
ABSTRACT
Hypertension is a world health problem which is strongly related with cardiovascular disease (CVD) and premature deaths. The purpose of this cross-sectional study was to determine the prevalence of undiagnosed hypertension and associated risk factors among adults in Gajida town. The blood pressure (BP) of 364 participants was measured. Risk factors of high BP (age, gender, obesity, occupational stress, family history, educational level, dietary habits and smoking) were assessed. The data obtained was analyzed using both descriptive and interferential statistics. The descriptive (mean, standard deviation & percentage) and inferential (Pearson, Spearman & Mann-Whitney-U) statistics were used to summarize/analyze the data at P<0.05 using Statistical Package for Social Science (SPSS) (version 16.0). Out of 364 participants, 185 (50.8%) were males and 179 (49.2%) were females. On average, participant’s age was 33 years, systolic blood pressure (SBP) was 110 mm Hg, diastolic blood pressure (DBP) was 80 mm Hg and BMI was 19.96 kg/m2. About 153 (41.9%) of the participants were housewives and 138 (37.9%) were not educated. Prevalence of undiagnosed HTN was 23.6%. Gender, age, BMI, and educational level were found to be associated significantly (P ≤ 0.05) with HTN. Occupational stress, history of HTN, family history of HTN, dietary habits and smoking showed no significant relationship (p ≥ 0.05). A moderate prevalence of undiagnosed hypertension was found among adults in Gajida town. Hypertension is associated with gender, age, BMI, and educational level. There is a need to detect and manage cases of undiagnosed hypertension through regular measurements.
KEYWORDS
Hypertension, Adults, Undiagnosed, Nigerians, Risk Factors, Prevalence
INTRODUCTION
Hypertension (HTN) has been reported to be a major cause of global morbidity with devastating outcomes, and has significant financial burden on resources of health1. Bharati et al1 further stated that hypertension is a significant cause of premature deaths. Several studies2-4 have reported a worldwide prevalence of HTN. The studies showed that nearly one-quarter of world population between the age of 20 years and older live with diagnosed HTN and the trend increases with ageing.
According to Ogah et al4, there is a high prevalence of HTN in Nigerian states in both males and females. Findings from studies showed higher prevalence rates in males as compared to the females in general. However, with respect to rural/urban prevalence, the rural areas have higher rate of prevalence of HTN as compared to the urban areas with females reporting high prevalence of HTN in rural areas while males recording higher rate of prevalence in urban areas. Gajida being a rural area will benefit from this study. Other studies 5-7 reported conflicting reports on prevalence of HTN in rural and urban areas. The reason for this being peculiarity of the people in the region, their lifestyle, or facilities available. Gajida town lacks health care facilities, with poor educational level, lower socio-economic status, poor dietary habits and poor standard of living. This makes it necessary to conduct this study to determine the prevalence of undiagnosed HTN to prevent complications that are associated with it.
According to Marwiro8 and Fernandez-Feijoo et al9, with increase in the systolic and/or diastolic BP, there is greater possibility in the risk of stroke, kidney disorder, coronary heart disease and damage to the eye. End-organ damage occurs as a result of chronic high BP. Despite all these complications, many people do not know their BP status. Marwiro8 justify that “the cost effectiveness of early hypertension diagnosis and strict control as compared to management of its complications and the losses incurred by the rural council in form of off-sick. Therefore, it is important to assess the risk posed by hypertension through determination of the awareness, prevalence and risk factors for hypertension and its complications”.
Hypertension has been linked with several risk factors (history of HTN in the family, smoking of cigarette, ageing, gender, African race, high BMI, physical inactivity, lower social class, high salt and alcohol consumption)8,10. The people living in rural areas have poor educational level, poor standard of living, lower socio-economic level, poor dietary habits and lack of access to health care facilities which place them at risk of HTN11,12. Hypertension remains highly undiagnosed and it a major cause of premature deaths12, thus, making it a necessity to carry out this study in order to determine its prevalence. Das et al11 and Singh et al12
further reported that proper management of HTN can reduce mortality and this is only possible when the individual is aware of having the condition. According to Singh et al12, people living in remote areas may not have awareness about hypertension, its’ control and treatment due to unavailability of health care facilities, lower socio-economic status, poor educational level, poor standard of living and poor dietary habits. Considering all these factors, it becomes important to determine the prevalence of undiagnosed HTN in remote area. Hence, this research was centered in determining the prevalence and risk factors of undiagnosed HTN among the adults in Gajida Town.
