
ABSTRACT
BACKGROUND AND AIM
Hip and knee OA has been ranked as eleventh maximum contributor to global incapacity. The prevalence is expected to increase up to 25.9% by 2040. Hip arthritis reduces the mobility at the hip joint limiting flexion extension, abduction, and adduction, internal and external rotation. Similarly knee pain causes considerable disability among middle adult population affecting both proximal and distal joint (hip and ankle) respectively. Hence the present study aims to find out a correlation between Hip Rotation Dysfunction and Knee Pain.
METHODOLOGY
A cross sectional study was conducted on patient with hip and knee pain of age in between 45 to 60 years. Ranges at the level of hip joints were assessed using goniometer. Knee pain was assessed using Visual Analog Scale.
RESULT
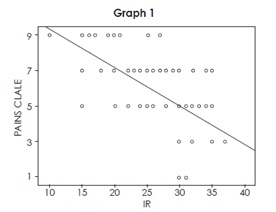
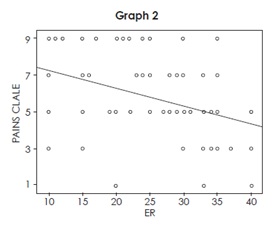
The result obtained from the study shows a moderate negative correlation between knee pain and hip internal rotation, r= -0.67 showing no significant correlation p=0.45. There is also a weak negative correlation between knee pain and hip external rotation, r= -0.37 with a p> 0.05.
CONCLUSION
The result obtained from the study concluded that no significant co-relationship exist between hip rotation dysfunction and knee pain, however more researches with larger number of sample size is required to further evaluate the causal relationship between the two variables.
KEYWORDS
Hip rotation, Correlation, dysfunction, knee pain, VAS, Prevalence.
Batool Hassan
Physiotherapist
Sindh Govt. Hospital
Anum Haidar
Physiotherapist
Memon Medical Centre
Nida Kanwal
Physiotherapist
Maa Ayesha Clinic
Mehak Yaseen
Physiotherapist
Chiniot General Hospital
[Hassan B, Haidar A, Kanwal N, Yaseen M. Correlation between Hip Rotation Dysfunction and Knee Pain. Pak. j. rehabil. 2017;6(2):32-37]
INTRODUCTION
Hip and knee OA has been ranked as eleventh maximum contributor to global incapacity and 38th maximum in incapacity Adjusted Life Years out of 291 conditions globally. Prevalence is seen higher in females than guys. Handicap for hip and knee extended from 10.5 million to 17.5 Million from 1990 to 20101. A research has been conducted in 2011 which revealed that around the world, osteoarthritis (OA) is presently evaluated to be the fourth driving reason for inability. The greater part of this inability trouble is inferable from the contribution of the hips or the knees2.
An expected 52.5 million (22.7%) grown-ups in the United States have joint inflammation. Of those, 22.7 million (9.8% of U.S. grown-ups) have joint inflammation inferable action impediment according to Morbidity and Mortality Weekly Report 2016. The prevalence of arthritis is projected to increase 78.4 million (25.9% of U.S. adults) by 2040, and the number of adults with AAAL is projected to increase to 34.6 million (11.4% of U.S. adults).
Knee and hip osteoarthritis are profoundly common infections in the more established population. The estimation for hip substitution is by all accounts altogether higher than that for knee substitution. Out of 11,002 individuals, the assessed suitability rate for hip substitution seems 37.7% in men and 52.7% in women with osteoarthritis. The evaluated propriety rate for knee substitution seems 11.8% in men and 17.9% in women with osteoarthritis3.
Degenerative deformities at the joint leads to structural and functional limitations at the joint limiting its physiological movements.
Radiographic signs of Femoral acetabular impingement in asymptomatic adults with age in between 40 and 60 years shows increase in alpha angle is related to decrease internal rotation of hip joint leading to painful hip joint which may affect it’s proximal and distal joint (Sacroiliac and Knee) respectively4.
According to the American Academy of Orthopedic Surgeons knee pain is a common condition resulting in 19.4 million pain-related visits to a physician each year. This number is significantly higher than low back pain (5.9 million visits), hip pain (3.2 million visits), and ankle pain (1.9 million visits). Knee pain impairs function, which can lead to disability5. This condition is profoundly pervasive in more seasoned people and is viewed as an essential determinant of general wellbeing status in maturity6. Agony in weight bearing joints might be because of various causes, including alluded or emanated torment, sciatica, delicate tissue malady. In any case, confirm is developing that personal satisfaction and incapacity in OA are more identified with indications than to radiological seriousness7. Hip arthritis reduces the mobility at the hip joint limiting flexion extension, abduction, andadduction, internal and external rotation. Similarly knee pain causes considerable disability among middle adult population affecting both proximal and distal joint (hip and ankle) respectively. Patients with osteoarthritis are at higher danger of death contrasted and the all-inclusive community. History of diabetes, tumor, or cardiovascular infection and the nearness of strolling incapacity are real hazard factors. Administration of patients with osteoarthritis and strolling inability should concentrate on compelling treatment of cardiovascular hazard variables and comorbidities, and also on expanding physical action8.
