
Fizza Memon1*, Shujaat Hussain Memon2
1*Assistant Professor Hyderabad Institute of Medical and Allied Health Science, Hyderabad, Pakistan![]()
2Assistant Professor/Vice principal, Isra University, Hyderabad, Pakistan![]()
ABSTRACT
Aims of Study: The purpose of this study is to ascertain the impact of positional release technique and muscular energy technique on low back pain.
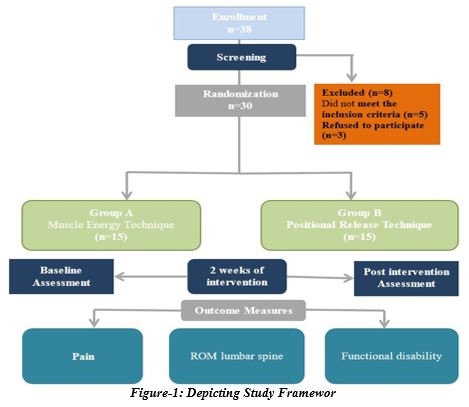
Methodology: It was a single blinded randomized controlled trial. Participants were enrolled using envelop method of simple random sampling technique. A total n=30 clinically diagnosed LBP patients with between 26 to 40 y/o were recruited and randomly divided into two groups. Group-A MET (n=15) patients receiving muscle energy technique and Group-B PRT (n=15) patients receiving Positional Release Technique for two weeks.
Results: Between groups analysis was performed using independent t test as the data was normally distributed. The results revealed statically significant results in both the groups. However, group A show more significant results with mean value of 2.0±0.53, 10.73±1.79, and 2.80±0.14 for NPRS, ODI, and Modified Schober’s Test Score respectively as shown in table 3.
Limitations and Future Implications: The study may have had a limited number of participants, which could affect the generalizability of the results. Secondly, the study might have focused on short-term outcomes, assessing the immediate effects of the interventions.
Originality: The study has used and compared new technique and have identified the efficacy between the two physical therapy intervention based study.
Conclusions: According to the findings of this study, both therapy options are successful in treating low back pain. The effectiveness of the patients in the muscle energy technique group, however, showed a substantial difference.
Keywords: Exercise, muscle energy technique, manual therapy, low back pain, physical therapy modalities, positional release technique.

Introduction
According to the Global Burden of Disease, low back pain (LBP) is defined as pain in the area from the lower border of the 12th ribs to the lower gluteal folds, with or without pain referred to one or both lower limbs that lasts for at least one day1. It is a major public health issue, with approximately 577.0 million people worldwide, or 7.5% of the total population, projected to experience LBP at any given time in 20172. Moreover, studies have shown that LBP has a lifetime prevalence of 70-80% by the age of 20, and the new onset rates are around 20% over a 1-2 year period3. Despite this, 85-95% of patients who visit primary care doctors do not have a clear-cut patho-anatomical cause for their pain.
Although most patients do not have a specific diagnosis, there are some underlying causes of LBP that need to be ruled out. For instance, estimates suggest that 0.01% of people who visit their primary care physician for LBP have infections, 0.0-0.7% have malignancies, 5% have inflammatory spondyloarthropathies, and 0-7.4% have osteoporotic vertebral fractures4. LBP-related disability has increased worldwide since 1990, and the prevalence of disability caused by LBP has grown across all age categories, with the 50-54 age group having the highest prevalence. Moreover, adults aged 20 to 65 who were employed lost over 70% of their years due to disabilities caused by LBP4. The prevalence of LBP is expected to rise as the global population ages, with the 50-54 age group currently having the highest prevalence, even though LBP frequency increases with age until 80-89 years5.
While population growth and ageing are the primary contributors to the rise in the burden of LBP, there could be other factors at play. The overall cost of low back pain in European countries accounts for 0.1-2% of their GDP6-7 However, there is a lack of information regarding the cost of LBP in lower-middle income countries. The cost of low productivity is also significant, with chronic low back pain being prevalent among more than 52%8-10 of employees in LMICs. Since the cause of LBP is unknown in most cases, it is classified as non-specific11. The National Institute for Health and Care Excellence guidelines recommend a shift towards self-management, education, and activity-based treatments, rather than surgical and pharmacological approaches12-14. Therefore, it is crucial to develop a program that addresses this condition and reduces the global burden of disease. This study aims to evaluate the effectiveness of positional release technique and muscular energy technique in alleviating pain, improving range of motion, and reducing disability among LBP patients.