Aims of the Study
The following were the purpose of this study:
- To determine prevalence of undiagnosed HTN among adults living in Gajida Town
- To highlight the associated risk factors of HTN among the population
- To determine the relationship between BP (SBP & DBP) and risk factors of HTN.
- To determine gender differences in prevalence of undiagnosed HTN among adults of Gajida town.
METHODS
Research Design
This study was a cross-sectional study carried out in Gajida Town.
Population of the Study
The population for this study comprised of all adults living in Gajida Town located in the Northern part of Tofa LGA of Kano state that are not previously diagnosed
as hypertensive.
Sample Size and Sampling Technique
A sample size of 364 participants was recruited for the study using convenient sampling in which a house-to-house enumeration of all adults’ blood pressure was conducted.
The formula used to calculate the sample size is11 n = z2pq/d2
Where, n= number of the sample; z= standard Z score; p = prevalence of hypertension; q= 1-p; d= absolute precision
Assuming 95% confidence level (z=1.96), prevalence of hypertension (p) of 35% and an absolute precision of 5% a total of 364 participant was calculated.
Therefore, n= (1.96)2(0.35) (1-0.35)/ (0.05)2; n=364
Inclusion Criteria
The participants were eligible if they are fulltime residents of the study area; adults aged 19 years and above.
Exclusion Criteria
Pregnant women; residents with musculoskeletal injury; Participants that are sick during the data collection; Known hypertensive individuals.
Data Collection Instruments
The instruments for data collection include:
- Mercury sphygmomanometer and Stethoscope (U-mec mercurial sphygmomanometer 300MMGH and Littmann stethoscope 3000/USA): These were used to assess the BP of participants to the nearest mm Hg.
- Portable Weighing scale (Model: Supreme; Make: Germany) – This was used to measure the body mass to the nearest Kg.
- Stadiometer (SECA gmbh/ Germany) – This was used to measure participants’ stature.
Data Collection Procedure
Ethical approval was sought from Hospitals Management Board, Kano. Approval to conduct this study was also got from the District Head, Gajida Ward. The procedure was fully explained to the
participants and consent of the participation was sought via completion of consent form.
The following measurements was made and recorded in the data sheet:
1.Stature
The participants were asked to stand anterior to the
stadiometer. Participants stood erect, with the trunk straight, the face facing forward, the arms by the side and the head straight. The calibrator was placed over the head of the participant and the reading was taken to the nearest centimeter13.
- Body Mass (BM) BM was assessed (with the subject bare footed and wearing light clothing) using a portable weighing scale, to the nearest kg13.
- Body Mass Index (BMI) The BMI was calculated using the following formula13:
BMI = Weight (kg)/[Height (m)]2.
- Blood Pressure
The participant was instructed to comfortably sit and place arm at heart level. The blood pressure was measured twice in the right arm with an interval
of at least ten minutes (10mins). Blood pressure was measured using a mercury sphygmomanometer12. It was ensured that the participants did not consume any caffeinated drink, did not engage in any form of physical activity, and not smoked cigarette for at least half-an-hour before assessing the BP. The average reading was recorded. Either systolic BP (SBP) or diastolic BP (DBP) of ≥140 mmHg and ≥90 mmHg respectively was used to determine hypertension14.
- Risk Factors of Hypertension
The following risk factors were assessed:
- Obesity
BMI value of >30kg/m2 was used to indicate obesity15.
The obesity associated risk was coded as: 0 = at no risk; 1 = at risk.
(b) Age
The age of participants was recorded in years. The age associated risk was grouped as follows16: 19-49 years = at no risk Coded as “0”; ≥50years = at risk Coded as “1”.
(c) Occupational Stress
Occupationally stressed participant was considered at risk of developing HTN and was Coded as: 0= at no risk; 1 = at risk.
(d) Education Level
Participants that are educated were considered as less likely to developed HTN17 and were coded as: 0
= at no risk; 1= at risk.
(e) Family History of HTN
An individual having a family history of HTN was considered at risk8 and was coded as: 0 = at no risk; 1= at risk.
(f) Dietary Habits
An individual with poor dietary habits was considered at risk of HTN18. It was coded as: 0 = at no risk; 1= at risk.