If we need to examine a patient with complain of pain in knee joint, it is not completed without examining adjacent joint, hip and ankle, respectively9. There is a connection between power and position of hip joint and Patellofemoral Joint Stress (PFJS)10. It is revealed by a study that strengthening of hip abductor muscles was very much productive in mounting muscle power and diminishing pain in patients with Patellofemaoral Pain Syndrome (PFPS)11.
The problem in the proximal (hip) joint can affect distal (tibiofemoral and patellofemoral) joint mechanics12. Hip strength is very much significant. It is concluded that any movement at hip joint whether flexion, extension, rotation, poor motor control at the hip often manifests itself in knee pain13. Severe knee osteoarthritis is a strong cause of hip and knee pain14.
Loose or weak pelvis may contribute to knee injury. A strong upper leg strength can be beneficial in preventing knee injury15.The result of a study suggested that there is a strong relation between a weak hip and knee pain thus indicating a strong hip joint has a positive impact on distal knee joint and a weak hip joint may contribute to weaken the knee joint16. Periodic dislocation is seen in quite a few patients which give may arise to knee complications17. So the knee pain may have a direct or indirect relation with faulty biomechanics at hip and ankle joint18.
METHODOLOGY
Participants
Patients between age 45 to 60 years including both male and female.
Research Design
Cross sectional study design.
Study Setting
The research was conducted in Out Patient Department of Jinnah Hospital, Alamgir Health Care Center, Memon Medical Institute, Sindh Government Hospital.
Study Duration
6-8 months.
Sample Size
Sample size was calculated using WHO software for sample size calculation. The study conducted in 2010 title as “epidemiology of osteoarthritis” was taken to calculate the sample size. By taking the prevalence of hip OA 27%, keeping confidence Interval 95% and 8% bound of error; a sample size of 115 was calculated.
Sampling Method
Subjects were allocated to study groups using convenient sampling method.
Inclusion Criteria
- The vast majority of the consideration criteria
utilized were the understanding, capacity and readiness to partake in the outpatient technique19.
- Ranging from 45 to 80 years20.
- Patients with both hip and knee pain
- Not taking any drug during the inclusion period which could perturb walking (for example neuroleptics)
- No limitation for strolling or light physical activity Exclusion Criteria
- Sign and symptoms of depression
- Any trauma and history of fall
- Grade 3 obese patients with BMI (>40kg/m2) will be excluded21.
- Patients with cardiovascular (e.g. heart disappointment, history of myocardial dead tissue, arrhythmia), pneumonic (e.g. embolism, respiratory disappointment) and inadequately controlled comorbidities will be prohibited22.
- Systemic problems
- Open wounds
- External fixators
Data collection procedure
All the subjects were recruited with knee pain; detailed hip assessment by a senior therapist was done. All ranges were assessed using goniometer and pain on the knee will be assessed using VAS.
Data Analysis
Analysis was performed by the researcher using computer analysis software SPSS Version 21. Descriptive data for the average of the three measurements VAS, IR and ER included means and standard deviations. The Pearson’s correlation coefficient was used to analyze the associations between hip and knee and to compare the pain of knee joint with hip
rotation dysfunction. In order to adjust for possible inflation of the (P > 0.05) alpha level due to multiple t-tests.
Outcome Measures
The visual analogue scale is a measurement tool which was used to assess intensity of pain which provides 0- 10 score in which higher score indicates high intensity of pain. VAS recommended score as no pain (0), mild pain (1 to 4), moderate pain (5 to 7) and severe pain (8 to 10). Another measurement instrument is goniometer which is used to measure ranges at hip joint.
RESULT
The study includes 100 participants with a mean age of 53.25. The male and female participants included in this study is shown in figure 1.
In the following table 1, the means and standard deviations of participants’ age s shown and gender distribution of participant. There were in total 100 participants in this research study were included. The demographics show that there was mean age 50 years. There were 24 % male and 66% female among participants.
| Table1. Percentage distribution of demographic characteristics of knee pain patients | ||
| Demographic characteristics | n | % |
| Age (Mean±SD) years | 53.25±4.5 | |
| Gender | ||
| Male | 24 | 24 |
| Female | 66 | 66
|
With pain scale 4 mean IR=30.67 and ER=36, at pain scale 5 mean IR=32.88 and ER=34.52, at pain level 6 mean IR=27.77 and ER=30.06, at 7 mean IR=24.93 and ER=28.24 and at pain scale 8 mean IR=17.33 and ER=25 was found as shown in Figure 2.
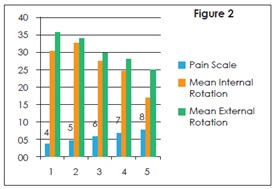
Mean value for pain scale was 6.40 with the average IR found to be 26.21 and ER 29.64 of the given sample with the SD 6.49 and 8.03 respectively as shown in Table 2.
| Table 2: Descriptive Statistics Of Pain Intensity (Vas), Internal Rotation And External Rotation (N=100) | ||
| Variable | Mean | Std. Deviation |
| VAS | 6.40 | 1.03 |
| IR | 26.21 | 6.49 |
| ER | 29.64 | 6.49 |
There is a moderate negative correlation between knee pain and hip internal rotation, r= -0.67, p=0.45. There is also a weak negative correlation between knee pain and hip external rotation, r= -0.37, p= 0.13.
| Table 3: Correlation Between Pain Intensity And Internal Rotation, Pain Intensity And External Rotation (N=100) | ||
| Variable | Pearson Correlation | P-Value |
| VAS+IR | -0.674 | 0.45 |
| VAS+ER | -0.373 | 0.13 |
Correlation is significant at the 0.01 level (2-tailed).
