
Sadia Sukhera1, Muzna Munir2*, Aroona Sattar3, Hira Rafique4, Zumah Saeed5, Hina Shiren6
1Senior Lecturer, Quaid e Azam College, Sahiwal, Pakistan![]()
2*Assistant Professor, Riphah International University, Lahore, Pakistan![]()
3Junior physical therapist, Riphah International University, Lahore Pakistan![]()
4Senior Lecturer, Quaid e Azam College, Sahiwal, Pakistan![]()
5Senior physiotherapist, Services Hospital, Lahore, Pakistan![]()
6Lecturer, Royal College of Physiotherapy, Rahim Yar Khan, Pakistan![]()
ABSTRACT
Aims of Study: The objective was to correlate myofascial trigger points and upper limb disability in post-mastectomy females.
Methodology: This six-month duration study included 45 participants aged 18 or older, using non-probability convenience sampling, who had undergone mastectomy at least six months prior. Numeric pain rating scale, Simon’s trigger point criteria and a disability questionnaire were used to assess disease complications.
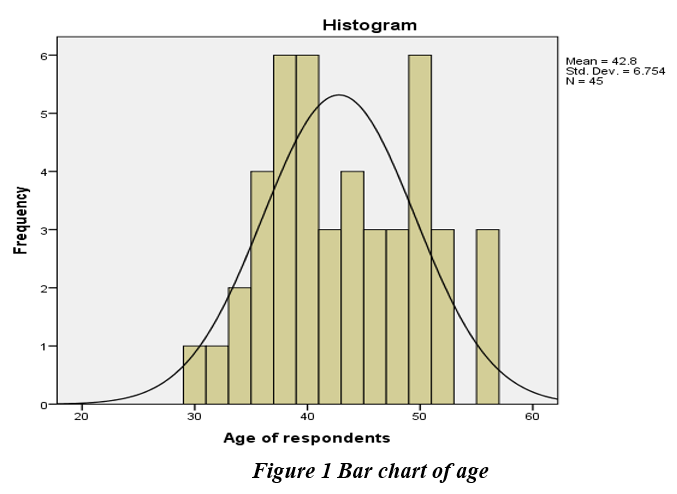
Results: A study involving 45 female participants (mean age 42.8±6.754) found that 33.3% had mild pain, 55.6% had moderate pain, and 11.1% had severe pain. Additionally, 46.7% had mild disability and 53.3% had moderate disability. There was a significant correlation between myofascial trigger points and upper extremity disability.
Limitations and Future Implication: The limitations include the small sample size used in study and limited generalization of findings due to cultural and contextual factors. Further research is needed to explore interventions and understand the long-term impact of myofascial trigger points on upper limb function.
Originality: This research is original in its focus on the correlation between myofascial trigger points and post-mastectomy upper limb disability.
Conclusion: This study concluded that there is a highly significant relation between trigger points in muscles and disability of upper extremity in female patients after mastectomy.
Keywords: Breast neoplasms, mastectomy, myofascial pain syndrome, upper extremity, myofascial trigger points, post mastectomy pain.

Introduction
Breast neoplasm is one of the main reasons for female deaths worldwide1. A rapid increase in the frequency of breast cancer was observed from 2008 to 20122. One of the surgical treatments for
I-III stages of breast cancer is mastectomy3. The term mastectomy represents an array of surgeries that include partial or complete removal of breast tissues4,5. Unfortunately, patients have to suffer a progression of postoperative complications after mastectomy such as seroma formation, wound infection, hemorrhage, arm pain, stiffness, and loss of range of motion in the cervical spine, shoulder, and arm termed upper quadrant dysfunction6.Following breast mastectomy, women tend to suffer from increased myofascial pain syndrome caused by trigger points7-9. Upper limb dysfunction is one of the most occurring post-op morbidity in mastectomy patients that can cause a reduction in the range of ipsilateral upper limb movement and functional hindrances for a long period10-12.
In 2022 a study evaluated the impact of rehabilitation for upper extremity disability in breast cancer survivors. Quick Dash scale was used to determine severity of disability. The study concluded that outpatient cancer rehabilitation program results in significant reduction of upper extremity disability after undergoing breast cancer treatments13,14.
A narrative review in 2019 was conducted to approximate the widespread presence of myofascial pain syndrome in patients of cancer to analyze the effectiveness of its treatments. Data was collected from PubMed, CINHIL, PEDRO, and Google scholar. All randomized control trial published material was analyzed. The result concluded that there was a rise in the incidence of myofascial pain syndrome in breast carcinoma patients15,16.
