
ABSTRACT
OBJECTIVE
To evaluate the effects of phase II cardiac rehabilitation (CR) on functional capacity and hemodynamic parameters of patients with CVD
STUDY DESIGN
Quasi Experimental Study
METHODOLOGY
121 individuals were recruited in cardiac phase II rehabilitation program by a simple random sampling, aged between 45-65 years, assessed on day 1 on the basis of medical history and 6 Minute Walk Test (6MWT). The patients were then enrolled into eighteen session of hospital based supervised exercise program according to ACSM’s guidelines.
RESULTS
The statistical analysis shows the significant changes in the functional status and hemodynamic variables of the participants after exercise session, where the post exercise heart rate was decreased to around 2.2±0.8 beats/minute with the p value of 0.001; systolic and diastolic blood pressure was plummeted to around 12.3±2.5 and 46.1±9.2 mmHg respectively with the p value of 0.00 and 0.001. The rate of exertion has been decreased by 6.2±1.5 (p value =0.0001) and the distance covered was increased to 111.9 meters (p value = 0.0002).
CONCLUSION
The study has concluded that potency of eighteen session of phase II cardiac rehabilitation is found to be effective in improving the functional status, hemodynamic variable and the myocardial workload of cardiac patients, determined by 6MWT.
KEYWORDS
Cardiac Rehabilitation, Six Minute Walk Test, Functional Capacity, Hemodynamic, Parameters, Cardiac Risk Factors.
Muhammad Usman Khan
Assistant Professor
Ziauddin College of Physical Therapy
Ziauddin University
Sumaira Imran Farooqui
Associate Professor, Principal
Ziauddin College of Physical Therapy
Ziauddin University
Farzana Amir Hashmi
Deputy General Manager, HOD
Preventive Cardiology and Cardiac
Rehabilitation
Tabba Heart Institute
Amna Aamir Khan
Assistant Professor
Ziauddin College of Physical Therapy
Ziauddin University
[Khan MU, Farooqui SI, Hashmi FA, Khan AA. Effects of Cardiac Rehabilitation on the Functional
Capacity and Hemodynamic Parameters of Patients with CVD using 6MWT. Pak. j. rehabil. 2017;6(1):21-27]
INTRODUCTION
Cardiovascular disease (CVD) is a leading cause of universal morbidity and mortality with an estimated death of around 17.3 million in one year which is expected to be more than 23.6 million by 20301. About 80% of deaths are due to heart attack and stroke2, out of that more than 75% of deaths occur in developing countries2. As per Shifa International Hospital, Islamabad among 30 to 40 percent of all deaths in Pakistan due to non-communicable diseases, cardiovascular disease has the leading mortality rate that has reached to about 2lacs deaths per year estimated to around 410/100,000 of the population3. The risk factors of the cardiovascular disease are enormous and are divided into modifiable and non-modifiable risk factors4. Modifiable risk factors include hypertension, tobacco use, raised blood glucose, physical inactivity, unhealthy diet, cholesterol, and overweight/obesity whereas age, gender and family history non-modifiable risk factors5. As majority of the cardiovascular problem is account from the modifiable risk factors that can be controlled the health care system around the globe are now primarily working on a multidisciplinary approach in order to prevent, controlled and rehabilitate the patient from the complications that arises from this disease6.
Over a last few decades cardiac rehabilitation has evolved from the point of simple monitoring to a multidisciplinary approach7, where the optimization of medical treatment can be augmented by the inclusion of supervised exercised plan, individualized diet plan, individual counseling, patient and family education for management of diabetes, hypertension (HTN), dyslipidemia, smoking cessation, obesity and stress8. Sedentary lifestyle is a fourth leading risk factor of cardiovascular diseases, that accounts for 3.2 million deaths/year and 32.1 million DALYs (disability adjusted life year)4. Insufficient physical activity is referred to the moderate activity of less than 30 minutes per week or vigorous activity of less than 20 minutes9. Cardio-respiratory fitness has a direct relationship with the physical fitness, thus makes physical activity an integral part of cardiac rehabilitation10. According to a study, cardio-respiratory fitness decreases by 27% in individual after continuous 20 days of bed rest11 and daily step count decreases from 10,051 to 1344 with estimated decreases in VO2 max of 7%12. Traditionally there are three phases of cardiovascular rehabilitation (CR) with the aim to smooth the progress of recovery and to prevent progression of the disease13. Phase-I is initiated when the patient is still in the hospital with the aim to improve early mobility of patient; Phase-II also called as a supervised ambulatory outpatient program having the duration of 6-8 months and is aimed to improve the cardiovascular and cardio-respiratory fitness of the patient; the final phase also called as the lifetime maintenance phase or Phase-III is based on the intend to modify the risk factors through the exercises learned in Phase-II14,15.
