
ABSTRACT
OBJECTIVES
The incidence of stroke is high among the Pakistani population as compared to developed countries. Studies concluded that home-based rehabilitation therapy increases the quality of life of survivors; however, it also increases the burden on rehabilitation therapists. Thus, this study aims to investigate the association between the level of burden and quality of the therapist’s life to address health-related outcomes
STUDY DESIGN
Cross-sectional survey.
STUDY SETTINGS & PARTICIPANTS
Total numbers of 100 therapists working in home-based rehabilitation were selected through the non-probability sampling technique. The data was collected through the World Health Organization Quality Of Life (WHQoL) questionnaire and Zarit Burden Interview.
RESULTS
A total number of 150 participants enrolled in the study, which comprised of 50 males and 100 females with a mean age of 25.8±5.14 years, while 50 refused to participate. The results show no significant association between the level of burden and quality of life. On the WHOQoL scale, 39% of the participants showed moderate to severe level of burden, 21% had mild to moderate burden while 19% had a level of severe burden.
CONCLUSIONS
Home-based therapy for stroke survivors has shown beneficial impact by implementing client-centred practice, however it also increases the burden on the caretakers and therapy service providers. The participants of the recent study have an average quality of life and an increased level of burden therefore, further studies are required to address the healthcare needs of therapists working in a home-based setting to improve health outcomes of both the therapist and the patient.
KEY WORDS
Quality of life (QOL), home-based, home care services, stroke, rehabilitation.
Maha Khan
Occupational Therapist
Ziauddin College of Rehabilitation Sciences
Ziauddin University
[email protected]
[Khan M. Association Of Level Of Burden And Quality Of Life Among Home-Based Therapists Of Stroke Survivors. Pak. j. rehabil. 2020;9(1):23-28]
This is an open-access article distributed under the terms of the Creative
Commons Attribution Licence (CC BY) 4.0 https://creativecommons.org/
Stroke is also known as cerebrovascular accident, which occurs due to an interruption of blood supply to brain. Globally, it is the leading cause of death and long-term disability. It lowers the survivor’s quality of life due to its poor health outcomes such as neurological co-morbidity, physical and cognitive impairments; this consequently increases economic burden on the family and community. The prevalence of a stroke is very high in Asian countries. Seventy per cent of global stroke burden is on low and middle-income countries. In the last decade, Stroke related mortality was found to be decreasing in East-Asian countries such as Japan and Korea. In South Asia, the minimum mortality rate of stroke in 2010 observed in Bangladesh (54.8/100, 00). Mortality rate in India and Pakistan is close to each other 82/100,000 and 83/100,000 respectively1. The risk factors of stroke include hypertension, diabetes mellitus; prolonged contraceptive use, dysthymias (atrial fibrillation, atrial flutter) rheumatic/valve heart disease, socioeconomic background, and health status. According to the current prevalence rate of stroke in Pakistan, hypertension is the most common risk factor2. It has been evident that stroke is the major cause of dysfunction in adults, the rate of stroke is high between 50 to 60 years of age thereby increases mortality ratio, resulting in an increased economic burden on society. Stroke is also a major cause of disability and poor quality of life in the elderly. It results in poor health outcomes such as prolonged hospital stay, reduced functional mobility and dependency for ADLs2-3.
Recent studies suggest that neuronal regeneration after stroke helps in spontaneous recovery. Immediate rehabilitation from a multidisciplinary team is linked with improved health outcomes. Post-stroke rehabilitation services by occupational therapists and physiotherapists are the keystone of treatment; the early rehabilitation intercessions have a more prominent advantage to the client4. Post-stroke rehabilitation is generally provided in four settings: inpatient rehabilitation facility, skilled nursing facility, outpatient facility and home-based rehab programmes. According to one study, patients who received rehabilitation services at home after stroke had lower depression rate as compared to those enrolled in rehabilitation at a hospital setting5. Furthermore, home-based rehabilitation is cost-effective and encourages active participation of caretakers. The multidisciplinary care in a home environment promotes client-centred intervention. Each professional in the team has its unique role. Physiotherapy is helpful in maintaining, developing movement and functional independence after a stroke6. Studies demonstrated a significant improvement in functional performance by implementing home- based occupation-focused activities and tasks in which cognitive, behavioural and environmental strategies were used7.