A study conducted in 2018 showed a greater prevalence of pain due to myofascial trigger points in upper trapezius muscle. Female having neck pain showed low pain intensity than breast cancer survivors17. An De Groef conducted a study in 2018 to highlight the myofascial trigger points contribution in upper extremity pain of breast cancer survivors18.
A quasi-experimental research design was utilized by in 2017. In the sample group, 60 patients were included. Three scales i.e.; Disabilities of Arm, Hand and Shoulder Scale (DASH), Muscle Strength Scale, and Rosenberg Self Esteem Scale were used to examine the impact of early upper limb exercises on reduction of disabilities and improvement of self-esteem among mastectomy patients. Muscle strength, self-esteem, and upper limb function were more greatly affected in the study group. The study concluded that exercises can reduce upper limb disabilities in post-mastectomy patients and can also increase their muscle strength and quality of life19,20.
A systemic review was conducted in 2015. The research aimed to observe the influence of therapeutic exercises on the physical consequences of breast cancer surgery such as painful and decrease mobility in upper limb21,22.
Up to the researcher’s knowledge, there is a lack of literature on the correlation between trigger points and upper limb disability in post-mastectomy patients as there are more studies on generalized upper limb disability without focusing on trigger points. This study aims to provide more data related to the correlation of physical consequences after mastectomy as it will be beneficial for future researches and in improving treatment approaches for patients. So, the goal of this study was to fill the gap in previous studies.
Hypothesis
Null Hypothesis
There is no association between myofascial trigger points and upper limb disability in post-mastectomy females.
Alternate Hypothesis
There is an association between myofascial trigger points and upper limb disability in post-mastectomy females.
Material & Methods
The study was a cross-sectional study and non-probability convenience sampling technique was used to collect data from DHQ Pak pattan and Jinnah Hospital Lahore. It was conducted within the time frame of 6 months after taking synopsis approval. The sample size calculated by Raosoft Software is 45 by taking a 5% margin of error and 95% of confidence interval23. The inclusion criteria consisted of 18 years of age or older women, with breast cancer diagnosed for the first time and at least six months are passed after surgery. The exclusion criteria were prophylactic mastectomy, cosmetic breast surgery, other medical conditions (e.g., arthritis, postural dysfunction, rounded shoulder), and recurrent cancer23. The Numeric Pain Rating Scale (NPRS) is one of the most frequently used tools to measure pain. The 11-point numeric with 0 representing no pain 1-3 representing mild pain, 4-6 representing moderate pain, and 7-10 representing severe pain15. Simons and Grewin’s criteria24 were used for determining trigger points which are taut palpable band within a skeletal muscle, referring pain distant in response to compression or painful limit to the full stretch range of motion25. The DASH questionnaire evaluates the impairment of the arm, shoulder, and hand due to injuries26. It consists of 30 questions that address health status of the individual during the past week. The total score ranges from 0 to 10019. Approval got from the ethical board of trustees before the initiation of the study. The study was disclosed to every one of the members and informed consent was taken from all subjects. Consent was taken from female participants. Members who met the inclusion criteria went through four components of evaluation which included DASH score, NPRS, and Simons criteria. Data were analyzed by SPSS version-26. Correlation between DASH total score and four items of Simons criteria were found by application of Chi-Square test.