It is evident from the study that around 50% reduction in the risk of mortality occurs through exercise based cardiac rehabilitation programs16, whereas 28% reduction in the risk is achieved by other modifiable factors, particularly smoking17. Thus making phase-II cardiac rehabilitation as an important aspect in controlling and preventing cardiovascular disease, scientific data has clearly established that improvement of 1MET (Metabolic Equivalent to Task) in functional capacity reduces 12% of mortality risk due to CVD18. Similarly the role of nutritional counseling and weight management is also important, as studies have suggested dietary recommendationsduring cardiovascular rehabilitation phase-II. It includes reduction in saturated fat intake that is <7% of total calories, cholesterol <200mg/dl and increase in uptake of polyunsaturated fat for about 10% of total calories, monounsaturated fat approximately 20% of total calories with adequate repartition of calorie sources for about 50-60%, 15% and 25-35% of carbohydrates, proteins and fats respectively and the increase in fiber intake (about 20-30 g/d)19. The weight management with a body mass index of 18.5-24.9 kg/m2 and waist circumference of <40 inches in men and <35 inches in women is recommended with an initial approach of reducing approximately 10% of weight from baseline during the rehabilitation phase. The role of psychosocial management is also essential as it affect both morbidity and mortality. Studies have revealed that 20% of patients following myocardial infarction suffer from, depression, anxiety, and denial20. Moreover, 30% of the population during the phase-II of cardiac rehabilitation takes unnecessary stress resulting in hypertension, increased blood glucose, cholesterol levels and body weight ultimately increases the development of atherosclerosis21. Thus making cardiac rehabilitation a multidisciplinary approach where the role of physical therapy intervention can be augmented by the indulgence of other medical health care professionals like nutritionist, psychologist, nurses etc. in improving the patient’s health and heart related concerns. The effects of phase II cardiac rehabilitation on functional capacity and hemodynamic variables of the participants using 6 Minutes-Walk Test (6MWT) as an indicator in patients with CVD.
METHODOLOGY
Study Setting
The study was conducted in the outpatient department of Tabba Heart Hospital, Karachi.
Target Population
Patient with cardiovascular disease enrolled in Phase-II Cardiac Rehabilitation program.
Study Design
Quasi Experimental Study
Duration of Study One year
Sampling Technique
Simple random sampling technique
Sample Size Sample size of 121 patients have been included in the study
Inclusion Criteria
- Patients with diagnosed CVD
- Both male and female of age 45-65 years
Exclusion Criteria
- Medical red flags like tumor, uncontrolled hypertension
- Structural deformity like scoliosis, that limits the
functional capacity of respiratory system
- Surgery that limits the inclusion of patient in Phase
II cardiac rehabilitation
Training Protocol
The patient after being recruited in the training program for phase II cardiac rehabilitation would be assessed on day 1 on the basis of medical history, functional capacity and hemodynamic variables by using 6MWT. The patients were then place into an eighteen session of supervised exercise program based on ACSM’s protocol of Frequency, Intensity, Time and Type. The protocol of the exercise was as follows:
- Frequency
6-8 weeks/ 3 sessions per week
- Intensity
Ranging from 20% to 59% of Target Heart Rate (HR) during exercise and RPE (Rate perceived Exertion) ranging from10-13 during exercise.
- Time
Each session ranging from 30 minutes initially (with 10 minutes bouts) then gradually duration increased up to 60 minutes per session.
