
ABSTRACT
OBJECTIVES
The purpose of this study is to ferret out the immediate results of traction or mobilization in neck pain patients and to determine which one is more effective.
STUDY DESIGN
An Experimental study.
STUDY SETTINGS & PARTICIPANTS
The study was conducted in outpatient departments of tertiary care hospitals and clinics having well developed physiotherapy center. The participants include individuals having upper extremity pain and numbness and have three out of four cervical nerve compression test positive.
INTERVENTIONS
Treatment was given for three days in a week for a consecutive period of two weeks which includes traction and cervical mobilization techniques of Mulligan.
OUTCOME MEASURES
The outcome was measure using VAS and Neck Disability index scale. The data was analyzed by using SPSS version 20
RESULTS
Patients (N=50) were screened out of which 30 were found eligible. The effect of traction and mobilization in the treatment of cervical radiculopathy patient was same. Both the interventions were found to be equally effective in reducing the disability and pain of the patient.
CONCLUSIONS
This study has concluded that the effects of traction and mobilization in the treatment of cervical radiculopathy patient were same. Both the interventions were found to be equally effective in reducing the disability and pain of the patient.
Keywords
Cervical Spine, Neck Disability Index (NDI), Visual Analog Scale(VAS), Natural Apophyseal Glides (NAGS), Sustained Natural Apiphyseal Glides (SNAGS), Manual Traction.
Ali Farhad
Lecturer
Ziauddin College of Physical Therapy
Ziauddin University
Zainab Abdul Razzak
Physiotherapist
Batwa hospital Karachi
Bibi Sobia
ADPT Student
Ziauddin College of Physical Therapy
Ziauddin University
Saad Saleem
Assistant Professor
Ziauddin College of Physical Therapy
Ziauddin University
Fareeda Shaheen
Consultant Physiotherapist
Sindh Government Hospital Karachi
[Farhad A, Razzak ZA, Sobia B, Saleem S, Shaheen F. Comparing the Effects of Cervical Traction and Cervical Mobilization in the treatment of Cervicogenic Headache.Pak. j. rehabil. 2015;4(2):21-25]
INTRODUCTION
In cervical spine, the most common symptoms are pain and discomfort that may occur due to reduce disc spaces between the cervical vertebrae, muscular weakness or trauma1, often caused by damage in the vicinity of the root of a spinal nerve. The medical term for this cervical condition is known as cervical radiculopathy. Cervical nerves leave the cervical spine (neck) at each level, excluding the last one(C7) and then branch out to offer muscles of upper limb that enables the shoulders, upper arms, arm, muscle of hands and fingers to function. These nerves bring sensory and motor fibers to the skin and muscles that provide consciousness. When any nerve root in the cervical spine is irritated through firmness or inflammation, the symptoms can radiate along that nerves pathway into the arm, forearm, hand and fingers. The patient’s specific cervical radiculopathy symptoms depend on nerve which is definitely be affected. The most common causes include; cervical herniated disc, cervical spinal stenosis and cervical degenerative disc disease.
It may also occur due to heavy manual works, seated and sedentary life style and may also be due to improper posture. The symptoms of cervical pain often last for prolonged periods of time or in some cases, over the entire life. The symptoms include neck pain, headache, parasthesia, numbness and scapular pain 2-5. Neck disorders are difficult to cure and sometimes it become worse, therefore emphasis on the primary prevention is necessary.
There are three main reasons for neck disorders; the load on the neck structures is maintained for prolonged periods of time, and the need of stabilization of the neck-shoulder region when working with the arms, Jobs that required high concentration which induces an increased activity in neck muscles and degenerative changes that occur in vertebrae due to the process of aging which causes an increase in pressure on nerve due to the
reduction of spaces between vertebrae leading to radiculopathy6.It is also likely that the rate of degeneration increases as a result of physical demands of the job.
The cervical vertebrae provide a bony covering to the spinal cord from which the cervical nerves arises on both the sides. These nerves leave the cervical spine from an opening known as foramen and travel down to neck, upper back and arm.
Cervical radiculopathy is a compression of the cervical nerve due to the reduction of spaces between the cervical vertebras that causes pain and uneven sensation at the areas of the upper extremity depending on where the broken roots are supplying 2,7. The nerve travels into neck, upper limbs and arm. It is a painful condition due to the pinching of nerve as it leaves the spinal cord. The pinching of the nerve is caused either by the degenerative bony spurs arising from the neck or by herniated disc material.
In Cervical radiculopathy, pain travels down the arm in the area of the nerve supply. Pain is usually sharp in nature. Individual can also suffer “pins and needles” sensation or even some time may be complete numbness. In addition, there may be muscular weakness with certain activities.