Results
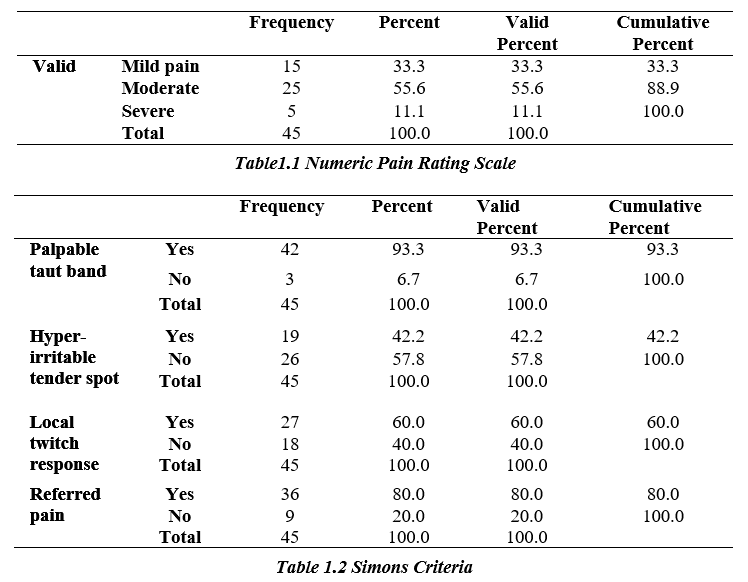
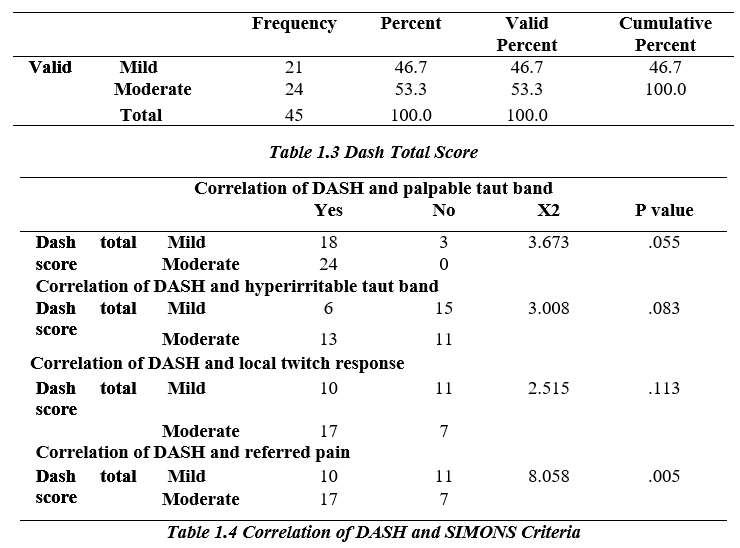
In the current study, forty-five females participated with a mean age of 42.8±6.754 years. NPRS scale resulted 33.3% of participants showing mild pain score 2, 55.6% scored 5 as moderate pain and 11.1% showed severe pain score 9. Regarding Simons criteria, only 93.3% of participants showed a taut band within skeletal muscles and 42.2% of participants responded to hyper irritable tender spot in the taut band. The frequency of participants who showed twitch response of taut band was 60 %. About 80% of participants showed compliance to Simon’s criteria of distant referred pain to trigger point compression. There were no participants who fall in the severe and no dysfunction category of DASH scale but score 50 which is mild response was showed by 46% of participants and 53.3% showed score 80 as a moderate response.
The comparison of findings of the DASH total score and the palpable taut band revealed a value of p<0.05. The analysis of correlation between DASH total score and the hyperirritable taut band was not significant as p-value>0.05. DASH score and local twitch response analysis showed a p- value not less than 0.05. Distant referred pain and DASH score analysis was significant as p-value < 0.05. The analysis for correlation of DASH score and Simons criteria was done with the Chi-square test.
Discussion
The aim was to find the relation between myofascial trigger points and disability in patients after undergoing mastectomy. The outcome measures of this study showed the existence of multiple muscle trigger points and widespread muscle pain in upper extremity after mastectomy. While analyzing the outcome measures of this study, significant correlation was found between trigger points and pain intensity in upper extremity. A study was done to find correlation number of muscle trigger points and pain intensity in post mastectomy patients. The correlation was significant showing that greater number of trigger points result in greater intensity of neck and shoulder pain. In research work, the authors investigated the widespread myofascial trigger points in post mastectomy patients27.
A study was conducted to understand the hypersensitivity of pressure pain after breast mastectomy and lumpectomy. The intensity of neck and shoulder pain was higher in women with mastectomy than with lumpectomy (P< 0.001). This study was in agreement with current study as it highlights the greater intensity of muscular pain in upper extremity after mastectomy28,29.
Another study showed the prevalence myofascial trigger points in post mastectomy patients. It was concluded that patients with mastectomy showed greater intensity of pain in the neck as well as in the shoulder region. The study was in disagreement with current study as there was lack of correlation for pain intensity and trigger points after mastectomy23.
A study presented a review of mastectomy and breast reconstruction’s effect on shoulder and upper limb function. This study was also in agreement with the current study in the context that mastectomy hurts upper limb functionality30,31.
A survey to learn about the effects of exercise in reducing disabilities among mastectomy patients. The study was in agreement in terms of upper limb function as there were statistical significance between the study and control groups post mastectomy. The DASH score result was significant P < 0.05 as in current study19,32.
The overall conclusion was deducted that many of the studies were in agreement with the current study and fewer were in disagreement.
Conclusion
The study findings concluded that mastectomy results in reducing upper limb functionality. Also, it showed the existence of multiple myofascial trigger points in patients with postmastectomy pain.