- Type
Treadmill, cycling and arm ergometer Telemetry monitor remain attached throughout sessions. Blood pressure (BP), heart rate (HR), pulse, rate of perceived exertion (RPE), Electrocardiograph (ECG), Oxygen Saturation (SpO2) and physical symptoms has been observed throughout the whole session, time to time specially (in start, during exercise and post session). Each recruited patient performed exercises within the prescribed intensity according to the exercise dosage plan of calculated target heart rate zone for each individual. Exercises were prematurely be terminated on the base of prescribed measures by American College
of Sports Medicine (ACSM) on the basis of Oxygen Saturation, ECG monitoring and RPE scale. The effects of exercise protocols were measured by using the parameters of 6MWTS and were compared from the values taken on the first day of exercise session. Beside exercise session diet consultation has been offered and education has been provided time to time about stress management, dietary habits and life style modification for related risk factor.
Ethical Considerations
Ethical issues considered in my studies are following:
- Confidentiality statement was issued to all participants because confidentiality and privacy of identity was an important aspect of personal security.
- Consent will be obtained from the participants to ensure the risk and costs regarding the treatment
- Participants had the right to with draw from study at any time.
- Data collection in the hospital/institute was done after permission from Head of department of Physiotherapy.
RESULT
A total number of 121 patients were recruited in this study. The demographic characteristics of the patient recruited are shown in Table 1.
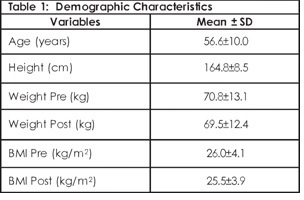
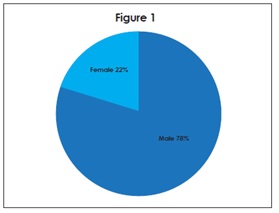
The mean age and height of the patients recruited in the study were 56.6 years and 164.8cm respectively. Out of them, 95 were males and 26 were females. The description of the participants according to gender is shown in Figure 1.
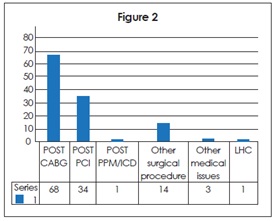
Out of 121 subjects that were recruited in the study, 68 were with the history of post Coronary Artery Bypass Grafting (CABG), 34 with post Percutaneous Coronary Intervention (PCI), 1 each for both post Implantable Cardioverter Defibrillator (ICD) and left heart catheterization and the rest had some other surgical and medical issues. The details are shown in Figure 2.
At baseline, the hemodynamic variables of the participants were taken after performing the 6MWT that includes heart rate, oxygen saturation rate, blood pressure, rate of perceived execration using Borg scale and total distance covered in meters during 6MWT. The baseline information obtained was compared with the values after performing cardiac rehabilitation session on the same day. The details are shown in Table 2. The values from 6MWT before and after performing a single day session of phase II cardiac rehabilitation shows no changes with the p-value of 0.00. However, some changes were observed in oxygen saturation level that has been dropped to 90±12.2 with the p-value of 0.03 after performing exercises prescribed for phase II cardiac rehabilitation.
Table 2: Variables after performing 6MWT at Day 1 of Cardiac Rehabilitation (CR) Session
| Variables | Before CR Session Mean± SD | After CR Session Mean± SD |
| Heart Rate | 7.8 0±11.5 | 86.0±12.2 |
| Oxygen Saturation | 98.5±11.5 | 90±12.2 |
| Systolic BP | 130±10.5 | 140±12.5 |
| Diastolic BP | 110.8±14.2 | 120.6±18.5 |
| RPE | 5.7±2.4 | 8.7±3.6 |
| Distance covered during 6 MWT | 274.3±60.9 | 363.5±64.7 |
| Variables | Before CR Session Mean± SD | After CR Session Mean± SD |
| Heart Rate | 74.8±12.7 | 83.8±12.4 |
| Oxygen Saturation | 98.5±1.2 | 98.8±1.2 |
| Systolic BP | 120.7±11.5 | 127.7±12.4 |
| Diastolic BP | 80.6±8.5 | 74.6±8.9 |
| RPE | 1.6±1.1 | 2.5±1.1 |
| Distance covered during 6 MWT | 476.4±20.7 | 475.4±10.3 |
The statistical analysis shows significant changes as the resting heart rate of the patient decreases by 3.2±1.2 beats per minutes with a p value of 0.002. The resting systolic and diastolic BP also falls to around 9.3±1.8mm of Hg and 30.6±5.2mm of Hg respectively having the p value of 0.004. The significant changes were also observed in RPE scale and a distance covered during 6MWT with the p-value of 0.001. The values were compared with the values taken at the post exercise session on first day. The statistical analysis shows that significant changes were occurred in the hemodynamic variables of the participants after exercise session as well where the post exercise heart rate was decreased to around 2.2±0.8 beats per minute with the p value of 0.001 and systolic and diastolic BP were plummeted to around 12.3±2.5 and 46.1±9.2 mm of Hg with the p value of 0.00 and 0.001 respectively. The changes were also observed on RPE scale where the rate of exertion has been decreased by 6.2±1.5 (p value 0.0001) and the distance covered was increased to 111.9 meters (p value 0.0002).