DISCUSSION
The purposes of this study were to determine whether there are differences in lower-extremity kinematics and to examine the relationship between hip Rotation and knee pain. Correlation between hip rotation dysfunction and knee pain has been checked on patients who have pain in knee for more than 3 months. Results shows that patients who have severe pain have decrease internal rotation at hip joint as compare to the patients who have moderate pain. External rotation is also reduced to some extent but we don’t see any direct effect of knee joint pain on external rotation. As our interpretation of research there would be change in ranges depending on whether pain is moderate or severe.
There were no gender differences (P>0.05), which may be driven by the low subject numbers; however, due to the lack of gender differences, the correlational analyses were performed without regard to gender. Also, due to the moderate r-values reported for our significant findings, the results do not appear to be influenced by the low subject number.
Previous studies show a strong connection between hip and knee joint dysfunction that a faulty knee joint mechanics may influence hip joint function. According to Erik, When adduction or internal rotation increases at hip joint, it increases the Q angle by increasing the relative valgus of the lower limb, thus pressure on the patellofemoral joint increases due to peal lateral contact23.
According to Gibson, pain and age of patient had inverse relation, younger patients report higher pain. Age difference in pain score have been reported but the cause of difference is not certain and questionable24. Herr believe that older adults are not familiar with pain, cultural factor like stoicism results in under reporting of pain in older adults. Suggest that cultural factors, such as stoicism, lack of familiarity with verbal pain descriptors and the practice of pain reporting, may result in under-reporting of pain among older adults25. Recently LaChapelle found that increasing age is related to decreased pain severity and the perception of greater control over pain. The literature suggests that under-reporting of pain by the older adult cohort may be commonplace and that older patients may perceive greater pain control and thus lower pain severity26.
For the future studies, check range and pain scale before and after treatment to see whether ranges are consistent or increases as pain decreases after the treatment. Age group of patients should be specific.
CONCLUSION
VAS for knee pain is not a reliable tool to extract the exact condition of knee joint pain at that particular time and unequal numbers of males and females and low number of subjects who participated in this investigation were the limitations of the study. To ensure the correlational analyses were not influenced by gender, separate one‐way analyses of variance were performed to determine if there were significant differences between males and females for all variables of interest A final limitation of this investigation was the range of motion limits and positioning utilized for assessing Rotation of the hip joint.
REFERENCES
[1] Cross M, Smith E, Hoy D, Nolte S, Ackerman I, Fransen M et al. The global burden of hip and knee osteoarthritis: estimates from the global burden of disease 2010 study. Ann Rheum Dis.
2014;73(7):1323-30
[2]Ganasegeran K, Menke JM, Ramaswamy C, Murthy V, Abdul Manaf R, Alabsi AM, Al-Dubai SA. Level and determinants of knowledge of symptomatic knee osteoarthritis among railway workers in Malaysia. BioMed research international. 2014
[3] Quintana JM, Arostegui I, Escobar A, Azkarate J, Goenaga JI, Lafuente I. Prevalence of knee and hip osteoarthritis and the appropriateness of joint replacement in an older population. Arch Intern Med. 2008;168(14):1576-84
[4] Diesel CV, Ribeiro TA, Scheidt RB, de Souza Macedo CA, Galia CR. The prevalence of femoroacetabular impingement in radiographs of asymptomatic subjects: a cross-sectional study. Hip Int. 2015;25:258-63
[5] Peat G, McCarney R, Croft P. Knee pain and osteoarthritis in older adults: a review of community burden and current use of primary health care. Ann Rheum Dis. 2001;60(2):91-7
[6] Dawson J, Linsell L, Zondervan K, Rose P, Randall T, Carr A, Fitzpatrick R. Epidemiology of hip and knee pain and its impact on overall health status in older adults. Rheumatology. 2004 ;43(4):497-504
[7] Salaffi F, Carotti M, Grassi W. Health-related quality of life in patients with hip or knee osteoarthritis: comparison of generic and disease-specific instruments. Clin rheumatol. 2005;24(1):29-37
[8] Nüesch E, Dieppe P, Reichenbach S, Williams S, Iff S, Jüni P. All cause and disease specific mortality in patients with knee or hip osteoarthritis: population based cohort study. BMJ. 2011;342:d1165
[9] Yilmaz AE, Atalar H, Tag T, Bilici M, Kara S. Knee joint pain may be an indicator for a hip joint problem in children: a case report. The Malaysian journal of medical sciences: Malays J Med
Sci. 2011;18(1):79
[10] Meira EP, Brumitt J. Influence of the hip on patients with patellofemoral pain syndrome: a systematic review. Sports Health. 2011;3(5):455-65
[11] Ferber R, Kendall KD, Farr L. Changes in knee biomechanics after a hip-abductor strengthening protocol for runners with patellofemoral pain syndrome. J Athl Train. 2011 ;46(2):142-9
[12] Powers CM. The influence of abnormal hip mechanics on knee injury: a biomechanical perspective. J Orthop Sports Phys Ther. 2010;40(2):42-51
[13] Van Dillen LR, Bloom NJ, Gombatto SP, Susco TM. Hip rotation range of motion in people with and without low back pain who participate in rotation-related sports. Phys Ther Sport. 2008;9(2):72-81.
