
ABSTRACT
BACKGROUND
Vitamin-D commonly known as Ergocalciferol (vitamin D2) & Cholecalciferol (vitamin D3) promotes the absorption and metabolism of calcium. Among children scarcity of vitamin D may cause rickets whereas osteomalacia both in adults and children having relevance with less circulating concentrations of 25OHD that is less than 20 nmol/L.
OBJECTIVE
To assess knowledge of undergraduate students about vitamin-D deficiency in various private sector universities of Karachi.
STUDY DESIGN
A cross-sectional study was conducted where structured questionnaire were distributed
STUDY SETTINGS & PARTICIPANTS
The targeted population was 100 subjects currently enrolled in medical universities.
RESULTS
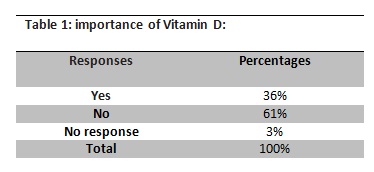
According to the descriptive analysis, 100% students were aware of the importance of Vitamin D. However, only 38% of them knew that the deficiency of Vitamin D can cause tiredness, low mood, muscle and bone pain. 64% knew the beneficence of exposure of 10-15% of sunlight.
CONCLUSION
Students of private medical universities are aware of Vitamin D deficiency and its importance but its implementation is absent.
Keywords
Osteomalacia, Rickets, Vitamin D deficiency, Osteoid, Trabecular Bone, Cholecalciferol, Ergocalciferol
Beenish Zafar
Visiting Faculty
Ziauddin College of Physical Therapy
Ziauddin University
Aysha Zia Qureshi
Pharmacist
Department of Pharmacy
Ziauddin Hospital
Sejaa Zafar
DPT Student
Ziauddin College of Physical Therapy
Ziauddin University
[Zafar B, Qureshi AZ, Zafar S. Assesment of Knowledge about Vitamin-D Deficiency among Undergraduate Students in Private
Sector University. Pak. j. rehabil.2015;4(2):26-31]
INTRODUCTION
Among children Vitamin D deficiency may cause rickets as well as osteomalacia both in adults and children. Rickets is illustrated as a delay or stoppage in the bone formation of long bones that inculcate the demolition and elimination of cartilage and the formation of osseous tissue in area that was previously filled with cartilages at their developmental ends1. In Osteomalacia, the demineralization of osteoid on the cortical surfaces occur and trabecular of the bone is coupled with broadened osteoid closure and existence of looser zones2. Altogether the fore-mentioned stipulations may be in confederation with hypocalcaemic fits, pain and paresis in the upper and lower extremities, respiratory, and cardio vascular structures. Reduced vitamin D, is also coupled with augmented menace of other diseases, as mainly osteoporosis, ailment of cardiovascular complex and various cancerous growth2. Quantifiable vitamin D insufficiency remained typical within various countries till the mid of previous century. Programs like strength training and upturns in the eminence of natural air have greatly repudiated osteomalacia and rickets from wide-ranging populace of Europe and North America3. Prevalence of rickets, on the other hand, remains despicably far above the ground in numerous regions of Asia, Middle East, and Africa3,4. The worldwide osteomalacia’s prevalence in adults is not so easy to measure for the reason that at present there are just a very few literatures available carrying relevant reports and chances that they remained nonspecific and set off unnoticed. Still, it is logical to presuppose that in areas wherever rickets is common in children, there are more chances of osteomalacia in adults, in-particular pregnant women and the elderly.
The long-lasting blood stream substance of vitamin D, 25-hydroxyvitamin D (25OHD), is an essential indicator of vitamin D inadequacy. The formation of this specific vitamin occurs in liver, imitates the vitamin D dispensing from integument and diet. There is a relationship of low circulating concentrations of 25OHD, usually less than 20 nmol/L (8 ng/mL; 2.5 nmol/L = 1 ng/mL) with rickets and osteomalacia.
The congregation of 25OHD in plasma is benefited to soft peculiar person at stake of vitamin D insufficiency disease, based upon the populace with speculated sufficiency of vitamin D supply 5.
There were notarization in recent past to classify vitamin D adequacy as blood stream 25OHD concentration >50 nmol/L (20 ng/mL), >75 nmol/L (30 ng/mL), >80 nmo/L (32 ng/mL) and >100 nmol/L (40 ng/mL)5. Additionally, there were entitlements to a tolerated level by recent safety data, as for the purpose of recapitulation in the recent upper intake level (UL) for cholecarciferol50 μg/day, to be acceptable in blood stream it can be gained by all nutritional resources5. Maintenance of normal blood pressure is the prime and important domain of Vitamin D as well as the maintenance of normal blood levels of calcium and phosphorous. Assimilation of calcium is also augmented by Vitamin D, which helps in the preservation and modulation of stronger bone. It is utilized, unaided or in addition with calcium, to boost bone mineral density and minimize the causes of fractures. In children, insufficiency of vitamin D ends up in rickets that causes skeletal deformities. While In adults osteomalacia is the main hallmark of its insufficiency which does not end up in bones weakness but of muscles too.