DISUSSION
The study involve the use of 6MWT as an indicator to identify the effects of phase-II cardiac rehabilitation exercises on patients underwent different cardiac surgical procedures as 6MWT is a predictor of incidence for re-hospitalization of patients who fails to cover a distance of more than 240 meters22. The result of this study shows that not only cardiac rehabilitation improves the hemodynamic variables of the patients but also improves their functional status. The result is according to the study conducted by Wenger N which stated that multidisciplinary approach involving the psychological parameters in CR improves the exercise tolerance in cardiac patients23. Study conducted Araya-Ramírez F found that initial walk test has an inverse relation (r=0.47 p<0.001) with 6MWT as lowest initial 6MWT exhibit greater improvement than those who have initially high 6MWT24. Audelin MC et al found that Phase II cardiac rehabilitation is safe even in patient of >75 years of age as it decreases the incidence of re-hospitalization of patients after heart surgeries25. Achttien RJ aims a meta-analysis to found the effectiveness of exercise-based CR in patients with coronary heart disease (CHD) and found the strong evidence regarding the effectiveness of exercise-based CR during all phases of CR26. Patient attended cardiac rehabilitation achieved a significant improvement in health-related quality of life as their functional status gets improved and they get better control on their hemodynamic responses. The strongest effect occurred in the first 8 weeks, when patients were receiving the most intense phase of the intervention27. Ramin Shabani et al in his study effect of CR program on exercises capacity in women undergoing coronary artery bypass graft concluded that effects of 12 weeks of training using cardiac rehabilitation protocol significantly improves the myocardial work load of women undergone coronary artery bypass graft than those who did not received any rehabilitation interventions the study also analyzed the effects of phase II CR program on Peak Rate Pressure Products (PRPP) and suggested that not only cardiac rehabilitation aims to improves the resting parameters of patients but focus should also be given to improves the hemodynamic parameters during and after every session of exercise28. Fiorina et al showed that 6MWT was well accepted in patients who had undergone a supervised cardiac rehabilitation phase29. In another study Vincent et al concluded that incorporation of resistance exercises regimen into supervised exercises program during phase-II cardiac rehabilitation provides additional benefits in terms of improving muscular strength, cardiorespiratory functions and physical functions30. Effects of phase-II cardiac rehabilitation has also been observed on exercise capacity and quality of life in different studies which provide evidences that six weeks of exercises significantly improves the distance covered during 6MWT and also concluded that metabolic equivalents of exercises stress test and 6MWT has a strong direct positive correlation (r=0.87)31. Ching-Huang Hung found that supervised cardiac rehabilitation was more effective in comparison to home based exercises program in improving the fitness of the patients after post CABG32. The study involves the assessment of fitness parameters by incorporating ACSM elements of fitness included body composition, flexibility, muscle strength, endurance and cardiopulmonary function32. Study by Ragawanti P et al found that a significant difference in the functional capacity was observed in patient before and after coronary revascularization, however greater improvement are found in patients who underwent CR for four to six weeks for 30-60 minutes and treated with 11 series of exercises33. Craciun et al 2011 had emphasized on the importance of intensive cardiac rehabilitation program in cases in which patients had low functional capacity <45%34, thus making cardiac rehabilitation program as an integral part of preventing the patient from the post cardiac surgical complications. The sample of the study includes greater number of male participants in comparison to female which may be due to the cultural barriers which limits the enrollment of female participants in phase-II CR hence same reflects in the present study as well35. However not all patients with cardiac disease are apposite for such an exercise program, this care component needs to be modified according to the requirement of the individual making the aspect of clinical decision making as an integral part in evaluating the complexity of disease in terms of its impact on an array of patient outcome.