[14] Zeni JA, Rudolph K, Higginson JS. Alterations in quadriceps and hamstrings coordination in persons with medial compartment knee osteoarthritis. J Electromyogr Kinesiol. 2010;20(1):148-54
[15] Bennell KL, Hunt MA, Wrigle TV, Hunter DJ, Hinman RS. The effects of hip muscle strengthening on knee load, pain, and function in people with knee osteoarthritis: a protocol for a randomized, single-blind controlled trial. BMC Musculoskelet Disord. 2007;8:121
[16] Rowe J, Shafer L, Kelley K, West N, Dunning T, Smith R et al. Hip strength and knee pain in females. North American journal of sports physical therapy: N Am J Sports Phys Ther. 2007;2(3):164-169
[17] Masaoka T, Yamamoto K, Shishido T, Katori Y, Mizoue T, Shirasu H, Nunoda D. Study of hip joint dislocation after total hip arthroplasty. Int Orthop. 2006;30(1):26-30
[18] Cookson L. Atypical knee pain: the biomechanical and neurological relationship between the pelvis, hip and knee—a case report. Clin Chiropr. 2003;6(2):63-66
[19] Aynardi M, Post Z, Ong A, Orozco F, Sukin DC. Outpatient surgery as a means of cost reduction in total hip arthroplasty: a case-control study. HSS J. 2014;10(3):252-5
[20] Berger RA, Kusuma SK, Sanders SA, Thill ES, Sporer SM. The feasibility and perioperative complications of outpatient knee arthroplasty. Clin Orthop Relat Res. 2009;467(6):1443-9
[21] Berger RA, Sanders SA, Thill ES, Sporer SM, Della Valle C. Newer anesthesia and rehabilitation protocols enable outpatient hip replacement in selected patients. Clin Orthop Relat Res.
2009;467(6):1424-30
[22] Gondusky JS, Choi L, Khalaf N, Patel J, Barnett S, Gorab R. Day of surgery discharge after unicompartmental knee arthroplasty: an effective perioperative pathway. J Arthroplasty. 2014;29(3):516-519
[23] Hewett TE, Myer GD, Ford KR, Heidt Jr RS, Colosimo AJ, McLean SG et al. Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: a prospective study. Am J Sports Med. 2005;33(4):492-501
[24] Gibson SJ, Helme RD. Age-related differences in pain perception and report. Clin Geriatr Med. 2001;17(3):433-56
[25] Herr KA, Mobily PR. Complexities of pain assessment in the elderly clinical considerations. J Gerontol Nurs. 1991;17(4):12-9.
[26] Roth ML, Tripp DA, Harrison MH, Sullivan M, Carson P. Demographic and psychosocial predictors of acute perioperative pain for total knee arthroplasty. Pain Res Manage. 2007;12(3):185-94.
Urooj Khan
Lecturer
Dow IPM&R
Sana Kayenat
Physiotherapist
ACELP
Khadija Usman
Physiotherapist
ACELP
Vinesh Kumar
Physiotherapist
Aga Khan University Hospital
[Khan U, Kayenat S, Usman K,
Kumar V. Correlation Between LBP
and Rectus Abdominis Muscle
Weakness Using Kendall’s Grading
Scale. Pak. j. rehabil.
2017;6(2):38-44]
INTRODUCTION
Back pain considers expensive disease in modernsociety1. It is job related complaint2. Most people experience low back pain (LBP) at some point throughout their life span3. In United States, the economic burden of disease ranges from 84 to 624 dollars per year4. The prevalence has been reported from 6% to 19% for a first episode and recurrence achieves up to 50% over a 5 years’ stage5. In the Western countries, back pain lifetime prevalence is 60%–80% among adult population6. The incidence increases with age and is more prevalent between 30 to 50 years, thus associated with increased health care expenditures around the world7. The prevalence of back pain in Bangladesh is 64.8%, in India is 19.8%, in Nepal is 69.5%, in Pakistan is 40.6% and in Sri Lanka is 36.2%6. The general prevalence is higher in females (48%) than in males (32%)8.
Low back pain is defined as a pain or discomfort located below the margin of the 12th rib and above the inferior gluteal fold, with or without leg pain9. Back pain can be classified into acute (less than six weeks), subacute (6 to 12 weeks) or chronic (longer than 12 weeks)4. Faulty posture and biomechanics amendment are precursor to low back pain development10. Faulty posture is often associated with weak abdominal muscle11. Dysfunction of abdominal musculature (internal oblique and rectus abdominis) is one of the major causes of chronic low back pain (CLBP). The muscles of abdomen averagely enhanced activation by 1–3% and the extensors enhanced by 13–31%, due to increased load in CLBP12. Rectus abdominis (RA) eccentric activity is crucial to support the trunk and evade too much spinal strain and back pain13.