(g) Smoking
An individual who is currently a smoker or have ever smoked in his lifetime was considered at risk of HTN19. It was coded as: 0 = at no risk; 1 = at risk
Data Analysis Procedure
Data was analyzed using both descriptive and interferential statistics. The descriptive statistics summarized data using mean, standard deviation and percentage. Interferential statistics of Spearman and Pearson was computed to determine relationship between BP and risk factors of HTN. Mann-Whitney-U was used to determine difference in prevalence of HTN across gender. Statistical Package for Social Sciences (SPSS) (version 16.0) was used for the analysis at significance level of P<0.05.
RESULTS
A total number of three hundred and sixty four (364) subjects participated in the study. Out of which 185 (50.8%) were males and 179 (49.2%) were females. The physical/anthropometric characteristics of the study participants are shown in Table 1.
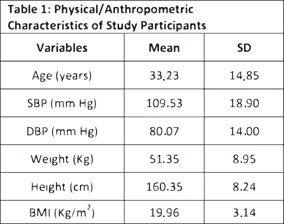
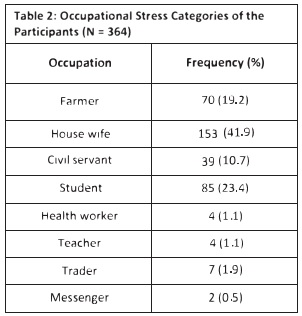
This study found that majority of the participants fall within the middle age category and they are averagely normal weight individuals. The result also showed that the BP of the participants is in the safer range. Table 2 shows that majority of the participants were house wives with very few Messengers.
As seen from the table 3, most of the participants are not educated, only few went through school.
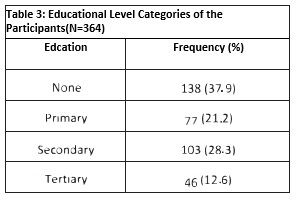
Table 4 describes some risk factors of hypertension with family history being the highest followed by dietary habits.
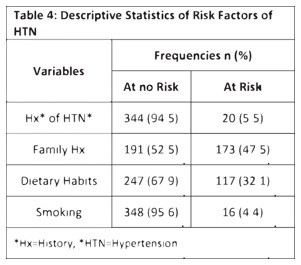
Table 5 shows that moderate number of participants were newly diagnosed as hypertensive.
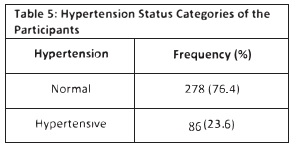
Table 6 shows the correlation between physical/anthropometric characteristics, some risk factors and prevalence of undiagnosed hypertension. There is a significant relationship between prevalence of undiagnosed hypertension and gender, age, BMI and educational level.
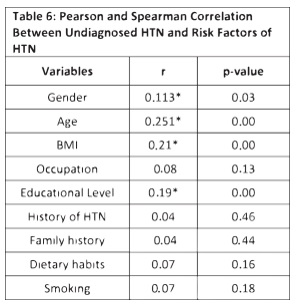
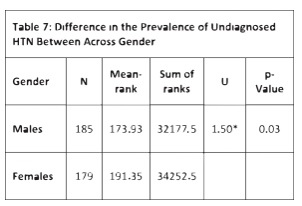
Table 7 shows summary of prevalence of undiagnosed HTN across gender. Mann Whitney U analysis shows that there is a significant difference between the male and female scores of HTN (SBP & DBP) (U= 1.497, p = 0.032).
DISCUSSION
This research determined the prevalence of undiagnosed hypertension among adults in Gajida town as 23.6% which is less than the 27% prevalence assessed among the general population in Zimbabwe8. Similar report was documented by Dolatabadi et al20 in an attempt to determine the prevalence of undiagnosed HTN in an emergency department of Imam Hossein Medical and Educational center, Teheren, Iran. The prevalence was found to be28.6%. Barron et al21 conducted a similar study among adults aged 45 years and above, andfound the prevalence of undiagnosed hypertension to be 62%. More so, the prevalence was higher among men (46.8%) than women (31.2%). A number of studies have determined the hypertension prevalence rate among rural population and this range from 1.99% and 21.2% in 1958 and 1994 respectively. However, the difference in the rates is may be due to different cut-off values used in diagnosis of hypertension and the different age categories among subjects of the study.