Methodology
Study Design
Single blinded randomized controlled trial.
Sampling Technique
In this study, 30 patients were included and assigned to either Group A or Group B using the simple random sampling method with the envelope technique. Each group consisted of 15 patients. Before the intervention, all patients underwent a pre-assessment for the three outcome measures.
Study Setting
Data was collected from Al-shifa physical therapy clinic, Hyderabad.
Inclusion Criteria
- Low back pain (LBP)
- Age 26 to 40 y/o
- Occupational/ work-related
- Job experience >5 years
- Computer usage >4 hours/ day
Exclusion Criteria
- Radiating LBP
- History of spinal surgery
- Systemic diseases
- History of trauma
- Scoliosis
- Spinal stenosis
- Discal lesions
Data Collection Procedure
In total n=30 patients with clinically diagnosed LBP divided in categories. In group A (MET); 15 patients receiving muscle energy technique (erector spinae and quadratus lumborum) and Group-B (PRT) 15 patients receiving Positional Release Technique. All participants were blinded regarding treatment.
Patients were provided with informed consent and an orientation was organized in which they were brief about the treatment sessions. After their signed consent, both groups received a therapeutic regime of 12 treatment sessions for 2 weeks followed by a follow-up of 1 session after 15 days. Each session of MET was applied on quadratus lumborum and erector spinae consists of each muscle contraction (post-isometric relaxation and reciprocal inhibition) hold for total duration of 20 seconds and then there is period of relaxation for 10 seconds. This was repeated 9 times. It counts for 270 seconds in total. Each technique positional release of ease is held for total duration of 90 seconds on quadratus lumborum and erector spinae 3 times. It counts for 270 seconds in total. Pain, ROM lumbar spine, Functional disability were assessed via Numeric pain rating scale (NPRS), Modified Schober’s test and Oswestry Disability Index (Fig 1).
In the Modified Schober’s
Therapist position
Standing beside patient.
Patient’s position
Standing and then bent down when instructed.
Procedure
This technique involves marking marks 5 cm below and 10 cm above the level of S2, which is recorded in between the posterior superior iliac spines (PSISs). This method is used to measure lumbar range of motion (ROM). The patient will be asked to bend down to the maximum extent possible. The spacing between three places is recorded before and after the forward flexion of the limbs. The difference between the two measures will provide an estimate of the amount of flexion experienced15.
The identical technique is repeated, but this time participant is advised to bend backwards to the greatest extent possible. The amount of extension will be determined by the difference in measurements.
Procedure of Muscle energy technique for erector spinae
Position of the patient
The patient is seated on a couch and has his/her hands behind her neck. Legs of the patient were hanged down. In order to promote side bending and rotation, the practitioner retains a knee on the table next to the patient.
Therapist position
Clinician’s stands beside the individual where its side bending and rotation are to be achieved with one knee supported on couch.
Technique
To perform the technique, the therapist places their hand on the front of the patient’s axilla on the side where the rotation is indicated, then moves their hand across the patient’s neck and rests it on the opposite shoulder.
Practitioner passively performs flexion, side bending and rotation. Practitioner other hand assess the tighten part and verify that various forces localize at point of maximum tension. When the individual has been brought to a comfortable range of flexion and is holding his or her breath, for 7-10 seconds and ask to upright position, little degree against the therapist’s ardent opposition. The patient is then requested to exhale and look in the direction of the side bending. introduced. This mechanism is post isometric relaxation. The patient relaxes and the therapist take him towards new resisting barrier.
At the end of each repetition cycle, the patient is asked to inhale for 7-10 seconds and gently strive to rotate against resistance, towards to the barrier. This results in the antagonists contracting. After relaxing, a further barrier is encountered16.
Frequency of treatment
The procedure is carried out for holding contraction for 20 seconds and then 10 seconds relaxation with 9 repetitions total. It counts for 270 seconds.
Positional release technique for erector spinae
Patient position
Prone lying with ankle bolstered towards the side of tenderness.
Clinician position
Clinician positions itself next to the thorax on the side opposite to be treated.