Diastasis recti abdominis (DRA) is an injury measured by a midline parting of the 2 rectus abdominis, this decrease strength of rectus abdominis. DRA occur 30% to 70% in pregnant women. DRA also seen in males. Condition is the consideration to be related with growing age, hereditary weakness of the abdominal muscles, weight lifting, weight fluctuations, performing full sit-ups, intermittent or chronic abdominal distention, and actions that may stimulate immense intra-abdominal pressure14. Kendall’s Abdominal Strength test is a standard method to assess abdominal strength in physical therapy15.
In Kendall’s abdominal strength test subjects lie supine on a firm surface with arms folded across the chest; a tester assists in raising the legs up to a vertical position, keeping the knees straight, then perform a posterior pelvic tilt and maintain this position while slowly lowering the legs to horizontal, strength is graded on the ability to keep the low back flat on the surface, the angle at which the back arches is noted and correlated with Kendall’s grading system15.
The rationale of this study is to find prevalence or contribution of rectus abdominis weakness in back pain patients. This study will contribute to decreasing the incidence of preventable impairments in population. The purpose of rectus abdominis weakness tests in backache patients is to find strength of rectus abdominis in back pain patients. It will determine is rectus abdominis weakness could be cause of back pain.
Deenika conducted systemic review in which eight studies were included. All the studies incorporated abdominal/core strengthening muscle exercises. The study resulted that exercises done during antenatal period reduced DRAM by 35%16.
A study on Effects of Basic Strength and Pelvic training on high school cross-country race times. He performed four standardized isometric strength test at hip adductors, abductors, extensors and core musculature for six weeks. He concluded that there was no interaction regarding increasing muscle strength and decreasing race times. Pelvic and core stability strengthening program routine trice a week could decrease in race times17.
A study conducted on finding out the occurrence of diastasis of rectus abdominal muscles instantly postpartum, having an outcome with the high occurrence of DARM (68%) on top of the umbilicus. A DARM of above 2.5cm is measured unsafe as it may hinder with the muscles of abdomen capability to stabilize the trunk, deprived lumbar stabilization may influence the person to the increase the development of back pain18.
Greta conducted the pilot study on 63 children and concluded that there is increased incidence of low back pain that has been related with Lumbar lordosis, especially in women. The posture stretches and weakens the abdominals (rectus abdominis, external and internal oblique) while shortening the hip flexors and lumbar extensors imbalance increases the stress to the low back, resulting in pain. He conducted Kendall’s lower abdominal and Kendall’s upper abdominal test to check the strength of rectus abdominis muscle. He concluded that strengthening exercises of rectus abdominis could delay back pain15.
Patricia, concluded in his article about Risk factors and occurrence of diastasis recti abdominis from late pregnancy to 6 months postpartum and a relationship with lumbo-pelvic pain, that diastasis recti abdominis is not linked with lumbo–pelvic pain14.
Study naming Correlation of low back pain and diastasis rectus abdominis in post-menopausal women between the age group of 50-60 years, resulted that there was a partial positive correlation between diastasis of abdominis and Low back pain in post-menopausal women. They used VAS and Roland Morris questionnaire for disability and pain and assessed for diastasis recti abdominis using diastasis recti test19.
Chiarello in their study Consequences of exercise regime on DRA in pregnant women resulted that about ninety percent of women who were not habitual of doing exercise or did not follow exercise regime had DRA and remaining who did exercise had only conditions. It was concluded that size and prevalence of DRA was more in non-exercising group than in exercising group of women20.
Chiarello conducted another research to compare inter rectus distance of pregnant women with pelvic girdle pain with these of other types of pregnancy related back pain, resulting in with inter rectus distance seen widest at umbilicus, narrowest below the umbilicus and decrease with a curl up, and showed no significant difference in the IRD of pregnant women with pelvic girdle pain21.
Monica conducted a multiple-baseline, single subject experimental design research on 16 women with lumbar pelvic pain after delivery and stated reduced pain and disability after an individually adjusted exercise intervention in women with post-delivery lumbar pelvic pain22.
Gerard conducted a study on functional therapeutic and core strengthening which postulated that athlete’s core strength, endurance, coordination flexibility and balance has the role in optimal sports performance, As of medical literature support core stability as a prevention of injury. So, exercises that promote neuromuscular re-educate in athletes with core dysfunction are crucial to preventing and treating injury23.
Any pain or discomfort occurring in the low back region presently or a previous episode with a duration greater than 3 days within the last year that essential prolonged rest or medical consideration.
Low back pain usually arises in the region of lumbar, thoracolumbar, or lumbosacral. Back pain mostly effects working population. Back pain is Associated with many symptoms and functional limitations. It may be due to any soft tissue injury of the trunk including weakness or spasm or it occurs when the core muscle which is responsible for stabilization of lumbar region is weak2.
METHODOLOGY
142 Participants was recruited in our study. Participants signed consent form. Questionnaires were filled by researcher after perform Kendell test.
Study Design
Study design was cross sectional study and information was collected using questionnaire.