Treatment of cervical radiculopathy includes; pain medications, corticosteroids (powerful anti-inflammatory drugs) or non-steroidal pain medication like ibuprofen.
Physiotherapy interventions include; traction and cervical mobilization, and other modalities that are heat and cold to reduce pain.
Mobilization also known as non thrust manipulation is a commonly used treatment for patients with a variety of neuro-musculoskeletal disorders as explained by Maitland 1985.It is passive, skilled manual therapy technique applied to joints and related soft tissues at varying speeds and amplitudes using physiologic and accessory motions for therapeutic purposes8. It is used to detect and treat soft tissues and joint structures for the reason of modulating pain, increasing range of motion (ROM), plummeting or eliminating soft tissue inflammation; inducing relaxation, improving contractile and non-contractile tissue repair, stability, facilitating movement, and improving joint function.
Joint mobilization of the neck includes stabilizing one bone of the joint while the other bone is moved into the realm of the joint play. Joint mobilization of the cervical spine is a very delicate technique that requires great skills as the range of the joint play is very small. It is important to perform the joint play very carefully and attentively. Joint mobilization plays a pivotal role in the treatment of both hypomobility and pain which is evident from various research studies.
Mulligan techniques are modern techniques and are very much effective in the treatment of cervicogenic headache. Nowadays, these techniques are precisely used to mobilize the spine of a patient having vertebral joint problem8. Mulligan provided three best techniques that are NAGS, SNAGS and Reverse NAGs to treat the patient with cervicogenic headache9,10. Numbers of studies have provided the evidence that these techniques are providing beneficial support in improving the pain and neck disability of a patient with cervical vertebrae problems. The effect of Mulligan’s technique and traction along with other conventional Physical Therapy modalities like Trans-Cutaneous Electrical Nerve Stimulation with Hot Packs and Ultrasound Therapy are found to be effective in the treatment of cervical patient but the effectiveness of Mulligan’s techniques and Traction alone along with the conventional Physical Therapy modalities are the subject which was untouched by the researchers yet and it is for this reason, the current study is based on the comparison of these two intervention strategies that is Traction and Mulligan’s Techniques in the treatment of cervicogenic headache.
Traction of spine is a technique through which a pressure from the spinal nerves can be relieved by pulling the vertebrae a part from each other thereby causes the stretching of nerve, ligaments and muscle and also reduces adhesion in the dural space10-13. At low intensity it is used to stretch the spinal muscles as well. Normally a force of 20-30 pounds is required. It can be done either manually or mechanically. Mechanically it is done via using a large range of machineries whereas manually it is usually done by medical or rehabilitation expert.
Traction allows the facet joints to slides thus causes increase in blood supply and relieves pressure on the spinal cord, its vessels and nerve roots11,14. The increase in blood supply allows the drainage of chemical substance that cause inflammation and pain whereas it also decreases the nervous excitability which is also a cause of pain.
METHODOLOGY
This was an experimental study design. Subjects were randomly selected and were distributed into two groups, for Group-1 subjects were treated with manual mobilization at cervical level while the other Group-2 was treated by manual traction program. Mulligan techniques; NAGs, SNAGs and Reverse NAGs were used as an intervention technique for patients from Group 1. The effectiveness of the treatment given was measured by using two different kinds of scales. The first was Visual Analog Scale and the second was the Neck Disability Index Questionnaire. A pain diagram was also used to locate the area of pain. All these forms were to be filled by the participants after the treatment session and the result were measured to find out the effectiveness of the treatment. The intervention was given for three days in a week for a consecutive period of two weeks, the participants were also be intervened by other pain relieving modalities like TENS and Ultrasound which remained the same for both the groups in order to extract out the effectiveness of traction and mobilization alone the other therapeutic interventions were kept same for both the groups. The patients from both the group also performed stretching and the strengthening exercises of the neck muscles in order to provide long term benefit of Physical Therapy interventions.
Sample Size and Selection of Data
30 patients were selected and randomly divided into two equal groups depending on the inclusion and exclusion criteria
Inclusion and Exclusion Criteria
Inclusion criteria includes; patients having upper extremity pain and numbness and 3 out of 4 clinical prediction rule positive i.e spurling test, distraction test, upper limb tension test and ipsilateral cervical rotation < 60. Exclusion criteria include cervial spine surgery, upper motor neuron disease, red flags like tumor, fracture and intake of medication like steroids.
Collection of Data
Assessment forms were used for data collection. The participants were required to fill the questionnaire in which their demographic information and past and present medical and surgical history were recorded. The participants were assessed according to the data provided by them and recruited randomly in one of the two groups for intervention strategies and then those participants were selected who met the inclusion criteria and who agreed to participate in the study with their informed consent.
