
ABSTRACT
OBJECTIVE
To compare the effects of deep friction massage and ultrasound therapy in subjects with tennis elbow in terms of pain, grip strength and functional activities.
STUDY DESIGN
Randomized Control Trial.
STUDY SETTINGS AND PARTICIPANTS
Study was conducted in Physiotherapy OPD of a tertiary care hospital. A sample of 50 patients were inducted in the study. Sample size calculated through open Epi calculator.
OUTCOME MEASURES
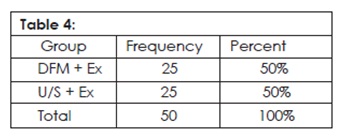
Patients with the diagnosed lateral epicondylitis (Tennis elbow) presenting to out Patient department of two tertiary care hospitals has been enrolled for study after written informed consent. Subjects were randomly allocated into two groups i.e., group A and group B. Group A = DFM + exercise, Group B = U/S + exercise.
RESULTS
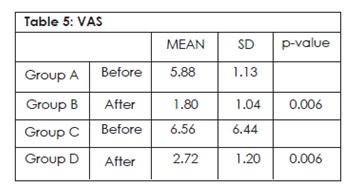
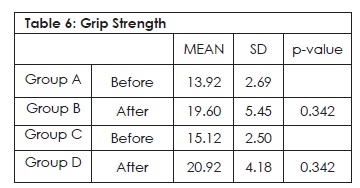
Total 50 patients were randomized and divided into two groups. Group A: the mean pain score on VAS before treatment was 5.88±1.130 and after treatment 1.80±1.041 p-value=0.006. Group B: the mean pain score on VAS before treatment was 6.56±1.446 and after treatment was 2.72±1.208 p-value=0.006. Group A: the mean grip strength score was 13.92±2.691 and in after treatment was 19.60±5.454 p-value=0.342. Group B: the mean grip strength was 15.12±2.505 and after treatment was 20.92±4.183p-value=0.342.
CONCLUSION
The present study showed no statistical difference in using deep frictional massage therapy in relieving pain, improving grip strength and functional performance in subject with tennis elbow.
KEY WORDS
Tennis Elbow, Lateral Epicondylitis, Deep Friction Massage, Hand Held Dynamometer, Ultrasound Therapy, Grip Strength.
Jetindar Puri
physiotherapist
Physiotherapy department
Agha Khan University
Dr Nabiha Ahmed
Senior lecturer
Assistant Manager
Physiotherapy department
Ziauddin hospital Clifton
[Puri J, Ahmed N. Effects of DeepFriction Massage on Tendinitis (Lateral Epicondylitis) in Comparison to Ultrasound Therapy. Pak. j. rehabil. 2014;3(2):36-40]
INTRODUCTION
Lateral Epicondylitis is commonly known as tennis elbow. It is characterized by an insidious onset of elbow pain on extension of wrist, during pronation or supination and aggravated by gripping action of the hand, such as holding tools, shaking hands, and lifting a kettle. This condition was first named by Morris (1882) who called it lawn tennis arm1-3.
Lateral epicondylitis affects 1-3% of the population, only 5% of all patients seen are recreational tennis players. Although the syndrome has been identified in patients ranging from 20 to 60 years of age, it predominantly occurs in the fourth and fifth decades. Male and female prevalence rates are reportedly equal. Seventy-five percent of patients are symptomatic in their dominant arms4-7. A study conducted by Verhaar (1994) revealed that between the ages of 40 and 60 years, 10% of women and only 3% of men were affected8.
The specific muscle that is most often implicated clinically and surgically is the extensor carpi radialis brevis with occasional involvement of the extensor digitorum communis, extensor carpi radialis longus, and extensor carpi ulnaris. The possible reason for the frequent involvement of the extensor carpi radialis brevis is its location as one of the most laterally situated muscles on the lateral epicondyle with slips taking origin from the radial collateral ligament9. The extensor carpi radialis brevis is intimately attached to the joint capsule, which is continuous with the radial collateral ligament and because of this proximity adhesions are more likely10
Treatment options for lateral epicondylitis includes therapeutic ultrasound, phonophoresis, corticosteroid injections, acupuncture, electromagnetic field therapy, extracorporeal shockwave therapy, laser, deep transverse friction massage, cervical spine mobilization, taping, elbow joint mobilization, exercise elbow cuff, and surgery10.
