
ABSTRACT
Bell’s palsy is a prevalent type of Facial nerve Palsy, estimated up to 75% of the cases. A 58 year old male patient presented with right sided Bell’s palsy. Thorough examination revealed the weakness of facial musculature and synkinesis associated with drooping and asymmetry. Reportedly, he had difficulty in eye closure, chewing and drinking. Assessment was conducted using Sunny Brook Facial Grading Scale. After assessment a comprehensive strategy combin-ing of different modalities including electrical stimulation with Russian Current, gentle soft tissue mobilization, resistance exercises and taping. Symptomatically, after 3 weeks there was a significant improvement in the facial symmetry, strength and function of facial musculature as well as score of Sunny Brook Facial Grading Scale. Experimentally, this indicates effectiveness of this treatment regime, however; further randomized control trials should be conducted to further investigate efficacy and validity of this combination approach.
KEYWORDS
Facial Neuropathy, Inflammatory, Acute Facial Paralysis, Idiopathic, Facial Paralyses, Paralysis, Idiopathic Facial, Inflammatory Facial Neuropathy.
Sagar Kumar
Physiotherapist
Departmental of Rehabilitation Sciences Ziauddin Hospital, Clifton [email protected]
Muhammad Ather Hashmi
Lecturer
Ziauddin College of Rehabilitation Sciences
Ziauddin University
[Kumar S. Hashmi MA, Multilpe approaches in management of Bell’s palsy; a case study. Pak. j. rehabil. 2018; 7(2): 52-54]
Bell’s palsy is characterized as the most prevalently Bell’s palsy is characterized as the most prevalently occurring type of facial nerve palsy/paralysis that is reported to be 75% of the cases1. Generally, Bell’s palsy is characterized as an idiopathic disorder2. However, literature also suggests reactivation of herpes simplex virus of having significant role in acute onset of this acute facial paralysis (Bell’s palsy) by causing inflammation, entrapment and sufferance of Facial Nerve in narrow labyrinthine portion of fallopian canal1. Consequently, Bell’s palsy presents with half-face paralysis manifesting certain typical symptoms including pain, synkinesis, facial dysethesia, numbness, hyperacusis, drooling, epiphora, incomplete eye closure and absence of facial creases and naso-labial folds3. Furthermore, the recovery of the symptoms varies depending upon the severity of the case that may last from 2 weeks up to 6 months4. The most affected aspect is loss of emotional marking, facial synchrony and symmetry that may also involve dropping a lip corner causing drooling and difficulty in drinking or rinsing the mouth5.
As a matter of fact, there are diversified approach-es of treatment being practiced globally for the management of facial paralysis or Bell’s palsy. Med-ically, administration of corticosteroids and other pharmaceutical agents is used while physical thera-py interventions include Electrical neural stimulation (by means of various therapeutic currents), massage, facial exercises, Kinesio taping and Kabat1,2,3,6. Interestingly, all the treatment regimens possess supporting liturgical evidences; however, the quality of evidence may vary. The current case study highlight the impact of combina-tion regime that account for the application of different modalities incorporated into a productive treatment protocol for Bell’s palsy patients.
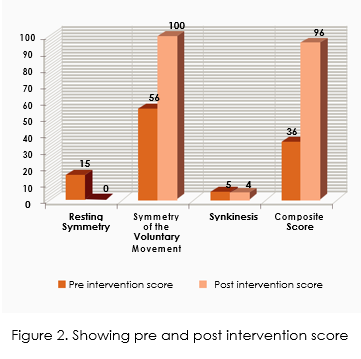
A 58 years old male experienced a sudden onset of right sided facial paralysis as a consequence of Bell’s palsy. He noticed alteration in the muscles strength while performing facial expression and in symmetry of facial markings while observing these in mirror. He reported to a well-known neuro-physician of the metropolis who diagnosed it as Bell’s palsy and after medicinal management referred him to the physical therapy department of a renowned tertiary care hospital. On examination it was that right side of the patient’s face was affected with moderate to severe degree of weakness and synki-nesis. Moreover, he was unable to close his right eye and due to dropped right corner of lips he was facing difficulty in drinking. The overall degree of severity of facial paralysis was assessed according to Sunnybrook Facial Grading System, whilst the composite score was 36.
Primarily, electrical stimulation using Russian current was applied on five distinct motor points of the affected side of patient’s face as demonstrated in figure 1. For each point, duration of stimulation was 3 minutes. Intensity was kept 5 mA with surging of 1, 10, 0, 3 for ramp-up, stay, ramp-down and delayed respectively. Furthermore, facial muscles were facili-tated using gentle soft tissue mobilization with tips of the fingers in cranial direction. The number of strokes ranges between 12 and 15 strokes in each set. Adding to this, resistive exercises were performed for all facial expression including eye opening and closure, eye brow lifting, smiling, teeth clinching, pouting and blowing. The resistance was provided by the therapist using his hand. In the culmination of treatment, affected side was provided with taping with surgical tape in order to enhance neuromuscu-lar facilitation, which the patient was instructed to remove after 4 hours. The method of application consist of 3 cm broad,two long tape stripes, stretched from intermandibular joint to temporo-mandibular joint lifting the drooping muscles of that side parallel to the jaw line while two short stripes with the same width anchoring the previous stripes at both ends.