Previous researchers have identified a high amount of burden among caregivers of stroke survivors (with partial and complete disability), adversely affecting caregiver’s quality of life. Providing continuous care to a stoke survivor increases burden on the caretaker, which many times may manifest as fatigue, depression and irritable mood8, therefore home-based rehabilitation is needed to improve functionality of stroke survivors and reduce burden on the caretaker. Moreover, Longitudinal Analysis shows the quality of life of a person with CVA and their caretaker correlates with each other9. Further studies highlighted that home-based rehabilitation increases the quality of life, improves functional performance and reduces further risk of deterioration10-11. Also, home-based therapy reduces potential problems of transfer of learnt skills from training setting to home setting. A qualitative study conducted in 2000 by Sues Stephenson, fellows identified therapist, and patient view about home-based therapy. Patients highlighted two main benefits of home-based therapy: convenience and relevancy however, therapists posits difficulty in maintaining control during therapy sessions and increased burden affecting their quality of life.
World Health Organization defines quality of life as the perspective of an Individual of its life in relation to its culture, and value system in which they live to achieve their goals and meet expectations of the society. It is a broad concept that addresses ones physical health, psychological state, personal belief and relationship to its environment12. World Health Organization Quality of Life – BREF (WHOQoL) assesses quality of life in a variety of settings and population groups. The purpose to develop this assessment tool was to develop a questionnaire to assess quality of life cross-based on their perception to their personal goals, value system and culture. Many researchers have used WHOQoL along with Zarit Burden Interview, which is a caregiver self-report measure; to identify the impact of care giving to stroke survivors on the level of burden and quality of life.
Client-centred stroke rehabilitation at a home setting showed to significantly reduce disability and improve health outcomes of stroke survivors; however, studies have shown that it increases burden on caretaker and home-based therapists reducing their quality of life; which may impact the continuity of home-based therapy and quality care to patients. A study conducted in 2014 at Nigeria identified that the quality of life of caregivers and therapists inversely correlates to a caregiver’s burden, also the lower functioning of stroke survivors significantly associates with care giving burden13.
This research article focus on quality of life and level of burden on Physiotherapist and Occupational Therapist providing home based rehab care. The physiotherapist focus on restoration of body moments interrupted due to any injury or insult while Occupational Therapist works for improvement of functional skills and maximizing of independency in activities of daily living. The work nature of both the professionals is high physical and emotional demanding. It includes many manual tasks, carrying and lifting weight, repetitive tasks and providing emotional support to patient and their families. Due to lack of rehab equipment, therapist often takes awkward positions and postures which increase stress and strain on joints and muscles. The outcome of is work related musculoskeletal disorders and fatigue. These outcomes also impact the mental health of the therapist and work performance.
The purpose to conduct this study is to identify the relationship between level of burden and quality of life of therapist who provides home-based rehabilitation to the stroke patients. This will help to address the health related concerns of patient and therapist.
Study Design
Cross-sectional survey
Study Design
The study was conducted at various Rehabilitation Departments of primary and tertiary hospitals of Karachi including Dr. Ziauddin Hospital North Nazimabad and Clifton Branch, Liaquat National Hospital (LNH), Institute of Physical Medicine and Rehabilitation (IPMR).
Duration of Study
6 months.
Sampling Technique
Non-Probability Convenience Sampling Technique.
Target Population
Home-based therapists dealing with stroke.
Sample Size
The sample size was calculated by using EPI software14. A study conducted in the year 2018 entitled “The Epidemiology of Stroke in a Developing Country (Pakistan)” was used for calculating a sample size. By keeping the Confidence Interval of 95%, bound of error of 7%, a sample size n=147.
- Inclusion criteria
Physiotherapists and occupational therapists providing home-based rehabilitation services to stroke patients.
- Exclusion criteria
Therapists who do not provide home-based rehabilitation services in stroke rehabilitation or those who refuse to participate.