Deep transverse friction (DTF) is also known as deep friction massage is a specific type of connective tissue massage applied precisely to the soft tissue structures such as tendons. It was developed in an empirical way by cyriax and is currently used extensively in rehabilitation practice11. It is a common clinical observation that application of DTF leads to immediate pain relief, the patient experiences a numbing effect during the session. Reassessment immediately after it shows reduction in pain and increase in strength and mobility. A number of hypotheses to explain the pain-relieving effect of DTF have been put forward. Absolute contraindications to DTF are few12. It is never applied over active infections, bursitis and disorders of nerve structures, ossification and calcification of soft tissue, or active rheumatoid arthritis, care is required if there is fragile skin or the patient is on anticoagulant treatment13.
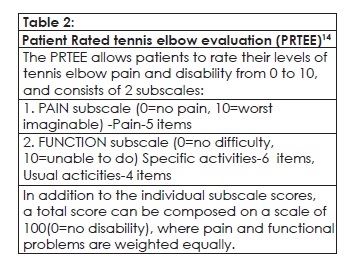
The PRTEE, formerly known as the Patient-Rated Forearm Evaluation Questionnaire (PRFEQ), is a 15-item questionnaire designed to measure forearm pain and disability in patients with lateral epicondylitis (also known as “tennis elbow”)14.
METHODOLOGY
Study Design
Randomized Control Trial
Sources of Data
Study was conducted in 3 renowned tertiary care hospitals.
Duration of Study
Six months
Sampling Technique
Simple Random Sampling.
Sampling Method
Subjects were randomly allocated into two groups i.e. group A and group B.
Group A: DFM + Exercises
Group B: Ultrasound +Exercises
Sample Size
A sample of 50 patients was inducted in the study and
divided into two groups.
Group A: 25 participants.
Group B: 25 participants.
Inclusion Criteria
- Both male and female between 20 to 50years of age.
- Pain and tenderness over the forearm extensor muscles origin.
- Pain with 1 of the following positive tests: Mill’s test, Cozens test, Maudsley’s tests15,16,17.
Exclusion Criteria
- History of fracture at the elbow joint.
- If full extension is not obtained at elbow. Hyper mobile joints.
- Sensitive skin.
- A recent steroid injection during last 3 months.
Data Collection Tool
Patient-Rated Forearm Evaluation Questionnaire Hand held dynamometer– Baseline evaluation instrument.
Data Collection Procedure
The purpose of this study has been explained and a written informed consent was obtained from all the participants. The subjects were screened based on the inclusion and exclusion criteria. Demographic data was collected along with initial assessment of VAS, grip strength, Patient rated forearm evaluation questionnaire for lateral epicondylitis. After initial assessment they were allocated into 2 groups Group A and Group B with equal no of participants in each group
Both groups received the selected treatment for 1 session per day for 7 days continuously.
Group A – Deep friction massage + Exercise
Group B – Therapeutic Ultrasound + Exercise
Data Analysis Procedure
Data was entered in SPSS Version 20. Frequencies and percentages were taken out for all categorical variables. Independent T test was applied as test of significance to find association between two categorical variables. P-value less than 0.5, considered significant.
RESULT
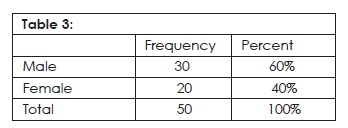
All assessments are recorded using pre-structured, standardized forms. Outcome assessments are done by the trial doctors and by the patient answering a questionnaire. Based on earlier studies and assessment of the validity and reliability of the outcome measures, the patient’s evaluation of improvement will be registered on a 6-point Likert scale (much worse – worse – a little worse – some improvement- much improvement – completely recovered). A total of 50 patients were randomized and divided into two equal groups. 30 male and 20 female patients [mean age 37.62 +7.44 (range 20-50 years)] were allocated (Table 3).
After the treatment sessions all 50 patients were present to be re-assessed. Group frequencies are show in table 04. The patients were treated for 6 months at hospital under the supervision of physical therapist.
Group A: The result shows that the mean pain score of VAS before treatment 5.88 ± 1.130, but after treatment VAS score were decreased and intensity of pain was 1.80 ± 1.041. P-value 0.006.Frequency of pain score is mentioned in Table 5. Group B: it has been observed that mean pain score of VAS before treatment was 6.56±1.446 and after treatment it was decreased and new value 2.72±1.208. P-value=0.006. Table 05 present group B values.