The treatment protocol was continued for 3 weeks while the patient was instructed to repeat the facial exercises using mirror at home, daily
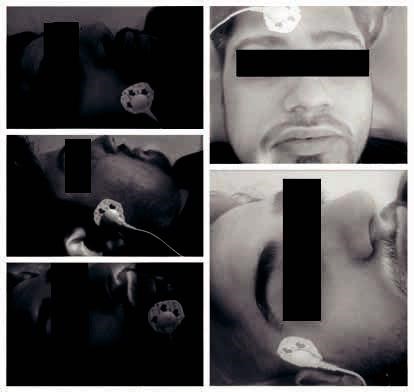
Figure 1. Showing the placement of electrodes for electrical stimulation
After three weeks, on visual observation facial symmetry was improved along with muscle strength and tone. Patient, satisfactorily, reported ease in chewing food and drinking fluids without drooling Upon reassessment through Sunnybrook Facial Grading System the composite score was found to be 96 which is illustrated in figure 2. Patient could not continue the treatment further in due to return-ing back to his hometown. However, this was a very quick recovery that may be considered as the consequence of this combination of treatment modalities and option.
The case report highlights the importance of incor-porating diverse means of treatment which has demonstrated better results in this case. Moreover, Sunny Brook Facial Grading Score had improved more frequently. Conversely, a recently published study investigated the effectiveness of tailored facial therapy protocol on facial palsy, comparing it with Botox and revealed better results with conclu-sion that prolong duration of treatment is directly proportional to the increase in Sunny Brook Score7. Therefore, it can be deduced that the combination approach has more profound impact despite a single tailored facial therapy or electrical stimula-tion distinctly as a review conducted by Fargheret. al failed to conclude availability of high quality evidences efficacy of electrical stimulation on facial palsy alone8. However, this does not exclude the possibility that treatment intervention was given during the acute phase of onset of symptoms that is also suggestive of frequent neuroplasticity by the literature9. Another study examined the effects of Low-Level-Laser therapy in combination with exercise while comparing it with the facial exercises alone and found better outcomes for the prior one suggesting that there are modalities too, to be incorporated in to the treatment regime and exam-ining its efficacy10.
This case report revealed that the combination therapy to be more efficient and potent in speedily improvement of Bell’s palsy symptoms. However, there is a need of randomized controlled trial to be conducted for the validity of this treatment regime.
- Monini S, Lacolucci CM, Triglia MD, Lazzario AI, Barbara M. Role of Kabat Rehabilitation in facial nerve palsy; a randomized study on severe case of Bell’s palsy. ActaOtorhinolaryngol Ital. 2016;36(1):282-288
- Shamsi S. Effect of physiotherapy in manage-ment of facial palsy- case study. Int J Health Sci Res. 2015; 5(1):408-412.
- Ghous M, Yaqoob I, Kanwal M, Malik AN. Effects of Kabat rehabilitation verses taping to reduce facial disability and synkinesis in Bell’s palsy. RMJ.2018;43(3); 543-546
- Badshah M, Umar M, Naeem A, Marryam M. A randomized control trial to review the effective-ness of combination therapy versus steroids alone, for the treatment of Bell’s palsy. Ann Pak Inst Med Sci 2013;9(3):118–21.
- Ng SY, Rothschild D. The Use of Phototherapy for Bell’s palsy in Facial Nerve.2018 Nov 5. IntechOpen.
- Mridha C, Thakre PI. Role of Kabat technique along with conventional physiotherapy treat-ment versus conventional physiotherapy alone in Bell’s palsy patients. Indian J. Res. 2018;7(6):23-25
- Watson GJ, Glover S, Allen S, Irving RM. Outcome of facial physiotherapy in patients with prolonged idiopathic facial palsy. “J Laryn-gol Otol. 2015; 129(1):348-352
- Fargher KA & Coulson SE. Effectiveness of electrical stimulation of for rehabilitation of facial nerve paralysis. Physical therapy reviews. 2017;22( 3): 169- 176
- Song W, Dai M, Xuan L, Cao Z, Zhou S, Lang C et. al. Sensorimotor cortical neuroplasticity in the early stage of Bell’s Palsy. 2017; 2017(1)
- Ordahan B, Karahan AY. Role of low-level laser therapy added to facial expression exercises in patients with idiopathic facial (Bell’s) Palsy. Lasers Med Sci. 2017;32(4):931-6