Technique
Prone lying position hip is extended and adducted. The position is held for one minute and thirty seconds before being gradually returned to neutral. The position is held gently and slowly until the level of discomfort reduces. Place your proximal hand, elbow, and forearm diagonally across your back and toward the unaffected hip to palpate. With your near forearm, support the rib cage that is not affected. In order for your shoulder to touch the patient’s shoulder, cross your opposite hand and arm over the opposite shoulder and into the patient’s axilla. Your anterior torso may touch the patient’s posterior torso depending on how the tables are set up, your size, and the patient’s size. Put the palm of your other hand on the patient’s posterior rib cage.
While holding the non-affected side with your forearm, use your far arm to extend and rotate the involved side’s thorax and shoulder girdle. Once the extension and rotation positions have been identified use the far arm and hand to elevate and depress the shoulder girdle of the affected side17.
Frequency of treatment
Each position of ease is held for 1 minute and 30 seconds with continuous 3 repetitions
Procedure of Muscle Energy Technique for Quadratus Lumborum
Patient’s position
Supine lying with crossed feet.
Therapist position
Clinician must stand non-treated quadratus lumborum side while holding shoulder to grasp axilla whereas other hand on tip of anterior superior iliac spine (ASIS).
Procedure
The subject is commanded to slightly side bend towards the treated side for 7 seconds. This initiate’s slight isometric contractions on QL. Following a period of 7 seconds, the patient is instructed to relax completely and then side bend towards the untreated side, while the practitioner shifts his weight from the leg closer to the head to the one closer to the feet and tilts his body slightly backwards. This will effectively stretch QL18.
Frequency
The contraction will hold for 15-20 seconds allowing the extensibility of contracted muscle with 3 repetitions.
Procedure of Positional Release Technique for Quadratus Lumborum
Patient position
Lying with prone knee bend
Therapist position
Clinician stands beside the patient on side to be treated.
Procedure
While palpating the quadratus lumborum tender point, apply lateral trunk flexion and move hip joint into abduction, extension and external rotation. Slide both legs across the table toward the QL lesion with your far hand while examining the patient and applying lateral trunk flexion to the affected side. With your far hand, extend, abduct, and externally rotate the stretched limb. Use a bolster or rest the patient’s thigh on your thigh and brace it against your body to stabilize the leg into the ideal treatment posture. Once you’ve established the ideal treatment position, adjust it by applying pressure with your opposite hand or body to the limb that is closest to the lesion 19.
Frequency
Hold this position of ease till 1 minute and 30 seconds unless tenderness is reduced. Follow this procedure 3 times consecutively.
Data analysis was done using SPSS, Version- 21. Percentages and frequency were used to report the gender and number of patients in each group. Whereas, mean ± SD was used to report age, experience, duration of pain and time duration of the computer used by the patients. Pre-post scores of NPRS, modified schober’s test scores and ODI were analyzed using Paired sample t- score. Independent sample t-test was used for further comparison between both groups post treatment as the data was normally distributed.
Results
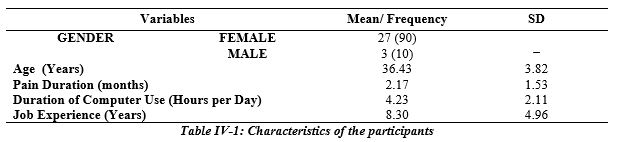
Thirty patients were recruited in the study, out of which 90% were female and remaining 10% were male, with mean age of 36.43 ± 3.82 years, whereas mean job experience of the patients was 8.30±4.9 years. Participant’s mean time of the computer usage on the daily basis was 4.23± 2.11 and mean duration of experiencing the back pain was 2.17 ± 1.53 months (table 1).
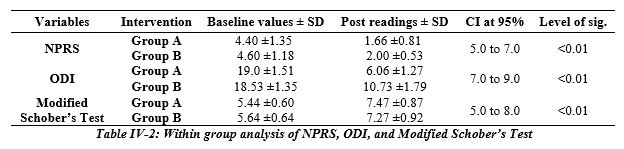
Within group analysis was done using dependent t test for all the variables because of normal distribution of data. As shown in Table 2 both groups showed statistically significant results on NPRS. However, the mean score of NPRS in patients receiving Positional Release technique on the numeric pain rating scale decreased to 2 ± 0.53 from 4.6 ± 1.18 after two weeks of intervention in contrast to Muscle Energy Technique Where the pre mean value was 4.4 ± 1.35 that reduced to 1.67 ± 0.81 with p value <0.01.