Data Collection Procedure
Data was collected from Rehabilitation Department of primary and tertiary hospitals of Karachi. Prior to the data collection, all participants were provided detailed information about the study and informed consent was obtained. Followed by the consent, participants were given the World Health Organization Quality of Life
(WHOQoL) and Zarit Burden Interview (ZBI) questionnaires to evaluate the amount of burden and its relation with their quality of life of home-based Rehabilitation Professionals (OT, PT) working with stroke patients
Data Collection Tool
Data was collected through two outcome measures: World Health Organization Quality of Life (WHOQoL) and Zarit Burden Interview (ZBI) questionnaires. The questionnaires were modified to research requirements. The WHOQOL-BREF is a commonly used questionnaire that consists of four domains (psychological health, environmental health, physical health and social relationships) 15. Higher domain score indicates higher quality of life. Mean score of all questions in each domain compute the domain score. Mean scores are then duplicated by four to make domain scores comparable by the scores utilised in WHOQOL-BREF.
Zarit Burden Interview (ZBI) is an effective and reliable tool for determining the burden that a person experiences in their current life situation16. Interviews are based upon 22 questions in which each question score is 0-4 points. According to the scoring key: 0 – 21 indicates little or no burden whereas, 21 – 40 indicates mild to moderate burden, but 41 – 60 means moderate to severe burden and 61 – 88 score is considered as severe level of burden.
Data Analysis Strategy
The statistical software named SPSS (Statistical Package for Social Sciences) was used find out the statistical tools and to analyse the data. Participant’s demographic details (including age and gender) were represented through descriptive statistics which includes tables of mean and standard deviation along with a graph i.e. histogram. Moreover, chi-square test of association used to indicate the association between the variables.
In this study the researcher provides detailed information about this particular topic and all the participants were provided detailed information about the research process and purpose. Moreover, the participants were also made aware with consent forms at the time of conducting research. The data was collected after obtaining informed consent from the participants and it is assured that all the information is highly confidential.
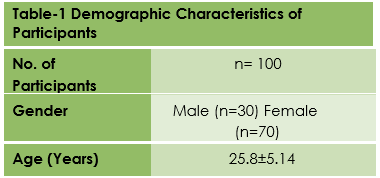
To conduct a detailed review and study on this kind of a topic, the researcher took a sample size of total 150 participants (50 males and 100 females) enrolled in the research while 50 generally refuse to participate; the mean age of participants was found to be 25.8±5.14 years respectively as shown in Table-1 which generally shows that the selected participants fall in between the age of 19 to 31 years.
To conduct a detailed review and study on this kind of a topic, the researcher took a sample size of total 150 participants (50 males and 100 females) enrolled in the research while 50 generally refuse to participate; the mean age of participants was found to be 25.8±5.14 years respectively as shown in Table-1 which generally shows that the selected participants fall in between the age of 19 to 31 years.
Findings of the study mostly shows that participants generally have a mean score of 65.89±16.7 (which essentially lies in the series of minimum value 48 and the maximum value of 81) in WHOQOL-BREF (Table-2). The descriptive statistics graph shows that 39% lies under moderate to severe burden, whereas, 21% specifically showed mild to moderate burden while 19% specifically had severe burden as shown in Figure-1. The value of Likelihood Ratio found 0.79 and the value of Pearson chi-square which mostly is also known as p value generally is 0.24. Both of these values show that there essentially is no statistically significant association found between level of burden and quality of life. (Table-2).
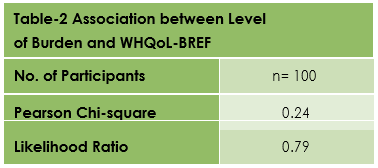

Figure-1 represents level of burden
The findings of the study revealed that the participants demonstrated slightly higher than average quality of life on the scale of WHO_QOL-BREF and on ZBI scale.
60% of the participant’s burden level falls into mild to severe level (39% moderate to severe burden, 21% mild to moderate) while 21% showed mild to moderate burden, and 19% had severe burden. However, no significant association was found between level of burden and quality of life. The scores of the present study are similar to the findings of a study conducted in 2016 on stroke survivors’ caregivers. The caregivers of stroke patients show average quality of life (62%) on WHO_QOL-BREF and moderate burden level (29%) on ZBI scale. Furthermore, this study also did not find significant association between quality of life and burden on the therapist17.
