
ABSTRACT
OBJECTIVE
To investigate the frequency of elevated resting heart rate among young adult population of ZCRS.
METHODOLOGY
This cross sectional study was conducted at a private sector University with 363 participants, within age group of 18-30, under consideration. The participants underwent an assessment of heart rate at rest with pulse oximeter, height and weight by stadiometer. IBM SPSS version 20 with a Confidence interval of 95% was used for the statistical analysis. The association of elevated Resting Heart Rate and Body Mass Index was assessed. In addition to this gender association elevated were also evaluated.
RESULT
The incidence of Elevated RHR with a mean of 95.30 ± 3.25 was found to be 27.04 percent. Also, 22.44 percent of participants had their heart rate with a mean heart rate of 108.40 ± 6.69 in the tachycardia category, which showed the increased risk of CVD events in the near future. In BMI’s view, there was no important correlation found between RHR and BMI jointly and in individual classifications (P>0.05).
CONCLUSION
The results revealed that resting heart rate was elevated among half of the population that may be a risk factor for cardiovascular events in future.
This is an open-access article distributed under the terms of the Creative
Commons Attribution Licence (CC BY) 4.0 https://creativecommons.
KEYWORDS
Heart rate, elevated resting heart rate, RHR, Cardiovascular Disease, Young Adults, risk factors modification
Atta Muhammad
Manager
Department of Physical Therapy
Agha Khan University
[Muhammad A.Prevalence of Elevated Resting Heart Rate Among Young AdultsPak.j.rehabil.2020;9(2):60-65]
DOI:10.36283/pjr.zu.9.2/012
The cardiovascular disease CVD is universally reported to be a lethal debility for all genders as a study in 2008 estimated the death ratio because of cardiovascular disease which was delineated to be 17.3 million that is approximately 30% of all deaths1.
Death rate because of cardiovascular disease is anticipated to rise to 23.4 million by 2030 globally2. In South Asia the population is deduced to be at risk for cardiovascular disease due to conditioning factors like, socioeconomic status, early life influences, education and awareness2. The latest WHO data published in 2017 states that deaths in Pakistan because of cardiovascular disease has outreached to be 21.76% of total number of death. Pakistan ranks 13th with reference to the age adjusted death Rate2.
Cardiovascular disease refers to the condition that include narrowing of blood vessels and weakening of cardiac musculature that manifest into numerous complications like myocardial infarction, ischemia, stroke, angina pectoris, cardiomyopathies and valvular heart disease3. A number of risk factor like hypertension, dyslipidemia, obesity, diabetes mellitus, and atherosclerosis are associated with aforementioned cardiovascular complications3.
Conversely, a risk factor that has not classically gained significance is an elevated resting heart rate. However, it has acquired attention over last few decades4. Existing literature reports elevated resting heart rate as the prime marker for cardiovascular disease among many others4. Moreover, for the assessment of cardiac functionality it is a valid and measureable asset5. The resting heart rate is elucidated as the number of beats in a minute while an individual is in the state of rest6. Moreover, the average value of a normal resting heart rate as indicated by American Heart Association AHA is specified between 60-100 beats per minute, which alters with a number of factors6. Exercise, medications, emotional stress, Cardio vascular diseases, hydration, body size is among the factors that have either a positive or negative influence on a resting heart rate7.