Between groups analysis was performed using independent t test as the data was normally distributed. The results revealed statically significant results in both the groups. However, group A show more significant results with mean value of 1.66±0.81, and 6.06±1.27for NPRS, and ODI respectively (table 3).

Discussion
The purpose of this research was to see how muscle energy method and position release on the quadratus lumborum and erector spinae affected pain, lumbar range, and impairment in people with low back pain. The results of our study revealed that both interventions were effective in both the groups with post mean value of 2.0±0.53, 10.73±1.79, and 2.80±0.14 for NPRS, ODI, and Modified Schober’s Test Score in Group B and 1.66±0.81, 6.06±1.27, and 3.46±0.13 for group A respectively. The results were in consistent with the finding of Priyanka rashi et al20 that Muscle energy technique has more beneficial effects in relieving pain.
There “was critical difference in the force of pain within the groups and between the groups after 4th week of treatment. Decline in pain intensity as documented with improvement in lumbar ROM was huge in the PRT group. As “found from the MODQ scale, relief from discomfort was accomplished with both Group A and Group B, in this study was considerably more critical in the PRT group. Here, MET helps in increase in blood supply, thus it decreases stiffness and restores the ROM”. It help in increasing mobility and strengthens the back muscles. While, hot moist packs help in reducing erector spinae spasm as it is helpful in increasing vascular permeability, vasodilation and reducing “inflammation. Thus, it leads to decease in pain and increasing mobility of back. PRT, used in this study had result in pain reduction. Pain reduction might have been due to the incongruent decline in the intrafusal and extrafusal fibers and reproduction of the undue proprioceptive activity21. Kaorr has given a conceptual model, how various manipulative methodologies such as isometric and stretching might be effective in the somatic dysfunction treatment22.
MET and PRT are likely useful in the relief of inflammation and spasm of the erecter spine muscle23-25 because they have activities that are akin to soft-tissue interventions, such as stretching the soft tissue in the affected spot and pushing fluids out of the inflamed area. Numerous studies have shown how effective MET and PRT are for treating low back pain. However, no study has compared the two methods using the MODQ scale for daily living tasks. There was no discernible difference between the two groups at the conclusion of the 4-week treatment period; however, there were statistically significant improvements in both active and passive lumbar extension range of motion.
MET are a successful method of treating both acute and chronic lower back pain. Chronic lateral epicondylitis and chronic neck discomfort can both be effectively treated with MET. When a functional restriction is present, MET can be used to extend the range of motion in a joint. Compared to MET, other methods appear to be better suitable for trigger sites26-27.
The greater effectiveness of the MET group may be due to its ability to directly target the erector spinae and quadratus lumborum muscles, which are commonly involved in LBP. The use of PRT, which involves the release of muscle tension through gentle positioning, may have also contributed to the improvements observed in the PRT group.
Overall, the study provides evidence to support the use of manual therapy techniques for the treatment of LBP. However, further research is needed to determine the optimal combination of manual therapy techniques for treating LBP, as well as their long-term effectiveness in reducing disability and improving quality of life for individuals with LBP. The findings of the study are consistent with previous research that has highlighted the effectiveness of manual therapy techniques in treating LBP. PRT and MET are two widely used manual therapy techniques that have been shown to reduce pain, improve range of motion, and increase muscle strength.
A Cochrane systematic review on 12 randomized controlled studies with 14 comparisons and 500 individuals across all comparisons was performed in 2016. With the exception of one, the studies included were typically tiny (with sample sizes ranging from 20 to 72), and the majority were deemed to be at high risk of bias. All trials reported on short-term results. To enable merging, the studies were split into seven functionally comparable analyses based on the patient group (acute or chronic LBP) and the type of control intervention. The addition of MET to other therapies did not result in better pain and disability results in the near term, according to low-quality data from meta-analyses and GRADE evaluation28.
Conclusion
This study aimed to investigate the impact of Positional Release Technique and Muscle Energy Technique on individuals experiencing low back pain. The results of the study indicate that both therapy options are effective in addressing low back pain. Notably, the muscle energy technique demonstrated significantly greater effectiveness than the positional release technique.