It has been observed the mean of grip strength in group A before the treatment was 13.92 ± 2.69 and after treatment the score was 19.60 ± 5.45. The result of group B shows that the mean of grip strength before the treatment was 15.12 ± 2.50 but after treatment score decreased, new value was 20.92 ± 4.18. All values are mentioned in table 06.
DISCUSSION
Earlier studies, including meta-analyses, have determined that more researches on treatment options for lateral epicondylitis is required for making effective and sound treatment decisions, so evidence based treatment guideline should be incorporated.
This study was designed to mirror the normal work flow in a primary care setting, for making the result readily applicable in this setting. We have selected current onset complaints as conflicting to recurring or severe form for easier comparison with earlier research, and also make the result more applicable in general training. It is established that a treatment protocol reflecting usual treatment for this condition is essential18. With the help of assessment the patients’ time off paid service, we are hopeful to gain valuable awareness about the financial impacts of this condition.
To address the methodological problems in some earlier researches, we have designed our research as a randomized controlled study with the time period of six months. We observed that the deep frictional massage with exercises were more valid as compared to ultrasound therapy with exercises.
The deep frictional massage lead to immediate pain relief that is a common clinical observation18. Some patients experienced numbing effect during the treatment session.
The Symptoms of some patients were reassessed immediately after the application of deep frictional massage, result showed reduction of pain and improved strength and mobility18.
Many theories and studies have been put forth to describe the pain relieving effects of DTF. According to Cyriax and Cyriax, DTF also lead to decreased pain provoking metabolites such as Lewis’s substances19. Another mechanism by which reduction in pain may be achieved through diffused noxious inhibitory controls, a pain suppression mechanism that releases erogenous opiates.
Study was done by G Ebenbichler et al in 1999 was on the patients having calcify shoulder tendinitis, for that purpose 63 participants were selected to find out the therapeutic effects of ultrasound in shoulder calcific tendinitis20. The conclusion of the study was that ultrasound help in resolving the calcification. It also decreases pain, improves one’s quality of life20.
In 1985 Binder et al tested the effectiveness of ultrasound; they took a group of individuals who were suffering from soft tissue lesions21. It was concluded through the study that ultrasound treatment enhances the recovery in most individuals with lateral epicondylitis. in one of the other studies done by Tim Noteboom et al10 in 1994, also point out that chronic symptom are usually linked to inadequate muscle power as well as muscle endurance. Jamar hand dynamometer was used in the study for the assessment of the grip22. Grip strength reduction was the obvious sign observed through the study. To overcome such deficiency a supervised strengthening exercise program was prescribed23.
During the research being done the participants of both groups were treated by applying strengthening as well as stretching exercises. These different types of exercises are necessary to enhance the repetitive wrist movement. These exercises are found to be beneficial for damaged wrist extensors24.
Through out the study it was observed that literatures have mentioned that strengthening exercise and stretching exercise both are effective whenever rehabilitation of tennis elbow is required. Stretching exercises to keep the tendon flexible and strengthening exercises to develop strength in the muscles. Positive effects of exercise program for tendon injuries may be attributable to lengthening of tendon by stretching and strength of muscles by strengthening exercises. Loading effect must be achieved in tendon of muscle, and tensile strength of muscle tendon must be improved25.
CONCLUSION
This study supported the deep frictional massage therapy as a useful technique for relieving pain and improving grip strength in subject with tennis elbow. It also revealed that deep frictional massage is more effective in reducing pain in comparison with ultrasound therapy. This evidence will promote a more efficient treatment option for the management of tennis elbow.
Ethical Consideration
According to ethical consideration Patient privacy, Patient hygiene factor, Patient therapist relationship and Environment of the place where we treat the patient were given due importance.
ACKNOWLEDGMENTS
I am really thankful to the Almighty who has provided me with the opportunity to study and make my dream possible.
I would like to thank my parents, siblings whose valuable support encouraged me and gave me the confidence throughout the study. I would like to thank all the subjects who were a part of our study without which this task would not have been possible.