CONCLUSION
The study concluded that potency of phase II cardiac rehabilitation is found to be effective in improving the functional status, hemodynamic variable and the myocardial workload of cardiac patients determined by 6MWT. The variables of 6MWT improve after the completion of cardiac rehabilitation program.
REFERENCES
[1] Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M et al. Heart Disease and Stroke Statistics-2016 Update: A Report from the American Heart Association. Circulation. 2016;133(4):e38-360
[2] Roth GA, Huffman MD, Moran AE, Feigin V, Mensah GA, Naghavi M, Murray CJ. Global and regional patterns in cardiovascular mortality from 1990 to 2013. Circulation. 2015;132(17):1667-1678
[3] Dawber TR, Moore FE, Mann GV. II. Coronary heart disease in the Framingham study. Int J Epidemiol. 2015;44(6):1767-1780
[4] Mendis S, Puska P, Norrving B. Global Atlas on Cardiovascular Disease Prevention and Control. Geneva: World Health Organization in collaboration with the World Heart Federation and World Stroke Organization; 2011.
[5] Regional Office for Southeast Asia. World Health Organization. Sep 2011. Hypertension fact sheet. Available from: http://www.searo.who.int/entity/noncommunicable_diseases/media/non_communicable_diseases_hypertension_fs.pdf
[6] Mampuya WM. Cardiac rehabilitation past, present and future: an overview. Cardiovasc Diagn Ther. 2012;2(1):38-49
[7] Zwisler AD1, Soja AM, Rasmussen S, Frederiksen M, Abedini S, Appel J, et al. Hospital-based comprehensive cardiac rehabilitation versus usual care among patients with congestive heart failure, ischemic heart disease, or high risk of ischemic heart disease: 12-month results of a randomized clinical trial. Am Heart J.
2008;155(6):1106-1113
[8] Lavie CJ, Milani RV. Cardiac rehabilitation and exercise training in secondary coronary heart disease prevention. Prog Cardiovasc Dis. 2011;53(6):397-403
[9] Booth FW, Roberts CK, Laye MJ. Lack of exercise is a major cause of chronic diseases. Compr Physiol. 2012;2(2):1143-1211
[10] Kim KH. The increasing role of exercise rehabilitation. J Exerc Rehabil. 2013;9(3):337
[11] Brolinson PG, Elliott D. Exercise and the immune system. Clin Sports Med. 2007;26(3):311–319
[12] Brooks GA FT, Baldwin KM. Exercise Physiology. 4th Ed. McGraw-Hill; New York: 2005
[13] Squires RW, Gau GT, Miller TD, Allison TG, Lavie CJ. Cardiovascular rehabilitation: status, 1990. Mayo Clin Proc 1990;65(5):731-755
[14] Thomas RJ, King M, Lui K, Oldridge N, Pina IL, Spertus J. AACVPR/ACC/AHA 2007 performance measures on cardiac rehabilitation for referral to and delivery of cardiac rehabilitation/ secondary prevention services. J Cardiopulm Rehabil Prev. 2007;27(5):260-290
[15] Smith SC, Allen J, Blair SN, Bonow RO, Brass LM, Fonarow GC, et al. AHA/ACC guidelines for prevention for patients with coronary and other atherosclerotic vascular disease: 2006 update endorsed by the National Heart, Lung, and Blood Institute. JACC. 2006;47(10):2130-2139
[16] Taylor RS, Unal B, Critchley JA, Capewell S. Mortality reductions in patients receiving exercise-based cardiac rehabilitation: how much can be attributed to cardiovascular risk factor improvements? Eur J Cardiovasc Prev Rehabil. 2006;13(3):369-374
[17] Milani RV, Lavie CJ, Mehra MR. Reduction in C-reactive protein through cardiac rehabilitation and exercise training. J Am Coll Cardiol. 2004;43(6):1056-1061
[18] Myers J, Prakash M, Froelicher V, et al. Exercise capacity and mortality among men referred for exercise testing. N Engl J Med 2002;346:793-801