Study Population
Men and women aged between 20 -40 years having back pain since 3 months.
Inclusion Criteria2
- Both gender male and female
- Age 20-40
- Having back pain
Exclusion Criteria13
- Pregnancy
- Spinal cord injuries.
- Neurological diseased
- Spondylosis
Red flag for back pain:
- Circulatory problems
- Tumors
- Infections
Yellow flag for back pain:
- Psychosocial problems
Sampling Technique
Non-probability Sampling Technique.
Sample Size
Sample size is calculated by using Epi software for sample size calculation. A study conducted at South Asia titled as “Participant in physical activity and back pain among an elderly population in South Asia” is used to calculate sample size.
Study Setting
- Tertiary care hospitals
Study Duration
3 months
Assessment Protocol
Back Patients were recruited from tertiary care hospitals after assessment and screening by consultants. Consent was taken from participants. Researcher re-examine patient and enrolled those who were met inclusion and exclusion criteria. Researcher filled self-administered questionnaire of those who fulfilled inclusion criteria. For rectus abdominis strength test researcher performed Kendell strength test and gave score as per performance.
Kendall’s Strength Test
- Kendall’s Lower Abdominal Test
is a test used to evaluate lower abdominal strength; subjects lie supine on a firm surface with arms folded across the chest; a tester assists in raising the legs up to a vertical position (subjects may actively raise one lower extremity at a time, if needed) keeping the knees straight; subjects then perform a posterior pelvic tilt and maintain this position while Khan U et al. Correlation Between LBP and Rectus Abdominis Muscle Weakness Using Kendall’s Grading Scale slowly lowering the legs to horizontal; strength is graded on the ability to keep the low back flat on the surface; the angle at which the back arches is noted and correlated with Kendall’s grading system (Kendall et al., 1993)15.
- Abdominal Strength Test
is a test of upper abdominal strength; subjects are asked to lie supine on a firm surface with knees extended; a roll is placed under the knees if the subject displays a positive Thomas Test; the subject is then asked to place both hands behind the head and proceed to slowly curl up to a sitting position completing spinal flexion range of motion; if this action cannot be achieved, the subject modifies the arm positions and a grade is assigned per Kendall’s muscle grading system (Kendall et al., 1993)15.
Data Analysis
SPSS Version 21 was used for data analysis. All categorical variables were used for jotting down frequencies and percentages. The association between two categorical variables was determined by applying chi-square test for significance. The significant P-value was less than 0.05
Ethical Consideration
- Confidential: Records of this study will be kept secured. Any information that patient tells us will remain confidential. The information’s will be kept in a locked file; only the researchers for this study will have access to the records.
- Autonomy: participants were independent to
take his or her decision to enroll in study.
- Beneficence: participants were requested to answer questions which may be private, but the data will not be shared with anyone else. Participants may refuse to answer any questions on the form. We will not share with anyone, the specific details you tell us.
- Justice: there was no harm of this research. Participants were included without any biasness
RESULTS
- Demographics
In the following table-1, the means and standard deviations of participant’s age and gender distribution is shown. There were in total 140 participants in this research study. The demographics showed the mean age of 29 years. There were 33.8% male and 66.2% female among participants.
| Table1. Percentage distribution of demographic characteristics of back pain patients | ||
| Demographic characteristics | n | % |
| Age (Mean±SD) years | 29.01±5.76 | |
| Gender | ||
| Male | 48 | 33.8 |
| Female | 94 | 66.2 |
 .
.
- Pain Characteristics of Participants Majority of participants were of acute back pain, followed by chronic back pain and most of the participants were not taking any medicine as shown in table 2,
Table 2 Percentage distribution of Pain characteristics of back pain patients Pain characteristics n % Duration of backache less than 6 weeks 58 40.8 6 to 12 weeks 41 28.9 more than 12 weeks 43 30.3 Taking any treatment Yes 68 47.9 No 74 52.1
Pain intensity was assessed on NPRS scale and most participants of the study were having moderate pain followed by mild pain as shown in table 3
| Table3. Percentage distribution of Pain Severity among back pain patients | ||
| Pain Severity | n | % |
| Pain(Mean±SD) years | 5.16±2.53 | |
| Severity of pain | ||
| Mild | 52 | 36.6 |
| Moderate | 61 | 43.0 |
| Severe | 29 | 20.4 |
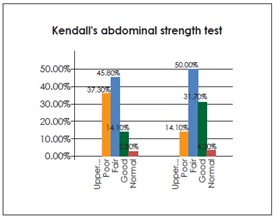
- Kendall’s Abdominal Test Score
Upper abdominal test score of most of the participant have grade 3 fair grade muscle power (45.8%) followed by grade 2 poor muscle power (37.3%) which was found statistically non-significant at P<0.509 (table 4).
| Table 4. Kendall’s Upper Abdominal test score | ||||
| Upper Abdominal test | N | % | Chi- Square Tests | P value |
| Poor | 53 | 37.3 | 5.276 | 0.509 |
| Fair | 65 | 45.8 | ||
| Good | 20 | 14.1 | ||
| Normal | 4 | 2.8 | ||
While performing lower abdominal test most participant have grade 3(fair grade) muscle power (50%) followed by grade 4 (good) muscle power (31.7%) which was found statistically significant at P<0.016, (table 5).