REFERENCES
- Vicenzino B, Brooksbank J, Minto J, Offord S, Paungmali A (2003) Initial effects of elbow taping on pain-free grip strengthand pressure pain threshold. J Orthop Sports Phys Ther. July 2003;33(7):400-07.
- Cyraix J. Book of Orthopaedic Medicine. 11th ed. 2000;Vol 1. AICBS Publications; Delhi
- Kushner S, Reid DC. Manipulation in the treatment of tennis elbow. J Orthop Sports Phys Ther. 1986; 7(5):264-72
- Wendy-Ann Wood, Aimee Strwart Lateral epicondylalgiaan overview. Physical Therapy Reviews 2006;11:155-160
- Stasinopoulos D, Johnson MI. Cyriax physiotherapy for tennis elbow/lateral epicondylitis. Br J Sports Med 2004;38(6):675-677.
- Ciccotti MC, Schwartz MA, Ciccotti MG. Diagnosis and treatment of medial epicondylitis of the elbow. Clin Sports Med 2004;23(4):693-705, xi.
- Stoeckart R, Vleeming A, Snijders CI. Anatomy of the extensor carpi radialis brevis muscle related to tennis elbow. Clin Biomech 1987;4:10-12.
- Verhaar JA. Tennis elbow. Anatomical, epidemiological and therapeutic aspects. Int Orthop 1994;18:263-7
- Brotzman SB, Wilk KE. Clinical Orthopedics Rehablitation, 2nded, Mosby: St Louis, MO: 2003
- Noteboom T, Cruver R, Keller J, Kellogg B, Nitz AJ. Tennis Elbow: A Review, JOSPT June 1994;19(6):357-366
- Stasinopoulos D, Stasinopoulos I. Comparison of effects of cyriax physiotherapy, a supervised exercise programme, and polarized polychromatic non–coherent light (Bioptronlight) for the treatment of lateral epicondylitis. Clin, Rehab. 2006;20:12-23.
- Low J, Read A, Electrotherapy Explained, principles and practice. 3rd ed, 2000, Butterworth Heinemann.
- O’Sullivan SB. Schmitz TJ. Physical Rehabilitation: Assessment and Treatment. 5thEd. Jaypee Brothers: New Delhi 2001:316:825-937
- MacDermid JC. Patient Rated Tennis Elbow Evaluation (PRTEE), User manual dec 2007;1-15
- Stratford P, Levy D, Gowl and C: Evaluative properties of measures used to assess patients with lateral epicondylitis at the elbow. Physiother Can. 1993;45:160-164.
- Ng GYF, Fan ACC. Does elbow position affect strength and reproducibility of power grip measurements? Physiotherapy. 2001;87(2):68-72
- Leung HB, Yen CH, Tse PY. Reliability of Hong Kong Chinese version of the Patient-rated Forearm Evaluation Questionnaire for lateral epicondylitis. Hong Kong Med J June 2004;10(3):172-77.
- De Bruijn R. Deep transverse friction: its analgesic effect. Int J Sports Med 1984;5:35-36
- [Stasinopoulos D, Johnson MI. Cyriax physiotherapy for tennis elbow / lateral epicondylitis. Br J Sports Med 2004;38(6):675-677.
- Ebenbichler GR, ERDOGMUS CB, RESCH KL, FUNOVICS MA, KAINBERGER F, BARISANI G, et al. Ultrasound therapy for calcific tendinitis of the shoulder. The new England journal of medicine. 1999;340(20):1533-1538.
- Binder A, Hodge G. Is therapeutic ultrasound effective in treating soft tissue lesions. Br Medical J. 1985;290:512-514
- Soderberg J, Grooten W J, Ang BO, Effects of eccentric training on hand strength in subjects with lateral epicondyltis: A randomized controlled trial, Sc and J Med Sci Sport, 2012;22(6):797–803.
- Manias P, Stasinopoulos D. A controlled clinical pilot trial to study the effectiveness of ice as a supplement to the exercise programmed for the management of lateral elbow tendonopathy, Br. J sports Med, Jan, 2006;40(1):81-85
- Page P. A new exercise for tennis elbow that works. N Am J Sports Phys Ther. 2010 Sep; 5(3): 189–193.
- Jarvinen AHT, Jarvinen M, Kalimo H. Regeneration of injured skeletal muscles after the injury. Muscles Ligaments Tendons J. 2013 Oct-Dec; 3(4): 337–345.