[19] Balady GJ, Williams MA, Ades PA, Bittner V, Comoss P, Foody JM, et al. Core components of cardiac rehabilitation/secondary prevention programs: 2007 update: a scientific statement from the American Heart Association Exercise, Cardiac Rehabilitation, and Prevention Committee, the Council on Clinical Cardiology; the Councils on Cardiovascular Nursing, Epidemiology
and Prevention, and Nutrition, Physical Activity, and Metabolism; and the American Association of Cardiovascular and Pulmonary Rehabilitation. Circulation. 2007;115 (20):2675- 2682
[20] Allison TG. Improving weight loss in cardiac rehabilitation. Circulation. 2009;119(20):2650-26 52
[21] Lavie CJ, Milani RV. Cardiac rehabilitation, exercise training, and psychosocial risk factors. J Am Coll Cardiol. 2006;47(1):212-213
[22] Newman AB, Simonsick EM, Naydeck BL, Boudreau RM, Kritchevsky SB, Nevitt MC, et al. Association of long-distance corridor walks performance with mortality, cardiovascular disease, mobility limitation, and disability. JAMA. 2006;295(17):2018-2026
[23] Wenger N. Cardiac rehabilitation. Cardiovascular Prevention and Rehabilitation. 2007 springer
[24] Araya-Ramírez F, Briggs KK, Bishop SR, Miller CE, Moncada-Jiménez J, Grandjean PW. Who is likely to benefit from phase II cardiac rehabilitation?
J Cardiopulm Rehabil Prev. 2010;30(2):93 100
[25] Audelin MC, Savage PD, Ades PA.
Exercise‐Based Cardiac Rehabilitation for Very Old Patients (≥ 75 Years): focus on physical function. J Cardiopulm Rehabil Prev. 2008;28(3):163-173
[26] Achttien RJ, Staal JB, Van der Voort S, Kemps HM, Koers H, Jongert MW, et al. Practice Recommendations Development Group. Exercise-based cardiac rehabilitation in patients with coronary heart disease: a practice guideline. Neth Heart J. 2013;21(10):429-438
[27] Austin J, Williams R, Ross L, Moseley L, Hutchison S. Randomised controlled trial of cardiac rehabilitation in elderly patients with heart failure. Eur J Heart Fail. 2005;7(3):411-417
[28] Shabani R, Gaeini AA, Nikoo MR, Nikbackt H, Sadegifar M. Effect of cardiac rehabilitation program on exercise capacity in women undergoing coronary artery bypass graft in Hamadan- Iran. Int J Prev Med. 2010;1(4):247-251
[29] Fiorina C, Vizzardi E, Lorusso R, Maggio M, De Cicco G, Nodari S, et al. The 6-min walking test early after cardiac surgery. Reference values and the effects of rehabilitation program. Eur J Cardiothorac Surg. 2007;32(5):724–729
[30] Vincent KR, Braith RW, Feldman RA, Kallas HE, Lowenthal DT. Improved cardiorespiratory endurance following 6 months of resistance exercise in elderly men and women. Arch Intern Med. 2002;162(6):673–678
[31] Beatty AL, Schiller NB, Whooley MA. Six-minute walk test as a prognostic tool in stable coronary heart disease: data from the heart and soul study. Intern Med. 2012;172(14):1096-1102
[32] Hung CH, Huang HC, Chen HC, Lin SC, Lun LH. The Effects of Short-term Cardiac Rehabilitation on Post-CABG Patients’ Fitness. IPCBEE. 2012;45(15):74-78
[33] Ragawanti P. Effect Of Cardiac Rehabilitation Programs On Functional Capacity Of Post Coronary Revascularization Patient Using Six Minute Walk-Test. Folia Medica Indonesiana. 2014;50(2):86-91
[34] Craciun L, Avram A, Avram C, Sarau C, Iurciuc S, Iurciuc M, et al. Revascularized coronary patients: benefit of cardiac rehabilitation program. TMJ. 2011;61(1-2):13-17
[35] Hashmi FA, Sheikh M, Tipu FI Patients’ perceptions and beliefs contributing to non-intention to attend cardiac rehabilitation program: a local perspective. Pak. j. rehabil. 2016;5(1):11-17