The limitation of this study was that females were reluctant to participate in the study, and the small sample size and prophylactic mastectomy were not included. The correlation in pre-mastectomy patients, a randomized experimental study in post-mastectomy patients, and psychological impact can also be considered for correlation in the future
AUTHORS’ CONTRIBUTION:
Conception or Design: Sadia Sukhera
Acquisition, Analysis or Interpretation of Data: Aroona Sattar, Hira Rafique, Zumah Saeed and Hina Shireena
Manuscript Writing & Approval: Muzna Munir
The author acknowledge his/her accountability for all facets of the research, ensuring that any concerns regarding the accuracy or integrity of the work are duly investigated and resolved.
ACKNOWLEDGEMENTS: I would like to thanks all the colleagues and participants who supported me in the production of this manuscript.
INFORMED CONSENT: Informed consent was taken from each of the patients before filling the proforma/ Questionnaire with proper code of ethics.
CONFLICT OF INTEREST: Not applied
FUNDING STATEMENTS: Not applied
ETHICS STATEMENTS: The protocol of the present study was registered by the local ethics committee of Institution (Riphah International University) approval code REC/RCR & AHS/21/0501 registered in Clinical Trial.gov (not applied as it was observational study)
References
- Kummerow KL, Du L, Penson DF, Shyr Y, Hooks MAJJs. Nationwide trends in mastectomy for early-stage breast cancer. 2015;150(1): pp 9-16.
- Ng ZX, Ong MS, Jegadeesan T, Deng S, Yap CT, editors. Breast cancer: exploring the facts and holistic needs during and beyond treatment. Healthcare; 2017: Multidisciplinary Digital Publishing Institute.
- Al–Gaithy ZK, Yaghmoor BE, Koumu MI, Alshehri KA, Saqah AA, Alshehri HZJAoM, et al. Trends of mastectomy and breast-conserving surgery and related factors in female breast cancer patients treated at King Abdulaziz University Hospital, Jeddah, Saudi Arabia, 2009–2017: A retrospective cohort study. 2019;41: pp 47-52.
- Miller KD, Siegel RL, Lin CC, Mariotto AB, Kramer JL, Rowland JH, et al. Cancer treatment and survivorship statistics, 2016. 2016;66(4): pp 271-289.
- Wang F, Peled AW, Garwood E, Fiscalini AS, Sbitany H, Foster RD, et al. Total skin-sparing mastectomy and immediate breast reconstruction: an evolution of technique and assessment of outcomes. 2014;21(10): pp 3223-3230.
- Santa Mina D, Brahmbhatt P, Lopez C, Baima J, Gillis C, Trachtenberg L, et al. The case for prehabilitation prior to breast cancer treatment. 2017;9(9): pp S305-S316.
- Petito EL, Nazário ACP, Martinelli SE, Facina G, De Gutiérrez MGRJRl-ade. Application of a domicile-based exercise program for shoulder rehabilitation after breast cancer surgery. 2012;20: pp 35-43.
- Gupta L, Singh SPJYmj. Ultrasound-Guided Trigger Point Injection for Myofascial Trigger Points in the Subscapularis and Pectoralis Muscles. 2016;57(2): pp 538-.
- Lacomba MT, Del Moral OM, Zazo JLC, Gerwin RD, Goñí ÁZJTCjop. Incidence of myofascial pain syndrome in breast cancer surgery: a prospective study. 2010;26(4): pp 320-325.
- Yang EJ, Park WB, Seo KS, Kim SW, Heo CY, Lim JYJJoso. Longitudinal change of treatment‐related upper limb dysfunction and its impact on late dysfunction in breast cancer survivors: a prospective cohort study. 2010;101(1): pp 84-91.
- Rietman JS, Dijkstra PU, Hoekstra HJ, Eisma WH, Szabo BG, Groothoff JW, et al. Late morbidity after treatment of breast cancer in relation to daily activities and quality of life: a systematic review. 2003;29(3): pp 229-238.
- Kärki A, Simonen R, Mälkiä E, Selfe JJJormojotUEBoP, Medicine R. Impairments, activity limitations and participation restrictions 6 and 12 months after breast cancer operation. 2005;37(3): pp 180-188.
- Wood KC, Hidde M, Kendig T, Pergolotti M. Community-based outpatient rehabilitation for the treatment of breast cancer-related upper extremity disability: an evaluation of practice-based evidence. Breast Cancer. 2022;29(6): pp 1099-1105.
- Brick R, Turner R, Bender C, Douglas M, Eilers R, Ferguson R, et al. Impact of non-pharmacological interventions on activity limitations and participation restrictions in older breast cancer survivors: A scoping review. J Geriatr Oncol. 2022;13(2): pp 132-142.