AUTHORS’ CONTRIBUTION:
Conception or Design: Fizza Memon, Shujaat Hussain Memon
Acquisition, Analysis or Interpretation of Data: Fizza Memon, Shujaat Hussain Memon
Manuscript Writing & Approval: Fizza Memon, Shujaat Hussain Memon
The author acknowledge his/her accountability for all facets of the research, ensuring that any concerns regarding the accuracy or integrity of the work are duly investigated and resolved.
ACKNOWLEDGEMENTS: I would like to thanks all the colleagues and participants.
INFORMED CONSENT: The informed consent was not applied
CONFLICT OF INTEREST: The authors have no conflict of interest.
FUNDING STATEMENTS: No funding has been received during this research.
ETHICS STATEMENTS: The guidelines provided by Belmont Report under Helsinki Declaration was exclusively followed. Informed consent were taken prior to recruitment and autonomy was given to left the study at any time without assigning any reason. The protocol was approved from Institutional approval board of Al-Shifa Hospital, IRB number ASC-PT-0122/11/2021.
References
- Hoy D, March L, Brooks P, Blyth F, Woolf A, Bain C, Williams G, Smith E, Vos T, Barendregt J, Murray C, Burstein R, Buchbinder R. The global burden of low back pain: estimates from the Global Burden of Disease 2010 study. Ann Rheum Dis 2014 ;73: pp 968–974.
- Wu A, March L, Zheng X, Huang J, Wang X, Zhao J, Blyth FM, Smith E, Buchbinder R, Hoy D. Global low back pain prevalence and years lived with disability from 1990 to 2017: estimates from the Global Burden of Disease Study 2017. Ann Trans Med 2020; 8(6): pp 299-313.
- Jones GT, MacFarlane GJ. Epidemiology of low back pain in children and adolescents. Archives of disease in childhood. 2005 Mar 1;90(3): pp 312-316.
- Finucane LM, Downie A, Mercer C, Greenhalgh SM, Boissonnault WG, Pool-Goudzwaard AL, Beneciuk JM, Leech RL, Selfe J. International framework for red flags for potential serious spinal pathologies. J Orth Sports Phys Ther 2020; 50(7): pp 350-372.
- Low back pain and sciatica in over 16s: assessment and management. NICE. Updated December 11, 2020. Published November 30, 2016. https:// www.guidelines.co.uk/ pain/ nice-low-back-pain-and-sciatica- guideline /453336.article
- Olafsson G, Emma Jonsson E. Fritzell P, Hägg O, Borgström F. Cost of low back pain: results from a national register study in Sweden. European Spine Journal. 2018 Nov; 27: pp 2875–2881.
- Wenig CM, Schmidt CO, Kohlmann T, Schweikert B. Costs of back pain in Germany. European Journal of Pain 13. 2009: pp 280–286.
- Carregaro RL, Tottoli CR, Rodrigues DD, Bosmans JE, da Silva EN, van Tulder M. Low back pain should be considered a health and research priority in Brazil: Lost productivity and healthcare costs between 2012 to 2016. PloS one. 2020 Apr 1; 15(4):e0230902. https://doi.org/10.1371/journal. pone.023090.
- Jackson T, Thomas S, Stabile V, Shotwell M, Han X, McQueen K. A systematic review and meta-analysis of the global burden of chronic pain without clear etiology in low- and middle-income countries: trends in heterogeneous data and a proposal for new assessment methods. Anesthesia & Analgesia 2016 Sep; 123(3): pp 739-748
- Mullerpatan R, Nahar S, Singh Y, Cote P, Nordin M. Burden of spine pain among rural and tribal populations in Raigad District of Maharashtra State of India. European Spine Journal. 2020 Sep 10; 30: pp 1004-1010. doi: 10.1007/s00586-020-06585-3.
- Maher C, Underwood M, Buchbinder R. Non-specific low back pain. The Lancet. 2017 Feb 18; 389(10070): pp 736-747.
- Sullivan N, Hebron C, Vuoskoski P. “Selling” chronic pain: physiotherapists’ lived experiences of communicating the diagnosis of chronic nonspecific lower back pain to their patients. Physiotherapy Theory and Practice. 2021 Sep 2; 37(9): pp 973-992.
- Foster NE, Anema JR, Cherkin D, Chou R, Cohen SP, Gross DP, Ferreira PH, Fritz JM, Koes BW, Peul W, Turner JA. Prevention and treatment of low back pain: evidence, challenges, and promising directions. The Lancet. 2018 Jun 9; 391(10137): pp 2368-2383.
