
Tasneem Shahzadi1*, Sara Aabroo2, Iqra Abdul Ghafoor3, Sidra Shafique4
*1Senior Lecturer, Riphah International University Lahore, Pakistan![]()
2Lecturer, Riphah International University Lahore, Pakistan![]()
3Lecturer, Riphah International University Lahore, Pakistan![]()
4Senior Lecturer, Riphah International University Lahore, Pakistan![]()
Abstract
Background and Aim: Sacroiliac joint pain is localized in the region of sacroiliac joint which can be increased by stress and provocation tests of the joint. Aim of this study was to compare two interventions for reduction of sacroiliac joint pain.
Methodology: Study design was randomized clinical trial. Study was conducted in bajwah hospital and children polyclinic Lahore. Duration of study was six months. The total sample size was 64 patients. Females of 20-50 years old with diagnosed sacroiliac joint pain were included in this study. Compression and distraction objective tests were performed for further confirmation of sacroiliac joint pain. Purposive sampling technique was used. Numeric pain rating scale (NPRS) and Oswestry low back disability questionnaire (ODI) were used to collect the data. Exclusion criteria was females with fractures and other abnormalities of spine.
Results: Results showed that both groups were equal when assessed on baseline by normality test colmogorov-smirnova. Independent t test was applied to compare the mean value of NPRS. Pretreatment mean of NPRS scale for both the regional treatment and standard treatment groups was 7.After 4 weeks NPRS of regional treatment group was 4 and of standard treatment group was 7. The mean value of pretreatment ODI for regional treatment group was 33 and for standard treatment group was 34.After 4 weeks ODI of regional treatment group was 24 and mean of standard treatment group was 27.
Conclusion: It is concluded that after giving equal sessions to both groups when results were assessed regional treatment is more effective than standard treatment.
Keywords: SIJ, ODI, NPRS, low back pain, regional treatment, enthesopathy.

Introduction
Sacroiliac joint has been thought of a significant reason for low back pain2. The sacroiliac joint (SIJ) can cause sciatica3. SI joint pain can be divided into intra-articular and extra articular regional pain. causes may include joint pain, spondyloarthropathies, and malignancies and causes of extra-articular pain includes enthesopathy, cracks, Ligamentous injury, wounds, and may facial damage4.Sacroiliac joint (SIJ) pain is an important source of mechanical low back pain, influencing somewhere in the range of 15 and 30% of people with persistent, non-radicular pain5. Although no single actual assessment or combined tests are needed to exaggerate pain during diagnosis there are some pain decreasing tests which can be used as diagnostic tests. Studies showed that intra articular injections reduce pain. People who do not respond to medical treatments they prefer intra articular injections. SIJ can also be painful due to muscular weakness and muscular spasm during stressful activities7. Ligaments and muscles completely support the SIJ when movements are performed on lower limbs9. Dangerous factors incorporate unusual step design, leg length disparity, scoliosis, substantial actual effort, injury, and pregnancy and lumbar combination medical procedure with obsession of the sacrum8. Many sacroiliac tests were performed for example Gaenslen’s test, pressure test, thigh trust, and Yeoman’s test. SIJ pain can be treated by using different manual therapy skills which includes mobilizations and muscular relaxation therapy14.
Methodology
Study design was randomized clinical trial the study was conducted in bajwah hospital and children polyclinic. Duration of study was six months. The total sample size was 64.The inclusion criteria was Females with diagnosed sacroiliac joint pain, age of patients was 20 to 50 years. The excluded population was patients with any warning signs i.e. tumor, fracture, metabolic infections, rheumatoid joint inflammation, delayed history of steroids use, females with sciatica ,females with transmitting pain in lumbar region and SIJ. Purposive sampling technique was used to gather the data. Tool was used Numeric pain rating scale (NPRS) and Oswestry low back disability questionnaire (ODI).Data was analyzed by SPSS V.21.
Results
Results showed that both groups were equal when assessed on baseline by normality test colmogorov-smirnova. Independent t test was applied to compare the mean value of NPRS. Pretreatment mean of NPRS scale for both the regional treatment and standard treatment groups was 7.After 4 weeks NPRS of regional treatment group was 4 and of standard treatment group was 7. The mean value of pretreatment ODI for regional treatment group was 33 and for standard treatment group was 34.After 4 weeks ODI of regional treatment group was 24 and mean of standard treatment group was 27.
Outcome Measures
NPRS and ODI tools were used to measure pain level and disability respectively. Both groups were given equal sessions of treatments. Regional treatment is more effective than standard treatment.