Prevalence rates of 24.9%, 32.2%, 25.2%, and 19.04% of undiagnosed hypertension were reported in rural areas of West Bengal22, Lucknow23, Tamil Nadu24 and central India25 respectively. A prevalence of 33.3% undiagnosed hypertension was reported in eastern India among the native people of Assam. In the rural areas of Jammu and Andhra Pradesh, a 13% and 27% prevalence of high BP was recorded respectively in people of greater than 30 years. This finding is similar to reports from industrialized countries.
Age
The prevalence of high BP increased with an increase in age in this study. This finding is similar to other studies in various parts of India. A study in north India reported highest prevalence of high BP among the 60-69 year age category. The findings are also consistent with those reported by Erem et al 26-28, Wang et al29 and Lim et al 30 from Turkey, US and Malaysia respectively.
Diet
This study shows no significant relationship between dietary habits and HTN. It is consistent with a report by Marwiro8. In contrast, Reddy et al31 showed a significant relationship between prevalence of high BP and dietary habit.
Education
The status of education was significantly related to prevalence of high BP in this study. More so, Erem et al28 stated that low educational status was related to high prevalence of hypertension in Turkey. Some
researches32,33 reported that no relationship between educational status and hypertension. Occupation This study showed no significant relationship, however, it was noted that hypertension is significantly related with sedentary life style. Previous studies23,25,34-38 show that hypertension was prevalent in people who live a sedentary life. A similar trend has been reported in different ethnic groups.
Sex
Hypertension prevalence was different across gender in this research. This finding is similar to previousfindings 25,26,39. However, some studies1,28 havereported that hypertension has no relationship with gender.
Family History of Hypertension
Hypertension family history was not related to hypertension in the present study. This finding is consistent with the reports of Bharati et al1 and Yadav et al23; however, Divan et al33, Reddy et al31 and Erem et al28
reported a positive association of family history of hypertension.
Smoking Habit
In the present study, the habit of smoking was not related to hypertension. Divan et al33 and Yadav et al23 reported similar findings. Others reported no association1,8,24,25,31.
Body Mass Index
It was noted from this study that hypertension is related to BMI. This finding was also noted in previous studies23-25,28,31,32,34.
CONCLUSION
A moderate prevalence of undiagnosed hypertension was found among adults in Gajida town aged 19 years and older. Hypertension is related to age, gender, BMI, and educational level. On the other hand, occupational stress, history of HTN, dietary habits, family history, and smoking showed no relationship with hypertension.
RECOMMENDATION
A moderate number of adults in Gajida town are living with undiagnosed hypertension. This finding highlights the need for services to further diagnose and manage cases of undiagnosed hypertension as this condition may be asymptomatic. Routine measurement of BP makes possible early diagnosis and management of hypertension and this can further avoid any harm to health. Also, the Director, Health Services, Tofa LGA, should organize some program on health education to promote awareness, detection and management of high BP. Campaigns need to be organized at work places to educate the people on hypertension and its association with obesity and level of education. High risk female individuals who are obese, above age forty with a family history of hypertension should be encouraged to have routine BP measurements. Posters should be used to convey information on physical activities and weight loss.
A surveillance system should be set up in Gajida town for risk factors of hypertension. This will enable monitoring and determination of prevalence of undiagnosed hypertension and its risk factors. It will further be beneficial in evaluation of interventions. Also, further studies should be conducted on the factors related with poor control of BP among persons already receiving treatment of HTN, knowledge and attitude of adults in Gajida town towards obesity and physical activity. In view of the moderate prevalence of undiagnosed HTN among adults in Gajida town compared to other population, a comparison study of Gajida town and other population may determine if there are factors peculiar to Gajida town.
REFERENCES
[1] Bharati DR, Nandi P, Yamuna TV, Lokeshmaran A, Agarwal L, Singh JB, et al. Prevalence and Covariates of Undiagnosed Hypertension in the Adult Population of Puducherry, South India. Nepal J Epidemiol. 2012;2(2):191-199
[2] Mancia G, De Backer G, Dominiczak A, Cifkova R, Fagard R, Germano G et al. ESH-ESC Task Force on the Management of Arterial Hypertension. J Hypertens. 2007;25(9):1751-1762
[3] Kearney PM, Whelton M, Reynold, K, Muntner P, Whelton PK, He J. Global burden of hypertension. Analysis of worldwide data. Lancet. 2005;365(9455):217-223
[4] Ogah OS1, Okpechi I, Chukwuonye II, Akinyemi JO, Onwubere BJ, Falase AO, et al. Blood pressure, prevalence of hypertension and hypertension related complications in Nigerian Africans: A review. World J Cardiol.