It is crucial to understand the importance of an elevated resting heart rate, since it is a prominent indicator of declining physical health and reduced cardiovascular fitness as the literature yields evidence that anchors on elevated resting heart rate being a key factor of risk among8. An increase in the values of resting heart rate of 10 beats per minute increases the incidence of cardiovascular and non-cardiovascular death up to 21 to 24%9. It is also claimed that a rise of 20% in cardiovascular related death and hypertension in individuals has occurred due to a rise of 10 beats per minute in the values of resting heart rate10. One author states that, an increase of cardiovascular death and heart failure was 3% for every 1 beats per minute increase and 16% for every increment of 5 beats per minute11. The deaths related to the cardiovascular cause were found to be twice in individuals who had an elevation in the heart rate of up to 90 beats per minute as compared to the individuals who did not had an elevation10. A rise in the resting heart rate, in hypertensive individuals, of greater than 80 beats per minute contributes to a mortality risk of 1.38 in comparison to a lower resting heart rate of 60 beats per minute4. Both cardiovascular and non-cardiovascular related risk factors are found to be related to an elevated resting heart rate9. Literature advocates that some of the factors are modifiable that can control and prevent the occurrence of the diseases; these include smoking, obesity, alcohol consumption, blood pressure, and cholesterol12. Contrariwise, the non-modifiable factors include age, gender, and familial predisposition13. It is reported in a study that resting heart rate is upraised in obese individuals as a result of cardiac hypertrophy and increased cardiac output 14. Outcomes of another study suggested that a disturbance in the baroreceptor sensitivity occurs due to immense consumption of nicotine smoke, leading to a malfunction in the negative feedback system which causes a disruption in the autonomic system making smoking a probable cause of elevation of the resting heart rate 15. A study conducted by Wang tremendously emphasizes an elevation in the resting heart rate, in the individuals of developed and developing countries, contributing as being a risk factor for diabetes. Moreover, the populations of Asian and outside it are also vulnerable to this root16. One author proclaims that, one of the causes of elevated resting heart rate is epinephrine, cortisol, IL6 and corticosterone release to prepare body for flight and fight response 17. A decrease in the periods of sleep may contribute as a stimulant for stress affecting the sympathetic activity of the body, which tends to be a cause for the elevation in the resting heart rate 18. The literature has reported that adolescents with better performance in physical fitness test have lower odds of high blood pressure, hypercholesterolemia and cardiovascular dysfunction19. Subjects with greater physical fitness capability were found to have low values of resting heart rate 20. Based upon these findings, it is now evident that resting heart rate should now be dealt as importantly as other risk factors like hyperlipidemia and hypertension have been 21.
However, there is no study found to be conducted in Pakistan that investigates the prevalence of elevated resting heart rate, especially in young adults. Thus, in order to enhance the awareness of elevated resting heart rate as a self-standing factor for the plausibility of cardiovascular disease, in Pakistan a prevalence study is necessitated to identify the population at risk and to provide guide lines and forestall the future generations.
Study design
Cross-sectional study design.
Sample size
The population sample was taken from a private institute. The total screening was of 420 students present at the time of screening at the college campus; only 392 students were recruited as participants after excluding those who were not fulfilling the inclusion criteria.
Sampling technique
Purposive sampling was used to collect the data for the study.
Inclusion criteria
Normal healthy young adults of age 18 to 30 years.
Exclusion criteria
Myocardial infarction, Arrhythmias, Cardiomegaly, Malignancy, Endocarditis , Myocarditis, Recent trauma , Cardiac surgery and People receiving beta blockers
Data collection procedure
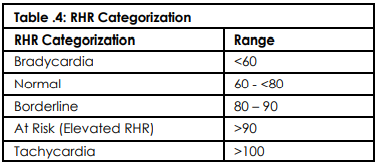
A written consent was taken from the participants. Using the assessment form generated by researchers, demographic data, height, and weight were collected. Evaluation of resting heart rate and BMI were performed. For resting heart rate, the participants were given a rest of 5 minutes prior to the assessment and 3 simultaneous readings of the heart rate were recorded with pulse oximeter, and the mean of the three readings was documented. BMI was calculated from the universal formula and interpretations were made based upon the standard universal values. The resting heart rate of young adult was classified into bradycardia, normal, elevated resting heart rate and tachycardia.
Data collection tools
- Pulse oximeter
- Stadiometer
- Weighing machine
- Assessment form to record HR and BMI
Data analysis method
Data analysis was performed in our study using the 20.0 version of SPSS. The baseline characteristics of participant were determined through descriptive statistics by using Frequency, Mean and Standard deviation. Furthermore, the prevalence of the elevated Resting Heart Rate was also described in terms of frequencies
The test of normality was run to determine the distribution of data through skewness and kurtosis that revealed the asymmetrical nature of data. Therefore, non-parametric Chi-Square testing was applied to investigate the association between Elevated RHR and gender whereas Spearman Co-efficient of Correlation was run to determine the relationship between Elevated RHR. Statistically, the values were analyzed at the Confidence Interval of 95% considering the p-value < 0.05.