Data Analysis Strategies
The outcome measures were VAS and NDI scale. The Data gathered was than analyzed by using VAS and NDI scale through SPSS version 16.
Ethics and Human Subject Issues
Ethical issues considered in my studies are following
1-Confidentiality statement was issued to all as an important aspect of personal security.
2- Beneficence of the study was identified before the conduction of the study and it was noted that the study does not have any such thing which could be harmful for the participants or have such thing which can overshadow its effectiveness and its patient-centered approach.
3-Consent from participants was taken as it is a legal procedure to ensure that a patient or client knows all of the risks and costs involved in treatment.
4- Participants had the right to with draw from study at any time.
5- Data collection and intervention in the hospital were done after taking permission from Head of department of Physiotherapy.
RESULTS
Patients (N=50) were screened, out of which 30 were found eligible having the mean age in years 34.36 ± 8.244 gave their consent to participate in the study. This included 14 male and 16 female participants. The mean age of male patients were 36.57 S ± 8.32 and the mean age of female patients was 32.43 ± 7.92.
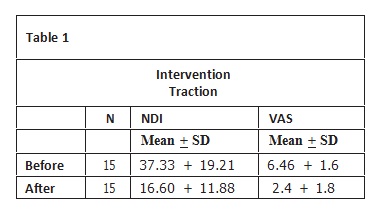
The result of the study has shown that in both groups the outcome of intervention was same, the mean VAS is reduced by 37% and mean NDI is reduced by 44% respectively by traction intervention and mean VAS is reduced by 38% and NDI is reduced by 46% respectively by mobilization intervention. The effect of traction in the handling of cervical radiculopathy patients as observed in the neck disability index questionnaire and on visual analog scale before and after the treatment is shown in table 1, which clearly indicated that the traction alone has a beneficial effect in reducing the disability and the pain of the patient, as before the intervention to group 1 the mean disability in patients due to cervical radiculopathy was 37.33% which reduced to 16.8% after the treatment.
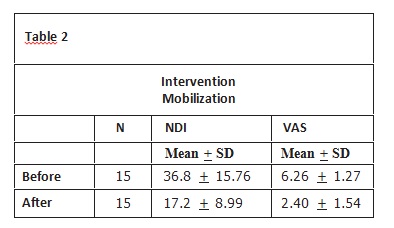
Similar effects were also seen in the intervention from mobilization, where the mean neck disability of the patients according to the neck disability questionnaire was 36.8% which reduced to the mean of 17.2% after the treatment of two weeks and the pain is reduced from 6.26 ± 1.27 to 2.40 ± 1.54 as shown in the table 2.
DISCUSSION
This Randomized Controlled Trial was done on patients having Cervical Radiculopathy to investigate the effect of Traction and Mobilization in the treatment of Cervical Radiculopathy. The subjects were divided into two groups. Group 1 was given traction and group 2 was treated by mobilization. The results were taken on Neck disability Index Questionnaire and on Visual Analog Scale which were filled by the patient after the treatment. The treatment was given for two weeks, three days per week and the results of treatment given were compared from day 1 and day 6. Although, results obtained show significant effect of reducing disability and pain in patients having Cervical Radiculopathy. There was no significant effect noticed to ferret out which one of the two treatments was more effective for Cervical Radiculopathy. The Neck Disability Index Questionnaire and the Visual Analog Questionnaire were filled by the patient each day after the treatment and the data of each day of treatment was obtained and calculated. The techniques used for cervical mobilization were NAGS, SNAGS and Reverse NAGS and traction. We used Manual Traction and teach the patients to perform self traction at the level of cervical vertebrae. The patients from both the groups were also intervened by neck strengthening exercises and the pain reliving modalities like TENS and Ultrasound. Studies have also shown that restoration of normal biomechanics of Thoracic Spine may also have effect on lowering the stress on Cervical Spine15. No effect of manipulation technique has been studied under this study and no intervention regarding Cervical manipulation were given to the patients under this study as considerable amount of care is required to give manipulation at the level of Cervical Spine16-18 . Strengthening of the scapulothoracic, deep neck flexors, cervical retraction as well as extension exercises were used for the treatment of Cervical Radiculopathy 19-20. Cervical retraction exercises were found effective in the treatment of neck pain and to improve the resting neck posture of the patient21, the exercise was also found effective in reducing the compression at cervical vertebrae22.
This study has supported the previous study regarding the conservative treatment of Cervical Radiculopathy and cervicobrachial pain23 -25.