| Table5. Kendall’s Lower Abdominal test score | ||||
| Lower Abdominal test score | N | % | Chi- Square Tests | P value |
| Poor | 20 | 14.1 | 15.562 | 0.016 |
| Fair | 71 | 50.0 | ||
| Good | 45 | 31.7 | ||
| Normal | 6 | 4.2 | ||
When we correlate the back pain and power/strength of rectus abdominis there were no correlation shown between back pain and rectus abdominis power/strength. (table 6)
| Table 6. Spearman’s rho correlation pain score with Kendall’s Upper Abdominal test score and Kendall’s Lower Abdominal test score | ||
| Spearman’s rho | Kendall’s Upper Abdominal test score | Kendall’s Lower Abdominal test score |
| Correlation
Coefficient |
0.065 | -0.031 |
| Sig. (2-tailed) | 0.439 | 0.712 |
| N | 142 | 142 |
DISCUSSION
Back pain considers expensive disease in modern society. There are many causes/risks that leading to the occurrence of back pain. A cross sectional
study was conducted to evaluate contribution of rectus abdominis muscle in the patients with the complain of back pain. This study included 142 patients who were diagnosed with back pain, without any serious pathology.
In this study, both genders participants were included. It was found that female participants ratio was high in comparison to male participants. Buchbinder (2013) in their systemic review stated that women suffered with back pain more than men24, whereas in other study Hoy (2014) stated that, men are more prone to have back pain than women25.
The participants age group were between 20-40 years were included in this study, keeping in view Shiri study (2010) who concluded that Low back pain is common in participants ages between 24–39 years26.
In the current study Kendall, upper abdominal and Kendall lower abdominal test were used as outcome measure to assess muscle power of abdominal muscles. MacDonald (1998) concluded in his pilot study on 63 that there is increased incidence of low back pain that has been related with Lumbar lordosis, especially in women. The posture stretches and weakens the abdominals (rectus abdominis, external and internal oblique’s) while shortening the hip flexors and lumbar extensors imbalance increases the stress to the low back, resulting in pain. He conducted fitness test among school going children. He conducted Kendall’s lower abdominal and Kendall’s upper abdominal test to check the strength of rectus abdominis muscle15. In the current study, no relation found back pain patients and weakness of rectus abdominis. MOTA (2014) in her research concluded that women with DRA were not prone to develop back pain than women without DRA, this study support the present study14. In another study by Joran (2016) showed no difference between women with and without DRA, and prevalence of low back and/or pelvic girdle pain27. According to Stephanie Mulhearn there is some evidence of a link between low back pain, postural muscle endurance in gymnasts and no cause and effect relationship determined28.
On the contrary, Dalal khushboo (2014) conducted research on 30 women aged greater than 18 years to find correlation between diastasis rectus abdominis and lumbopelvic pain. Subjects were assessed on the Pelvic Floor Distress Inventory, Modified Oswestry Low Back Pain Disability Questionnaire, Visual Analog Scales (VAS) for pain. Diastasis Rectus Abdominis measurement was taken. Dalal concluded that the incidence for the DRA was 83.33%, and women with a DRA tend to have more lumbo-pelvic pain29.
The strength of the study was, it was a randomized control trail, single blindness, both genders were included in the study, and it was multi-centered study. The weakness of study is non-back pain patients were not included in the study so no comparison could have done between health and back pain patients.
CONCLUSION
In the current study, the prevalence of back pain is higher in females. There was no correlation found between back pain and rectus abdominis
REFERENCE
[1] Arslan SA, Hadian MR, Olyaei G, Bagheri H, Yekaninejad MS, Ijaz S, Kheradmand AA. Prevalence and Risk Factors of Low Back Pain Among the Office Workers of King Edward Medical University Lahore, Pakistan. PTJ. 2016;6(3):161-168
[2] Lee M, Song C, Jo Y, Ha D, Han D. The effects of core muscle release technique on lumbar spine deformation and low back pain. J Phys Ther Sci. 2015;27(5):1519-22
[3] Meucci RD, Fassa AG, Faria NM. Prevalence of chronic low back pain: systematic review. Rev Saude Publica. 2015;49
[4] Mostagi FQ, Dias JM, Pereira LM, Obara K, Mazuquin BF, Silva MF, Silva MA, de Campos RR, Barreto MS, Nogueira JF, Lima TB. Pilates versus general exercise effectiveness on pain and functionality in non-specific chronic low back pain subjects. J Bodyw Mov Ther. 2015;19(4):636-45