Autonomy to participate in the study was given to the participants Confidentiality of the participants was not breached Participants were given the right to with draw from the study anytime. All the causations of harm towards the participants were avoided.
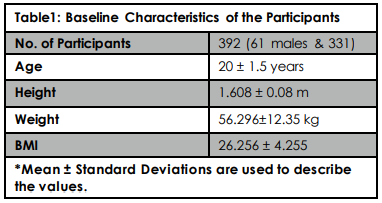
A total sample of 392 young adult participants consisting of 61 males and 331 females were recruited for the study among young adult students of ZCRS. The baseline characteristics of the participants including mean age 20.26 ± 1.52, height, weight and BMI as shown in table:1
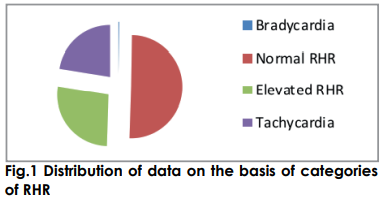
Investigating the readings of Resting Heart Rate (RHR) among the young adult participants, the prevalence of the elevated RHR (HR= 90-100 bpm) was found 27.04% with a mean RHR of 95.30 bpm ± 3.25. Furthermore, 22.44% participants were found to be tachycardic (HR>100 bpm) with a mean heart rate of 108.40 bpm ± 6.69 while 17.85 % participants lied in normal RHR category (HR=60-90) with mean heart rate of 81.19 bpm ± 6.65. Exclusively, only one participant was categorized as bradycardic with heart rate of 60 bpm as shown in figure 1.
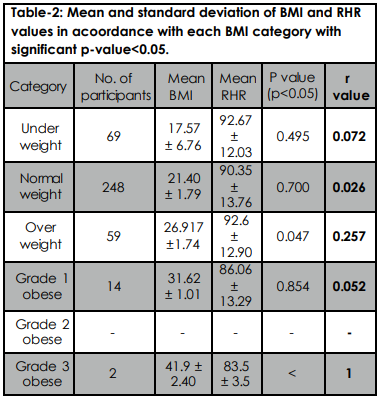
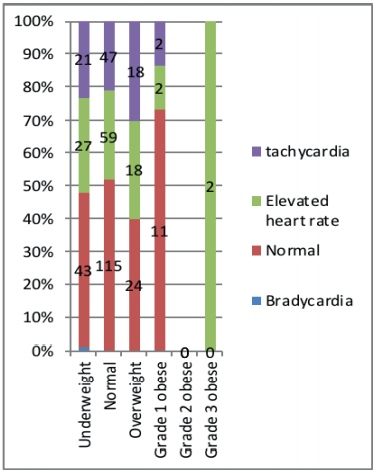
The Spearman Co-efficient of Correlation was applied to investigate the association between RHR and BMI categorizing it into Underweight, Normal, Overweight, Obesity grade I, grade II and grade III respectively. Statistically, the significant association between RHR and BMI was found in the grade 3 obese individuals (r =1, p Moreover, a fair degree of association was in overweight category (r=0.257, p= 0.047). In contrast no significant correlation was found among the categories of Underweight as shown in figure 2.
Additionally, the association between the categorical variable i.e. gender and RHR was investigated employing Chi-Square Test. The test revealed no statistical significant relationship between gender and RHR (p= 0.493) as demonstrated in table 3.
Fig.2: Prevalence of each class of RHR with respect to BMI in young adult
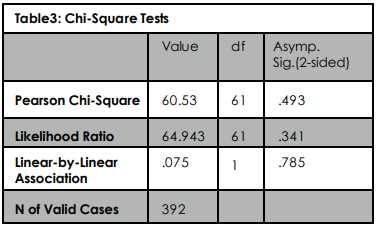
However, the mean RHR values for both genders were observed to be 90.77 ± 15.74 and 91.31 ± 11.92 respectively that shows very less variation between the two means.