Many factors contribute to the burden on the therapist in a subtle way. Earlier studies specifically identifying the risk factor of physical stress faced by occupational and physiotherapist, consequently affecting the quality of life, really was a fairly physically challenging role, with excessive twisting and bending tasks, lifting, carrying and transferring generally heavy objects. Furthermore, in home-based therapy sessions, the therapist receives minimum assistance during the session as compared to hospital-based sessions. All of these factors increase physical burden on the therapist and affect their standard of living significantly18-19.
Similarly, a study conducted in Africa also reports that care-giving role to stroke patient is challenging which increases the physical and emotional burden on the caretaker affecting their quality of life. The study found that the caregiver experienced emotional distress and care giving strain20.
On the contrary, some studies do not found association between physical activity and health related outcomes of the therapist. A study conducted in Australia founded that the therapist had higher than average activity level in a week and only few of them complained for discomfort and pain21.
Many studies have identified a similar level of work burden on the therapist working with stroke patients in hospital and patient’s home22. According to a study, the participants (therapists) were satisfied with their work despite of moderate level of physical and psychological stress. This was due to moderate to high level of job control. The therapists were allowed to suggest and bring ergonomic improvements to reduce work-related stress,23 while burnout and emotional exhaustion in the therapist was found in settings where the therapist had a strict and tough routine and less job control24-25.
Many factors contribute to the quality of life and efficacy at work. Each individual experiences stress differently depending upon their personality traits and coping mechanism. There mode of living is comparatively different in all aspects from one another and that is why they carried out a stressful lifestyle. The workload, personality traits, coping mechanism, workplace environment and balance between work and family mediates the individual’s experience to stressful situations – all of which ultimately affects the quality of life.
The work nature of physiotherapists and occupational therapists increases the risk of musculoskeletal issues and weakness. Due to unavailability of rehabilitation equipment and support at client’s home, therapists have to adapt the awkward positions and postures that cause fatigue and pain. They usually get stressed having the patient go through too much exercise that can otherwise easily be done through equipment. Many workplaces have ergonomically altered to guarantee the specialist’s well-being, yet little consideration is paid on the well-being results coming about because of work worry of home-based rehabilitation services. This investigation has shed light on the level of workload and its effect on the well-being and prosperity of rehabilitation professionals providing home-based rehabilitation services.
This study statistically shows the weak association between quality of life and burden on therapist, proving home-based rehabilitation demonstrated moderate to high burden. Thus, researches are required to identify the factors influencing quality living of therapist in Pakistan.
The study was helpful to investigate the risk factor that promotes burden and reduces the quality of life of rehabilitation professionals. Moreover, this research could be supportive in reducing the amount of burden in order to enhance the quality of life. Furthermore, it also addresses the need of therapists as they are prone to injury due to the nature of their work.
It is concluded that the participants had an average quality of life and increased level of burden therefore, further studies are required to address the healthcare needs of therapists working in home-based settings to reduce the level of burden and increases quality of life.
- Venketasubramanian N, Yoon BW, Pandian J, Navarro JC. Stroke epidemiology in south, east, and south-east Asia: A review. Journal of stroke. 2017 ;19(3):286
- Khealani BA, Hameed B, Mapari UU. Stroke in Pakistan. Journal of the pakistan medical association. 2008;58(7):400. Morris, J.H., Oliver, T., Kroll, T., Joice, S. and
- Williams, B., 2015. From physical and functional to continuity with pre-stroke self and participa-tion in valued activities: A qualitative explora-tion of stroke survivors’, carers’ and physiother-apists’ perceptions of physical activity after stroke. Disability and rehabilitation, 37(1), pp.64-77.
- Hellweg S. Effectiveness of physiotherapy and occupational therapy after traumatic brain injury in the intensive care unit. Critical care research and practice. 2012 ;2012.
- Mayo NE. Stroke rehabilitation at home: lessons learned and ways forward. Stroke. 2016;47(6):1685-91..
- Memon AR, Sahibzada NM, Azim ME, Siddiqui FA. Physical therapy as a profession and its educational development in Pakistan. JPMA. The Journal of the Pakistan Medical Associa-tion. 2016 ;66(11):1472-4.