CONCLUSION
This study has concluded that the effect of traction and mobilization in the treatment of cervical radiculopathy patient was same. Both the interventions were found to be equally effective in reducing the disability and pain of the patient. The disability of the patients was measured by neck disability index questionnaire and pain was assessed by Visual Analog Scale. The other conventional intervention that were used TENS, ultrasound and exercises were kept the same for both the group. The neck strengthening exercises including strengthening of scapulothoracic, deep neck flexors and scapular retraction were taught to both the groups and were asked to perform at home as a home rehabilitation programmed.
Indeed the effect of Cervical Radiculopathy is disabling and it is vital to carry out more researches on this topic
REFERENCES
[1] Wolff MW, Levine LA. Cervical Radiculopathies: conservative approaches to management. Physb Med Rehab Clin N Am. 2002;13:589-608.
[2] Young IA, Michener L, Cleland JA, et al. Manual Therapy, Exercise and Traction for patient with cervical radiculopathy. Phys Ther. 2009;89(7):632-642.
[3] Cloward RB. Cervical diskography: a contribution to the etiology and mechanism of neck, shoulder and arm pain. Ann Surg. 1959;150:1052-1064.
[4] Yoss RE, Corbin KB, Mac Carty CS, et al. Significance of symptoms and signs in localization of involved root in cervical disk protrusion. Neuro. 1957;7:673- 683.
[5] Persson LC, Carlsson JY. Headache in patient with neck shoulder arm pain of cervical radicular origin. Headache. 1999;39(3):218-224.
[6] Adams C. Outline of Orthorpeadics. London: Churchillivingston; 2002.
[7] Eubanks JD. Cervical radiculopathy: nonoperative management of neck pain and radicular symptoms. Amer Fam Phys. 2010;81(1):33-40.
[8] Mulligan BR. SNAGS, Published papers. IFOMPT Congress, 1988.
[9] Reid SA, Riwett DA. Sustained Natural Apophyseal Glides (SNAGS) are an effective treatment for cervicogenic dizziness, 2008.
[10] Takasaki H, Hall T. Cervical segmental motion induced by shoulder abduction assessed by magnetic resonance imaging. Spine. 2009;34(3):122-126.
[11] Maitland G, Hengeveld E, Banks K, English K. Maitland’s vertebral manipulation. 6th edition. Woburn, MA: Butterworth Heinemann; 2001.
[12] Bland JH. Disorder of the cervical spine, diagnosis, medical management. Philadelphia: WB, saunders; 1994
[13] Moeti P. Intermitent cervical traction for the treatment of cervical radiculopathy pain. J Ortho Sports Physther. 2001;31(4):207-213.
[14] Ellen Berg MR, Honet JC. Cervial radiculopathy. Arc Phys Med Rehab. 1994;75:342-352
[15] Valtonen E.J. Cervical traction as a therapeutic tool: a clinical analysis based on 212 patients. Scand J Rehab Med. 1970;2:29-36.
[16] Spurling RG, Scoville WB. Lateral rupture of the cervical intervertebral discs: a common cause of shoulder and arm pain. Surg Gynecol Obstet. 1944;78:350-358.
[17] Cleland JA, Childs JD, Mc Rae M. Immediate effect of thoracic manipulation in patient with neck pain: a randomized clinical trial. Man Ther. 2005;10:127–135.
[18] Haldeman S, Kohlbeck FJ, Mcgregor M. Risk factor and precipitating neck movement causing vertebrobasilar artery dissection after cervical trauma and spinal manipulation. Spine. 1999;24:785–794.
[19] Haldeman s, Kohlbeck, FJ Mc Gregor M. Stroke cerebral artery dissection, and cervical spine manipulation therapy. J Neurol. 2002;249:1098–1104.
[20] Haldeman S, McGregor M. Kohl beck FJ. Unpredictability of cerebrovascular ischemia ssociated with cervical spine manipulation therapy : a review of sixty-four cases after cervical spine manipulation. Spine. 2002;27:49 -55.
[21] Cleland JA, Whitman JM, Fritz JM, Palmer JA. Manual physical therapy, cervical traction, and strengthening exercises in patients with cervical radiculopathy: a caseseries. J Orthop Sports Phys Ther. 2005;35:802–811.
[22] Cleland JA, Fritz JM, Whitman JM, Heath R. Predictors of short-term outcome in people with a clinical diagnosis of cervical radiculopathy. Phys Therapy. 2007;87:1619-1632.
[23] McKenzie R. The cervical and thoracic spine: mechanical diagnosis and therapy. New Zealand: Spinal Publication Ltd; 1990.
[24] Abdulwahab SS, Sabahi M. Neck retraction cervical root decompression, and radicular pain. J Orthop Sport Phys Ther. 2000;30:4
[25] Joghataei MT, Arab AM , Khaksar H. The Effect of cervical traction combined with conventional therapy on grip strength on patients with cervical radiculopathy. Clin Rehab. 2004;18:879-887.