According to our study the prevalence of RHR found in the young adult population of ZCRS was found to be 27% which surprisingly is a high value, indicating 27% of the ZCRS population at risk. Our study aimed to distinctly classify the population at risk, i-e individuals falling in an elevated RHR category, and the population who already has crossed the borderline of risk, i.e. individuals falling in the category of tachycardia, which according to our knowledge no other study has done presently. We stratified the resting heart rate as shown in the table 422;
Among the target population only 17% showed normal RHR values which assuredly is an indicator of poor cardiovascular functionality in this population. In contrast to it the individuals with tachycardia appears to be 22%, who are already amid cardiovascular deconditioning. Perret-Guillaume, et al in their study in 2009 found great risk of cardiovascular death on RHR values greater than 90bpm, which impelled them to set the criteria for tachycardia in their population at 80-85%10. Aforementioned study is a consolidated proof of a direct association between higher RHR and cardiovascular related deaths.
Compellingly, one participant, who appears to be an athlete, showed a RHR value of 60bpm, driving our concerns to the significance of physical fitness which possibly would prevent a number of cardiovascular conditions as Silva, et al in 2018 concluded with their study as well19. Aeschbacher, et al. in 2015 also implied lifestyle modifications as a plausible factor to reduce cardiovascular events risks5 . With regard to the literature BMI and RHR were considered confounding over each other, which amazingly contradicts our results. In our study no significant association was witnessed between BMI and RHR in the young population of ZCRS, except for two categories namely overweight with a P value of 0.047 and r value of 0.257 and grade 3 obese having a r value of 1, leaving all other categories insignificantly associated which is certainly is questionable. Although, Yar in 2010 studied Saudi population and found RHR values to be elevated among obese individuals, and Silva, et al. in 2018 found skin fold thickness to be directly associated with RHR19, 23. With regard to the literature further investigation is required in this context. In consideration to past studies gender and RHR have been found to have an association, as Farah, et al. in 2015 found RHR to be gender dependent, with regard to the studies carried out in past, our study in ZCRS population showed no association between gender and RHR at all, which probably would be because of contemplating one risk factor namely obesity, and a significantly larger female population in comparison to male population24. Moreover, risk of cardiovascular disease has increased more in young adults during last two decades in due to prevalent risk factors like obesity and sedentary life-style25.
The study revealed significantly high percentages of young adults with elevated RHR as that itself is an independent risk factor for cardiovascular disease. Hence, there is an inevitable need of awareness programs for early detection of disease, promotion of healthy life style and behavioral modifications in order to reduce the future risk of cardiovascular disease especially young adults.
- int. (2018). [online] Available at: http://www.who.int/nutrition/publications/bmi_asia_strategies.pdf [Accessed 13 Sep. 2018].
- World Life Expectancy. (2018). Coronary Heart Disease in Pakistan. [online] Available at: http://www.worldlifeexpectancy.com/pakistan-coronary-heart-disease [Accessed 13 Sep. 2018]
- Mayo Clinic. (2018). 2 easy, accurate ways to measure your heart rate. [online] Available at: https://www.mayoclinic.org/healthy-lifestyle/fitness/expert-answers/heart-rate/faq-20057979. [Accessed 13 Sep. 2018]
- Saxena A, Minton D, Lee DC, Sui X, Fayad R, Lavie CJ, Blair SN. Protective role of resting heart rate on all-cause and cardiovascular disease mortality. Mayo Clinic Proceedings 2013;88(12):1420-1426).
- Aeschbacher S, Bossard M, Ruperti Repilado FJ, Good N, Schoen T, Zimny M, Probst-Hensch NM, Schmidt-Trucksäss A, Risch M, Risch L, Conen D. Healthy lifestyle and heart rate variability in young adults. Eur. J. Prev. Cardiol. 2016;23(10):1037-44.
- heart.org. (2018). All About Heart Rate (Pulse). [online] Available at:http://www.heart.org/en/health-topics/high-blood-pressure/the-facts-about-high-blood-pressure/all-about-heart-rate-pulse [Accessed 13. 2018].
- Earnest CP, Jurca R, Church T, Chicharro JL, Hoyos J, Lucia A. Relation between physical exertion and heart rate variability characteristics in professional cyclists during the Tour of Spain. Br. J. Sports Med 2004;38(5):568-75.
- Caetano J, Alves JD. Heart rate and cardiovascular protection. Eur. J. Intern. Med.. 2015;26(4):217-22.