- Gültekin H, Bayram D, Yüksel GA, Bayram T, Tireli H. Assessment of Modified-modified Schober Test and Lomber Range of Motion in Patients with Parkinson’s Disease with and Without Low Back Pain. Turkish Journal of Neurology/Turk Noroloji Dergisi. 2022 Mar 1; 28(1).
- Ahmed UA, Nadasan T, Van Oosterwijck J, Maharaj SS. The effect of muscles energy technique in the management of chronic mechanical low back pain: A scoping review. Journal of Back and Musculoskeletal Rehabilitation. 2021 Jan 1; 34(2): pp 179-193.
- Aiyegbusi AI, Tella BA, Uzor CU. Comparative Efficacy of Muscle Energy Technique and Positional Release Therapy in the Management of Acute and Sub-cute Low Back Pain. University of Lagos Journal of Basic Medical Sciences. 2022 Sep 2; 4(8).
- TUBASSAM S, RIAZ S, KHAN RR, GHAFOOR S, RASHID S, ZAHRA A. Effectiveness of Muscle Energy Technique Versus Strain Counter Strain Technique on Trigger Points of Quadratus Lumborum among Low Back Pain Patients. Age (Years). ; 34(4.59): pp 34-55.
- Boćkowski R, Gębska M. Assessment of Trigger Points therapy effectiveness with positional release method among office workers. Journal of Education, Health and Sport. 2019 Mar 7; 9(3): pp 97-108.
- Yadav H. Goyal M. Efficacy of muscle energy technique and deep neck flexors training in mechanical neck pain — a randomized clinical trial. Int J Ther Rehabil Res2015; 4 (1): pp 52–66.
- Thomas E, Cavallaro AR, Mani D, Bianco A, Palma A. The efficacy of muscle energy techniques in symptomatic and asymptomatic subjects: a systematic review. Chiropractic & manual therapies. 2019 Dec; 27(1): pp 1-8.
- Kashyap R, Iqbal A, Alghadir AH. Controlled intervention to compare the efficacies of manual pressure release and the muscle energy technique for treating mechanical neck pain due to upper trapezius trigger points. Journal of pain research. 2018; 11: pp 3151.
- Dayanır IO, Birinci T, Kaya Mutlu E, Akcetin MA, Akdemir AO. Comparison of three manual therapy techniques as trigger point therapy for chronic nonspecific low back pain: a randomized controlled pilot trial. The Journal of Alternative and Complementary Medicine. 2020 Apr 1; 26(4): pp 291-299.
- Oh S, Kim M, Lee M, Kim T, Lee D, Yoon B. Effect of myofascial trigger point therapy with an inflatable ball in elderlies with chronic non-specific low back pain. Journal of Back and Musculoskeletal Rehabilitation. 2018 Jan 1; 31(1): pp 119-126.
- Bellido-Fernández L, Jiménez-Rejano JJ, Chillón-Martínez R, Gómez-Benítez MA, De-La-Casa-Almeida M, Rebollo-Salas M. Effectiveness of massage therapy and abdominal hypopressive gymnastics in nonspecific chronic low back pain: a randomized controlled pilot study. Evidence-Based Complementary and Alternative Medicine. 2018 Jan 1; 2018.
- Shamsi M, Mirzaei M, Shahsavari S, Safari A, Saeb M. Modeling the effect of static stretching and strengthening exercise in lengthened position on balance in low back pain subject with shortened hamstring: a randomized controlled clinical trial. BMC musculoskeletal disorders. 2020 Dec; 21(1): pp 1-9.
- Thomas E, Cavallaro AR, Mani D, Bianco A, Palma A. The efficacy of muscle energy techniques in symptomatic and asymptomatic subjects: a systematic review. Chiropractic & manual therapies. 2019 Dec; 27(1): pp 1-8.
- Franke H, Fryer G, Ostelo RW, Kamper SJ. Muscle energy technique for non-specific low-back pain. A Cochrane systematic review. International Journal of Osteopathic Medicine. 2016 Jun 1; 20: pp 41-52.
The Ziauddin University is on the list of I4OA, I4OC, and JISC.
This is an open- access article distributed under the terms of the Creative Commons Attribution License (CC BY 4.0).