- Hidding JT, Beurskens CH, van der Wees PJ, van Laarhoven HW, Nijhuis-van der Sanden MWJPo. Treatment related impairments in arm and shoulder in patients with breast cancer: a systematic review. 2014;9(5): pp e96748.
- Dibai-Filho AV, de Jesus Guirro RR, Koga Ferreira VT, Kelly de Oliveira A, Maria de Almeida A, de Oliveira Guirro EC. Analysis of chronic myofascial pain in the upper trapezius muscle of breast cancer survivors and women with neck pain. J Bodyw Mov Ther. 2018;22(2): pp 237-241.
- De Groef A, Van Kampen M, Dieltjens E, De Geyter S, Vos L, De Vrieze T, et al. Identification of Myofascial Trigger Points in Breast Cancer Survivors with Upper Limb Pain: Interrater Reliability. Pain Med. 2018;19(8): pp 1650-1656.
- Mohamed WAEW, Mohammed IRJMSNJ. Effect of Early Upper Limb Exercises on Reducing its Disabilities and Improving Self-Esteem among Mastectomy Patients. 2017;1(1): pp 46-52.
- De Groef A, Van Kampen M, Dieltjens E, Christiaens M-R, Neven P, Geraerts I, et al. Effectiveness of postoperative physical therapy for upper-limb impairments after breast cancer treatment: a systematic review. 2015;96(6): pp 1140-1153.
- McNeely ML, Campbell K, Ospina M, Rowe BH, Dabbs K, Klassen TP, et al. Exercise interventions for upper‐limb dysfunction due to breast cancer treatment. 2010(6).
- Fernández-Lao C, Cantarero-Villanueva I, Fernández-de-Las-Peñas C, Del-Moral-Ávila R, Menjón-Beltrán S, Arroyo-Morales MJJob, et al. Development of active myofascial trigger points in neck and shoulder musculature is similar after lumpectomy or mastectomy surgery for breast cancer. 2012;16(2): pp 183-190.
- Shah JP, Danoff JV, Desai MJ, Parikh S, Nakamura LY, Phillips TM, et al. Biochemicals associated with pain and inflammation are elevated in sites near to and remote from active myofascial trigger points. 2008;89(1): pp 16-23.
- Simons DGJJoe, kinesiology. Review of enigmatic MTrPs as a common cause of enigmatic musculoskeletal pain and dysfunction. 2004;14(1): pp 95-107.
- Beaton DE, Katz JN, Fossel AH, Wright JG, Tarasuk V, Bombardier CJJoHT. Measuring the whole or the parts?: validity, reliability, and responsiveness of the Disabilities of the Arm, Shoulder and Hand outcome measure in different regions of the upper extremity. 2001;14(2): pp 128-142.
- Fernandez-Lao C, Cantarero-Villanueva I, Fernández-de-Las-Peñas C, Del-Moral-Avila R, Arendt-Nielsen L, Arroyo-Morales MJTCjop. Myofascial trigger points in neck and shoulder muscles and widespread pressure pain hypersensitivtiy in patients with postmastectomy pain: evidence of peripheral and central sensitization. 2010;26(9): pp 798-806.
- van Helmond N, Steegers MA, Filippini-de Moor GP, Vissers KC, Wilder-Smith OH. Hyperalgesia and Persistent Pain after Breast Cancer Surgery: A Prospective Randomized Controlled Trial with Perioperative COX-2 Inhibition. PLoS One. 2016 Dec 9; 11(12): pp e0166601.
- Fernández-Lao C, Cantarero-Villanueva I, Fernández-de-las-Peñas C, Del-Moral-Ávila R, Menjón-Beltrán S, Arroyo-Morales MJPm. Widespread mechanical pain hypersensitivity as a sign of central sensitization after breast cancer surgery: comparison between mastectomy and lumpectomy. 2011;12(1): pp 72-78.
- Vidt ME, Potochny J, Dodge D, Green M, Sturgeon K, Kass R, et al. The influence of mastectomy and reconstruction on residual upper limb function in breast cancer survivors. 2020;182: pp 531-541.
- Fourie WJJob, therapies m. Considering wider myofascial involvement as a possible contributor to upper extremity dysfunction following treatment for primary breast cancer. 2008;12(4): pp 349-355.
- Giray E, Akyüz GJEJoBH. Assessment of family caregiver burden and its relationships between quality of life, arm disability, grip strength, and lymphedema symptoms in women with postmastectomy lymphedema: a prospective cross-sectional study. 2019;15(2): pp 111.
The Ziauddin University is on the list of I4OA, I4OC, and JISC.
This is an open- access article distributed under the terms of the Creative Commons Attribution License (CC BY 4.0).