- Nielsen TL, Petersen KS, Nielsen CV, Strøm J, Ehlers MM, Bjerrum M. What are the short-term and long-term effects of occupation-focused and occupation-based occupational therapy in the home on older adults’ occupational performance? A systematic review. Scandina-vian journal of occupational therapy. 2017 ;24(4):235-48.
- Balhara YP, Verma R, Sharma S, Mathur S. A study of predictors of anxiety and depression among stroke patient–caregivers. Journal of Mid-life Health. 2012 ;3(1):31.Pucciarelli G, Vellone E, Savini S, Simeone S, Ausili D, Alvaro R, Lee CS, Lyons KS. Roles of changing physical function and caregiver burden on quality of life in stroke: A longitudinal dyadic analysis. Stroke. 2017 ;48(3):733-9.
- Pinedo S, SanMartin V, Zaldibar B, Miranda M, Tejada P, Erazo P, Lizarraga N, Aycart J, Gamio A, Gomez I, Bilbao A. Quality of life of stroke patients and their caregivers. Int J Phys Med Rehabil. 2017;5(386):2.
- Ng S, Chu M, Wu A, Cheung P. Effectiveness of home-based occupational therapy for early discharged patients with stroke. Hong Kong J. Occup. Ther.. 2005 ;15(1):27-36.
- Chaiyawat P, Kulkantrakorn K, Sritipsukho P. Effectiveness of home rehabilitation for ischemic stroke. Neurology international. 2009 ; 1(1).
- Su CT, Ng HS, Yang AL, Lin CY. Psychometric evaluation of the Short Form 36 Health Survey (SF-36) and the World Health Organization Quality of Life Scale Brief Version (WHO-
- QOL-BREF) for patients with schizophrenia. Psychological Assessment. 2014 (3):980. Ogunlana MO, Dada OO, Oyewo OS, Odole AC, Ogunsan MO. Quality of life and burden of informal caregivers of stroke survivors Hong Kong Physiother J2014; 32(1):6-12.
- Kevin M. Sullivan, R., 2018. Openepi – Toolkit Shell For Developing New Applications.
- Cheung YB, Yeo KK, Chong KJ, Khoo EY, Wee HL. Measurement equivalence of the English, Chinese and Malay versions of the World Health Organization quality of life (WHO-QOL-BREF) questionnaires. Health and quality of life outcomes. 2019 ;17(1):67.
- Yap P. Validity and reliability of the Zarit Burden Interview in assessing caregiving burden. Ann Acad Med Singapore. 2010; 39:758-63. Caro CC, Costa JD, Da Cruz DM. Burden and quality of life of family caregivers of stroke
- patients. Occupational therapy in health care. 2018 ; 32(2):154-71.
- Ntsiea MV. Current stroke rehabilitation services and physiotherapy research in South Africa. S Afr J Physiother2019;75(1).
- McPhail SM, Waite MC. Physical activity and health-related quality of life among physio-therapists: a cross sectional survey in an Austra-lian hospital and health service. J Occup Med Toxicol 2014;9(1):1.
- Badaru UM, Ogwumike OO, Adeniyi AF, Nelson EE. Determinants of caregiving burden and quality of life of informal caregivers of African stroke survivors: literature review. nt J Disabil Hum Dev. 2017;16(3):249-58.
- McPhail SM, Waite MC. Physical activity and health-related quality of life among physio-therapists: a cross sectional survey in an Austra-lian hospital and health service J Occup Med Toxicol. 2014;9(1):1.
- Lindsay R, Hanson L, Taylor M, McBurney H. Workplace stressors experienced by physio-therapists working in regional public hospitals. Aust J Rural Health2008 ;16(4):194-200.
- Muaidi QI, Shanb AA. Effects of work demands on physical therapists in the KSA. J Taibah Univ Sci. 2016;11(1):56-62.
- Rogan S, Verhavert Y, Zinzen E, Rey F, Scherer A, Luijckx E. Risk factor and symptoms of burn-out in physiotherapists in the canton of Bern. Archives of Physiotherapy. 2019;9(1):1-5.
- Nerdrum P, Rust en T, Helge R nnestad M. Psychological distress among nursing, physio-therapy and occupational therapy students: A longitudinal and predictive study. Scand. J. Educ. Res.2009;53(4):363-78.