[5] Hirata RP, Salomoni SE, Christensen SW, Graven- Nielsen T. Reorganised motor control strategies of trunk muscles due to acute low back pain. Hum Mov Sci. 2015;41:282-94
[6] Bishwajit G, Tang S, Sanni Yaya ZF. Participation in physical activity and back pain among an elderly population in South Asia. J Pain Res. 2017; 10:905
[7] Zanuto EA, Codogno JS, Christófaro DG, Vanderlei LC, Cardoso JR, Fernandes RA. Prevalence of low back pain and associated factors in adults from a middle-size Brazilian city. Cien Saude Colet. 2015;20(5):1575-82
[8] Nelson-Wong E, Callaghan JP. Is muscle co-activation a predisposing factor for low back pain development during standing? A multifactorial approach for early identification of at-risk individuals. J Electromyography Kinesiol. 2010;20(2):256-63
[9] Meucci RD, Fassa AG, Paniz VM, Silva MC, Wegman DH. Increase of chronic low back pain prevalence in a medium-sized city of southern Brazil. BMC Musculoskelet Disord. 2013;14(1):155
[10] Acharry N, Kutty RK. Abdominal exercise with bracing, a therapeutic efficacy in reducing diastasis-recti among postpartal females. Physiother Res Int. 2015;3(2):999-1005
[11] Gray J, Aginsky KD, Derman W, Vaughan CL, Hodges PW. Symmetry, not asymmetry, of abdominal muscle morphology is associated with low back pain in cricket fast bowlers. J Sports Sci Med. 2016;19(3):222-6
[12] Silfies SP, Squillante D, Maurer P, Westcott S, Karduna AR. Trunk muscle recruitment patterns in specific chronic low back pain populations. Clin Biomech . 2005;20(5):465-73
[13] Correia JP, Oliveira R, Vaz JR, Silva L, Pezarat-Correia P. Trunk muscle activation, fatigue and low back pain in tennis players. J Sports Sci Med. 2016;19(4):311-316
[14] Da Mota PG, Pascoal AG, Carita AI, Bø K. Prevalence and risk factors of diastasis recti abdominis from late pregnancy to 6 months postpartum, and relationship with lumbo-pelvic pain. Man Ther. 2015;20(1):200-5
[15] McDonald GL, Nederveld KL. The Effects of Abdominal Strength Exercises and Testing on Posture in School Children.1998. Available from: https://scholarworks.gvsu.edu/theses/409
[16] Benjamin DR, Van de Water AT, Peiris CL. Effects of exercise on diastasis of the rectus abdominis muscle in the antenatal and postnatal periods: a systematic review. Physiotherapy. 2014;100(1):1-8
[17] Clark AW, Goedeke MK, Cunningham SR, Rockwell DE, Lehecka BJ, Manske RC, Smith BS. Effects of pelvic and core strength training on high school cross-country race times. J Strength Cond Res. 2017;31(8):2289-95
[18] Rett MT, Braga MD, Bernardes NO, Andrade SC. Prevalence of diastasis of the rectus abdominis muscles immediately postpartum: comparison between primiparae and multiparae. Braz J Phys Ther. 2009;13(4):275-80
[19] Shah SK, Honkalas P, Kumar A. Correlation of Low Back Pain and Diastasis Rectus Abdominis in Post-Menopausal Women between the Age Group of 50–60 Years. Indian J Physiother Occup Ther. 2016;10(3):108-11
[20] Chiarello CM, McAuley JA, Hartigan EH. Immediate effect of active abdominal contraction on inter-recti distance. J Orthop Sports Phys Ther. 2016;46(3):177-83
[21] Chiarello CM. Pregnancy-Related Pelvic Girdle Pain and Diastasis Rectus Abdominis. J Womens Health Phys Therap. 2017;41(1):3-9
[22] Unsgaard-Tøndel M, Vasseljen O, Woodhouse A, Mørkved S. Exercises for women with persistent pelvic and low back pain after pregnancy. Glob J Health Sci. 2016 ;8(9):107
[23] Malanga GA, Aydin SM, Holder EK, Petrin Z. Functional Therapeutic and Core Strengthening. In The Hip and Pelvis in Sports Medicine and Primary Care 2017 (pp. 185-214).
[24] Springer International Publishing. Buchbinder R, Blyth FM, March LM, Brooks P, Woolf AD, Hoy DG. Placing the global burden of low back pain in context. Best Pract Res Clin Rheumatol. 2013; 27(5):575-89
[25] Hoy D, March L, Brooks P, Blyth F, Woolf A, Bain C, Williams G, Smith E, Vos T, Barendregt J, Murray C. The global burden of low back pain: estimates from the Global Burden of Disease 2010 study.
Ann Rheum Dis. 2014: 73(6):968-974
[26]Shiri R, Solovieva S, Husgafvel‐Pursiainen K, Viikari J, Raitakari OT, Viikari‐Juntura E. Incidence of nonspecific and radiating low back pain:
followup of 24–39‐year‐old adults of the Young Finns Study. Arthritis care Res. 2010;62(4):455-9
[27] Sperstad JB, Tennfjord MK, Hilde G, Ellström-Engh M, Bø K. Diastasis recti abdominis during pregnancy and 12 months after childbirth: preva- lence, risk factors and report of lumbopelvic
pain. Br J Sports Med. 2016:
[28] Mulhearn S, George K. Abdominal muscle endurance and its association with posture and low back pain: An initial investigation in male and female elite gymnasts. Physiotherapy. 1999;85(4):210-6
[29] Dalal K, Kaur A, Mitra M. Correlation between diastasis rectus abdominis and lumbopelvic pain and dysfunction. Indian J Physiother Occup Ther.
2014;8(1):210