2012;4(12):327-340
[5] Opie LH, Seedat YK. Hypertension in Sub-Saharan African populations. Circulation.
2005;112(23):3562-3568
[6] Ng N, Stenlund H, Bonita R, Hakimi M, Wall S, Weinehall L. Preventable Risk Factors for Non-communicable disease in Rural Indonesia Prevalence Study using WHO STEPs Approach. Bull. World Health Organ. 2006;84(4):305-313
[7] Kaufman JS1, Tracy JA, Durazo-Arvizu RA,Cooper RS. ICSHIP Investigators. Lifestyle, Education, and Prevalence of Hypertension in Populations of African Origin. Ann Epidemiol. 1997;7(1):22-27
[8] Marwiro A. Prevalence and Risk Factors for Hypertension among Bulawayo City Council Employees. [Masters Dissertation]. University of Zimbabwe; Zimbabwe. 2010
[9]Fernández-Feijoo J, Núñez-Orjales JL, Limeres-Posse J, Pérez-Serrano E, Tomás-Carmona I. Screening for hypertension in a Primary Care Dental clinic. Med Oral Patol Oral Cir Bucal. 2010;15(3):467-472
[10] Graham I, Atar D, Borch-Johnsen K, Boysen G, Burell G, Cifkova R. European Guidelines on Cardiovascular Disease Prevention in Clinical Practice. Eur Heart J. 2007;28(19):2375-2414
[11] Das OP, Vijaya AN, Ashwini B, Narasannavar RS. Prevalence of Hypertension among Adults Residing In Urban Slums of Ramnagar, Belgaum
City-A: Cross-Sectional Study. Journal of Dental and Medical Sciences. 2014;13(5):102-104
[12] Singh AK1, Mani K, Krishnan A, Aggarwal P, Gupta SK. Prevalence, Awareness, Treatment and Control of Hypertension Among Elderly Persons in an Urban Slum of Delhi, India. Indian J Community Med. 2012;37(4):236-239
[13] Owoeye OBA, Olawale OA, Tella BA, Ajuluchukwu JN, Akinbo SRA. Prevalence of Hypertension and Pre-hypertension in Male Adolescent Football: A Cross-Sectional Cohort Study of Nigerian Players. American J Hyperten Res. 2013;1(1):26-28
[14] Effects of weight loss and sodium reduction intervention on blood pressure and hypertension incidence in overweight people with high-normal blood pressure. The Trials of Hypertension Prevention phase II. Arch Intern Med. 1997;157(6):657-667
[15] Bcheraoui CEI, Memish ZA, Tuffaha M, Daoud F, Robinson M, Jabar S, et al. Hypertension and its associated risk factors in the Kingdom of Saudi Arabia, 2013: A National Survey. Int J Hypertens. 2014;1-8
[16] Cipullo JP1, Martin JF, Ciorlia LA, Godoy MR, Cação JC, Loureiro AA, et al. Hypertension prevalence and Risk Factors in a Brazilian Urban Population. Arq Bras Cardiol. 2010;94(4):519-26
[17] Powdthavee N. Does Education Reduce the Risk of Hypertension? Estimating the Biomarker Effect of Compulsory Schooling in England. J Hum Cap. 2010;4(2):173-202
[18] Bhat B, Shenoy J, Dutt A, Kumar S, Kalpana B, Bhat S, Shet U. Influence of Dietary Habits on Blood Pressure in Preadolescent Boys of Coastal Karnataka. National Journal of Physiology. J. Pharm. Pharmacol. 2012;3(1):9-13
[19] Abtahi F, Kianpour Z, Zibaeenezhad MJ, Naghshzan A, Heydari ST, Babaie MA, Khosropanah S, Moaref AR. Correlation between Cigarette Smoking and Blood Pressure and Pulse Pressure among Teachers Residing in Shiraz, Southern Iran. Iran Cardiovasc Res J. 2011;5(3):97-102
[20] Dolatabadi AA, Motamedi M, Hatamabadi H, Alimohamadi H. Prevalence of Undiagnosed Hypertension in the Emergency Department. Trauma Mon. 2014;19(1):7328
[21] Barron S, Balanda K, Hughes J, Fahy L. National and sub-national hypertension prevalence estimates for the Republic of Ireland: better outcome and risk factor data are needed to produce better prevalence estimates. BMC Public Health. 2014;14:24