- Alhalabi L, Singleton MJ, Oseni AO, Shah AJ, Zhang ZM, Soliman EZ. Relation of higher resting heart rate to risk of cardiovascular versus noncardiovascular death. The American journal of cardiology. 2017;119(7):1003-7.
- Perret-Guillaume C, Joly L, Benetos A. Heart rate as a risk factor for cardiovascular disease. Progress in cardiovascular diseases. 2009 Jul 1;52(1):6-10.
- Böhm M, Reil JC, Deedwania P, Kim JB, Borer JS. Resting heart rate: risk indicator and emerging risk factor in cardiovascular disease. The American journal of medicine. 2015 Mar 1;128(3):219-28.
- heart.org. (2018). Understand Your Risks to Prevent a Heart Attack. [online] Available at: http://www.heart.org/en/health-topics/heart-attack/understand-your-risks-to-prevent-a-heart-attack [Accessed 13 Sep. 2018]
- Hill LK, Hu DD, Koenig J, Sollers III JJ, Kapuku G, Wang X, Snieder H, Thayer JF. Ethnic differences in resting heart rate variability: a systematic review and meta-analysis. Psychosomatic medicine. 2015 Jan;77(1):16.
- Lee JF, Harrison ML, Christmas KM, Kim K, Hurr C, Brothers RM. Elevated resting heart rate and reduced orthostatic tolerance in obese humans. Clinical Autonomic Research. 2014;24(1):39-46..
- Opdahl A, Venkatesh BA, Fernandes VR, Wu CO, Nasir K, Choi EY, Almeida AL, Rosen B, Carvalho B, Edvardsen T, Bluemke DA. Resting heart rate as predictor for left ventricular dysfunction and heart failure: MESA (Multi-Ethnic Study of Atherosclerosis). Journal of the American College of Cardiology. 2014;63(12):1182-9..
- Wang L, Cui L, Wang Y, Vaidya A, Chen S, Zhang C, Zhu Y, Li D, Hu FB, Wu S, Gao X. Resting heart rate and the risk of developing impaired fasting glucose and diabetes: the Kailuan prospective study. International journal of epidemiology. 2015;44(2):689-99..
- Wiczynski T. Interactions between Aerobic Exercise Volume, Academic Stress, and Immune Function.
- Fernandes RA, Ronque ER, Venturini D, Barbosa DS, Silva DP, Cogo CT, Carnelossi MS, Batista MB, Coelho-e-Silva MJ, Sardinha LB, Cyrino ES. Resting heart rate: its correlations and potential for screening metabolic dysfunctions in adolescents. BMC pediatrics. 2013;13(1):48.
- Silva DA, Lima TR, Tremblay MS. Association between resting heart rate and health-related physical fitness in brazilian adolescents. BioMed research international. 2018;2018.
- Jensen MT, Suadicani P, Hein HO, Gyntelberg F. Elevated resting heart rate, physical fitness and all-cause mortality: a 16-year follow-up in the Copenhagen Male Study. Heart. 2013 15;99(12):882-7.
- Jiang X, Liu X, Wu S, Zhang GQ, Peng M, Wu Y, Zheng X, Ruan C, Zhang W. Metabolic syndrome is associated with and predicted by resting heart rate: a cross-sectional and longitudinal study. Heart. 2015;101(1):44-9..
- Anon . Your Resting Heart Rate: What Is Normal and Healthy? Resting Heart Rate Chart | Healthy Heart Rate. 2015;1(1)
- Lee JF, Harrison ML, Christmas KM, Kim K, Hurr C, Brothers RM. Elevated resting heart rate and reduced orthostatic tolerance in obese humans. Clinical Autonomic Research. 2014;24(1):39-46.
- Farah BQ, Christofaro DG, Balagopal PB, Cavalcante BR, de Barros MV, Ritti-Dias RM. Association between resting heart rate and cardiovascular risk factors in adolescents. European journal of pediatrics. 2015;174(12):1621-8.
- Andersson C, Vasan RS. Epidemiology of cardiovascular disease in young individuals. Nature Reviews Cardiology. 2018 ;15(4):230.