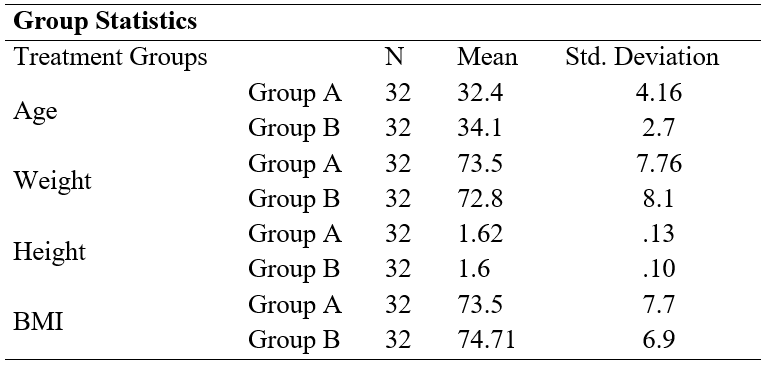
Table 1: Comparison of Demographic Variables of two Groups
The above drawn up table summed up the comparison of socio-demographic variables i.e. age, weight, height and Body Mass Index (BMI) across the two groups.
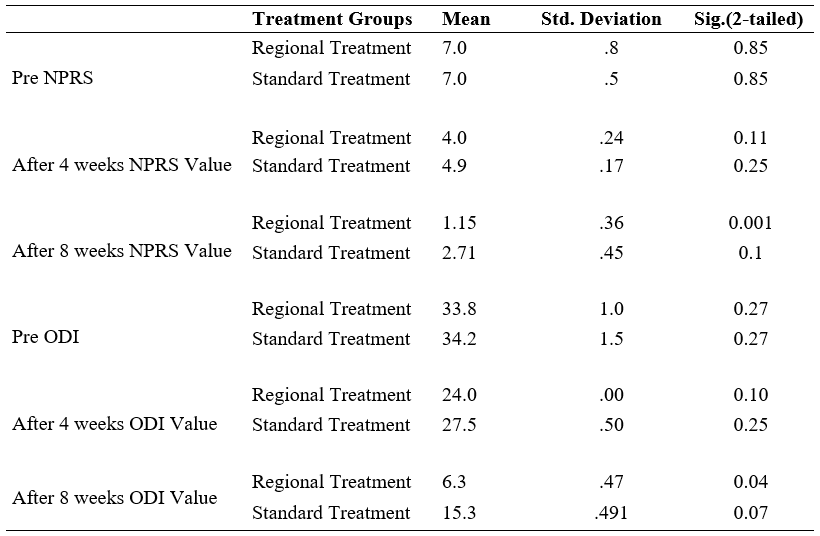
Table.2: Independent sample T-test
Table Showed pre treatment value of pain on NPRS which was same in both groups while after treatment it was more reduced in regional treatment group having value of 0.001.It also showed value of ODI which was also improved in regional treatment group having value of 0.04.
Discussion
The SIJ may also be treated during the treatment of pain in the low back and backside going into the upper leg and groin region. It is sometime ignored as a separate joint with different signs in patients of low back pain in lumbar region. Clinically, one can develop a clear diagnosis by seeing the patient’s sitting and walking positions and by performing two or three provocative tests and eagerly seeing where the patient shows indications16. A randomized clinical trial study was conducted in 2015 in which the impact of the treatment was assessed following 4 and 12 weeks. After effects Of the 51 patients, were effectively treated. Physiotherapy was beneficial in 4 out of 15 patients), manual treatment in 14 of the 18 and intra-articular injections in 7 of 18 (50 %) patients (p = 0.01). Manual treatment had preferable effects over physiotherapy and other interventions11.
The outcomes showed that physiotherapy inter sessions are effective in decreasing the pain related with SIJ dysfunction. In Another study which was conducted in 2018 effects of kinesio tape are assessed and conclusions were that kinesio taping are effective in the treatment of pain, disability and pelvic deviation in SIJ dysfunction15. In current study Group A was treated with regional physical therapy treatment. In this treatment patients were given mobilization to lumbar area and SIJ, pelvic floor exercises and Group B was treated with standard physiotherapy in which patients were given SIJ activation and Straight leg raise. Results showed that regional treatment is more effective than standard exercise based treatment.
Conclusion
Regional treatment is more effective than standard treatment.
AUTHORS’ CONTRIBUTION:
The following authors have made substantial contributions to the manuscript as under:
Conception or Design: Tasneem Shahzadi, Sara Aabroo,
Acquisition, Analysis or Interpretation of Data: Sidra Shafique
Manuscript Writing & Approval: Iqra Abdul Ghafoor
All authors acknowledge their accountability for all facets of the research, ensuring that any concerns regarding the accuracy or integrity of the work are duly investigated and resolved.
ACKNOWLEDGEMENTS: We thanks all the participants in this study.
INFORMED CONSENT: Written Informed Consent was taken from each patient.
CONFLICT OF INTEREST: The author (s) have no conflict of interest regarding any of the activity perform by PJR.
FUNDING STATEMENTS: None declared
ETHICS STATEMENTS: Work is ethically approved by higher authority and letter is attached with this abstract.
References
- Forst SL, Wheeler MT, Fortin JD, et al. The sacroiliac joint: anatomy, physiology and clinical significance. Pain Physician. 2016;9:61–67.
- Cohen SP (2015) Sacroiliac joint pain: a comprehensive review of anatomy, diagnosis, and treatment. AnesthAnalg 101:1440– 1453.
- Forst SL, Wheeler MT, Fortin JD, et al. The sacroiliac joint: anatomy, physiology and clinical significance. Pain Physician. 2016;9:61–67.