[22] Das SK, Sanyal K, Basu A. Study of urban community survey in India: growing trend of high prevalence of hypertension in a developing country. Int J Med Sci. 2005;2(2):70-78
[23] Yadav S, Boddula R, Genitta G, Bhatia V, Bansal B, Kongara S, et al. Prevalence & risk factors of pre-hypertension & hypertension in an affluent north Indian population. Indian J Med Res. 2008;128(6):712-720
[24] Kannan L, Satyamoorthy TS. An epidemiological study of hypertension in a rural household community. Sri Ramachandra J. Med. 2009;2(2):9-13
[25] Kokiwar PR, Gupta SS, Prevalence of hypertension in a rural community of central India. Int J Biol Med Res. 2011;2(4):950-953
[26] Hazarika NC, Narain K, Biswas D, Kalita HC, Mahanta J. Hypertension in the native rural population of Assam. Natl Med J India. 2004;17(6):300-304
[27] Chow CK, Naidu S, Raju K, Raju R, Joshi R, Sullivan D et al. Significant lipid, adiposity and metabolic abnormalities amongst 4535 Indians from a developing region of rural Andhra Pradesh. Atherosclerosis. 2008;196(2):943-952
[28] Erem C, Hacihasanoglu A, Kocak M, Deger O, Topbas M. Prevalence of prehypertension and hypertension and associated risk factors among Turkish adults: Trabzon Hypertension Study. J Public Health. 2009;31(1):47-58
[29] Wang Y, Wang QJ. The prevalence of pre-hypertension and hypertension among US adults according to the new joint national committee guidelines: new challenges of the old problem. Arch Intern Med. 2004;164(19):2126-2134
[30] Lim TO, Morad Z. Prevalence, Awareness, Treatment and Control of Hypertension in the Malaysian Adult Population: Results from the National Health and Morbidity Survey 1996. Singapore Med J. 2004;45(1):20-27
[31] Reddy SS, Prabhu GR. Prevalence and risk factors of hypertension in adults in an urban slum, Tirupati, A.P. Indian J Community Med. 2005;30(3):84-86
[32] Manimunda SP, Sugunan AP, Benegal V, Balakrishna N, Rao MV, Pesala KS. Association of hypertension with risk factors & hypertension related behaviour among the aboriginal Nicobarese tribe living in Car Nicobar Island, India. Indian J Med Res. 2011;133(3):287-293
[33] Divan V, Chauhan V, Panchal S, Bansal RK. Prevalence of hypertension amongst workers of a fertilizer company in Surat District. Indian J Community Med. 2010;1(2):153-155
[34] Singh RB, Beegum R, Ghosh S, Niaz MA, Rastogi V, Rastogi SS, et al. Epidemiological study of hypertension and its determinants in an urban population of North India. J Hum Hypertens. 1997;11(10):679-685
[35] Malhotra P, Kumari S, Kumar R, Jain S, Sharma BK. Prevalence and determinants of hypertension in an un-industrialized rural population of North India. J Hum Hypertens. 1999;13 (7):467-472
[36] Anand MP. Prevalence of hypertension amongst Mumbai executives. J Assoc Physicians India. 2000;48(12):1200-1201
[37] Chockalingam A, Ganesan N, Venkatesan S, Gnanavelu G, Subramaniam T, Jaganathan V, et al. Patterns and predictors of prehypertension among “healthy” urban adults in India. Anqiology. 2005;56(5):557-563
[38]Zachariah MG, Thankappan KR, Alex SC, Sarma PS, Vasan RS. Prevalence, correlates, awareness, treatment, and control of hypertension in a middle-aged urban population in Kerala. Indian Heart J. 2003;55(3):245-251
[39] Raina DJ, Jamwal DS. Prevalence Study of Overweight/Obesity and Hypertension among Rural Adults. JK Science. 2009;11(1):20-23