript as under:
Conception or Design: Taliah Bashir Sindhu, Ayesha Jamil
Acquisition, Analysis or Interpretation of Data: N/A
Manuscript Writing & Approval: Taliah Bashir Sindhu, Ayesha Jamil
All authors acknowledge their accountability for all facets of the research, ensuring that any concerns regarding the accuracy or integrity of the work are duly investigated and resolved.
ACKNOWLEDGEMENTS: We would like to thank all the colleagues who supported us in the production of this review. Their contributions are sincerely appreciated.
INFORMED CONSENT: The informed consent was not signed because the study was a systematic review.
CONFLICT OF INTEREST: The authors have no conflict of interest.
FUNDING STATEMENTS: The authors declare that no funding has been received during this research.
ETHICS STATEMENTS: The protocol of the present study was registered in PROSPERO (ref id: CRD42022338370).
References
- Levy SE, Giarelli E, Lee LC, Schieve LA, Kirby RS, Cunniff C, Nicholas J, Reaven J, Rice CE. Autism spectrum disorder and co-occurring developmental, psychiatric, and medical conditions among children in multiple populations of the United States. Journal of Developmental & Behavioral Pediatrics. 2010 May 1;31(4): pp 267-275.
- Montes G, & Halterman J S. Association of childhood autism spectrum disorders and loss of family income. Pediatrics. 2008; 121(4): pp e821-e826.
- Furrukh J, Anjum G. Coping with autism spectrum disorder (ASD) in Pakistan: A phenomenology of mothers who have children with ASD. Cogent psychology. 2020 Dec 31;7(1): pp 1728108.
- Strunk J, Leisen M, Schubert C. Using a multidisciplinary approach with children diagnosed with autism spectrum disorder. Journal of Interprofessional Education & Practice. 2017 Sep 1;8: pp 60-68.
- Bowman KS, Suarez VD, Weiss MJ. Standards for interprofessional collaboration in the treatment of individuals with autism. Behavior Analysis in Practice. 2021 Dec;14(4): pp 1191-208.
- Rilveria JR. Understanding the secondary system of therapeutic alliance in autism interventions from the perspectives of parents and caregivers. International Journal of Child Care and Education Policy. 2022 Jan 10;16(1): pp 1-24.
- Beaudry-Bellefeuille I, Pomoni M, Welch A, Moriyon-Iglesias T, Suarez-Gonzalez M, Ramos-Polo E. Multidisciplinary approach to assessment and intervention of feeding problems in children with autism spectrum disorders: a clinical perspective. Irish Journal of Occupational Therapy. 2021 Sep 3;49(2): pp 77-83.
- Imran N, Azeem MW. Autism spectrum disorders: perspective from Pakistan. Comprehensive Guide to Autism. New York: Springer. 2014: pp 2483-96.
- Migowa A, Bernatsky S, Ngugi A, Foster HE, Muriuki P, Lusambili A, Luchters S. An iceberg I can’t handle: a qualitative inquiry on perceptions towards paediatric rheumatology among healthcare workers in Kenya. Pediatric Rheumatology. 2023 Jan 21;21(1):6.
- Santos PD, Bordini D, Scattolin M, Asevedo GR, Caetano SC, Paula CS, Perissinoto J, Tamanaha AC. The Impact of the Implementation of the Picture Exchange Communication System–PECS on Understanding Instructions in Children with Autism Spectrum Disorders. InCoDAS. 2021 May 5; 33. Sociedade Brasileira de Fonoaudiologia. https:// doi.org/ 10.1590/ 2317-1782/ 20202020041.
The Ziauddin University is on the list of I4OA, I4OC, and JISC.
This is an open- access article distributed under the terms of the Creative Commons Attribution License (CC BY 4.0).