- Merskey H, Bogduk N. Classification of Chronic Pain: Descriptions of Chronic Pain Syndromes and Definitions of Pain Terms. 2nd ed. Seattle, WA: IASP Press; 2018.
- Cohen SP (2016) Sacroiliac joint pain: a comprehensive review of anatomy, diagnosis, and treatment. AnesthAnalg 101:1440– 1453.
- Solonen KA: The sacroiliac joint in the light of anatomical, roentgenological and clinical studies. Acta Orthop Scand 2017;27(suppl):1-127 Fortin JD, Dwyer AP, West S, et al: Sacroiliac joint: pain referral maps upon applying a newinjection/arthrography technique: part 1, asymptomatic volunteers. Spine 2017; 19(13):1475-1482.
- Schwarzer AC, Aprill CN, Bogduk N: The sacroiliac joint in chronic low back pain. Spine 2018;20(1):31-37 9.
- Dreyfuss P. Michaelsen M, Pauza K, et al: The value of medical history and physical examination in diagnosing sacroiliac joint pain. Spine 2018;21 (22):2594-2602.
- Hoek van Dijke GA, Snijders CJ. Stoeckart R, et al: A biomechanical model on muscle forces in the transfer of spinal load to the pelvis and legs. J Biomech 2018;32(9):927 -933 13.
- Sturesson B, Selvik G, Uden A: Movements of the sacroiliac joints: a roentgen stereophotogrammetric analysis. Spine 2018;14(2):162-165 21.
- Fortin JD, Aprill CN, Ponthieux B, Pier J. Sacroiliac joint: pain referral maps upon applying a new injection/arthrography technique. Part II: Clinical evaluation. Spine 19(13), 1483–1489 (2029).
- Murakami E, Aizawa T, Noguchi K, Kanno H, Okuno H, Uozumi H. Diagram specific to sacroiliac joint pain site indicated by one-finger test.J. Orthop. Sci. 13(6), 492–497 (2018).
- Slipman CW, Jackson HB, Lipetz JS, Chan KT, Lenrow D, Vresilovic EJ. Sacroiliac joint pain referral zones. Arch. Phys. Med. Rehabil. 81(3), 334–338 (2020).
- Laslett M. Evidence-based diagnosis and treatment of the painful sacroiliac joint. J. Man. Manip. Ther. 16(3), 142–152 (2018).
- Young S, Aprill C, Laslett M. Correlation of clinical examination characteristics with three sources of chronic low back pain. Spine J. 3(6), 460–465 (2017).
- Mason LW, Chopra I, Mohanty K. The percutaneous stabilisation of the sacroiliac joint with hollow modular anchorage screws: a prospective outcome study. Eur Spine J. 2020;22: 2325–2331.
- Sturesson B, Selvik G, Uden A: Movements of the sacroiliac joints: a roentgen stereophotogrammetric analysis. Spine 2018;14(2):162-165 21.
- Ponthieux B ,Fortin JD, Aprill CN, Ponthieux B, Pier J. Sacroiliac joint: pain referral maps upon applying a new injection/arthrography technique. Part II: Clinical evaluation.Spine 19(13), 1483–1489 (2020).
- Uozumi H,Murakami E, Aizawa T, Noguchi K, Kanno H, Okuno H, Uozumi H. Diagram specific to sacroiliac joint pain site indicated by one-finger test. J. Orthop. Sci. 13(6), 492–497 (2018).
- Jackson HB, Lipetz JS, Slipman CW, Jackson HB, Lipetz JS, Chan KT, Lenrow D, Vresilovic EJ. Sacroiliac joint pain referral zones. Arch. Phys. Med. Rehabil. 81(3), 334–338 (2020).
- Lipetz JS,Laslett M. Evidence-based diagnosis and treatment of the painful sacroiliac joint. J. Man. Manip. Ther. 16(3), 142–152 (2018).
- Lipetz JS, (2016) Sacroiliac joint pain: a comprehensive review of anatomy, diagnosis, and treatment. AnesthAnalg 101:1440– 1453.
- Forst SL, Wheeler MT, Fortin JD, et al. The sacroiliac joint: anatomy, physiology and clinical significance. Pain Physician. 2016;9:61–67.
- Merskey H, Bogduk N. Classification of Chronic Pain: Descriptions of Chronic Pain Syndromes and Definitions of Pain Terms. 2nd ed. Seattle, WA: IASP Press; 2016.
- Cohen SP (2015) Sacroiliac joint pain: a comprehensive review of anatomy, diagnosis, and treatment. AnesthAnalg 101:1440– 1453.
- Solonen KA: The sacroiliac joint in the light of anatomical, roentgenological and clinical studies. Acta Orthop Scand 2015;27(suppl):1-127 Fortin JD, Dwyer AP, West S, et al: Sacroiliac joint: pain referral maps upon applying a newinjection/arthrography technique: part 1, asymptomatic volunteers. Spine 2015; 19(13):1475-1482.
The Ziauddin University is on the list of I4OA, I4OC, and JISC.
This is an open- access article distributed under the terms of the Creative Commons Attribution License (CC BY 4.0).