According to one study conducted across the community in Karachi, in 2012, the prevalence of Vitamin D deficiency and its correlates. A cross sectional study among randomly selected communities was done for the determination of occurrence and risk factor of Vitamin D deficiency among females. Data was collected on the variables like housing construction, nutritional intake and sunlight exposure. Serum Vitamin D3 levels were calculated, along with it mean and SD values were also calculated. ANOVA and Chi-square were also used for auxiliary analyses of data. Out of 305 premenopausal females most of the females were vitamin D deficient .This was such a high prevalence observed in females in that specific community it was found out that for the incidence of conditions associated with the in appropriate levels of vitamin D there is always a requirement of an immediate action in regards of supplement intake3.
Another local study was done at Agha Khan University Hospital Karachi in 2012 about correlation of Vitamin D with sunlight exposure duration the advancement and validation of sunlight exposure measurement questionnaire (SEM-Q) which was used in grown-up populace dwelling in Pakistan.
This study was developed to evaluate exposure to sunlight in healthy adults in Karachi. Fifty four healthy individuals were included according to their exposure to sunlight (high=17, moderate=18, low=19). The individuals who were the research subjects were asked to put on a dosimeter and spent time in the sunlight. The samples of the blood were taken for serum vitamin D. The coalition between the levels of vitamin D and average score was found to be 0.36(p= 0.01). It was concluded that the questionnaires about sunlight exposure measurement were efficient tools to make the most of in great epidemiological studies to calculate sunlight exposure4.
As per one international survey based study conducted at Hong Kong in 2006 on the subject of the knowledge of vitamin D and perceptions and attitudes towards sunlight among Chinese middle-aged and elderly women. The rationale of this study was to evaluate awareness about VitaminD among 547 middle-aged and aged women who were Chinese in origin but dwelling in Hong Kong, an interview survey through phone was done in which Computer Assisted telephone technique was used. A random sampling was done in the study to evaluate understanding of vitamin D amongst inhabitants by the side of marked threat of impaired vitamin D status, bones of poor health, and osteoporosis. The results revealed that most of the females were unaware regarding the function of sunlight in the production of vitamin D. There were little understanding about the function and sources of vitamin D. Most of the younger females were trying to avoid sunlight, although they had sufficient knowledge of vitamin D5.
One study was done through qualitative survey at Riyadh, Saudi Arabia with the topic knowledge, attitude and practice regarding vitamin D deficiency among female students in Saudi Arabia. Eight comprehensively one-to-one and one focused group semi-structured interviews carried out, evaluated and analysed. Contestants had inadequate knowledge in relation to vitamin D and its scarcity. They reported imperfect sun exposure because of severe heat, edifying grounds for covering the body, and the cultural issues as well due to which there was difficulty in getting sunlight exposure6.
Another cross-sectional descriptive study was done at a hospital in Oslo, Norway, with a population of multiple ethnicities with the subject to inspect vitamin D gradients in patients with headache, pain in soft and hard tissues, and tiredness in the absence of any obvious cause. A general practitioner (GP)referred 572 patients who came up with the complain of muscular and bone pain, headache, or tiredness, for assessment of hypo vitaminosis D. Inclusion criteria was both male and females from all age groups, the patients’ inhabitant countries were: South-East Asia, America and Europe (n = 83), Norway (n = 249), and the Middle East, South Asia and Africa (n = 240) since the actual conclusion was Vitamin D levels (25-hydroxyvitamin D) in nmol/L. and it was found out the diagnosed hypo vitaminosis D (25-hydroxyl vitamin D <50 nmol/L) recognized in 58% of patients whereas rest of the other were with negligible seasonal differentiation of levels. Every second women from these countries had vitamin D level below 25 nmol/L. vitamin D levels were lower in patients who had headaches with comparison to the sufferers with other signs and symptoms. 15% of the person with the vitamin D levels< 50 nmol/L reported headaches, in comparison to 5% of individuals with normal vitamin D levels. Therefore, the study revealed a high incidence of hypo vitaminosis D in patients with non-specific muscles and bone pain, or tiredness or headaches for whom the general physician inferred a lowvitamin D level7.
One of the study that was conducted by the Occupational and Social Medicine unit at University of Gottingen, Germany that was published in 2010,294 patients were included through a randomized double blind trials of supplements of vitamin D with compare to the placebo for the treating chronic pain conditions in adults. Two authors, who were reviewing, autonomously chose the studies for inclusion,evaluated procedural quality, and hauled out data. Analysis in a group was not done due to scarcity of data with the previous knowledge of that Vitamin D is formed in the dermis after its exposure to sun-light and can also be attained all the way through food. The deficiency of Vitamin D has recently been associated with variety of diseases together with chronic pain. Circumstantial and observational evidence recommends that in the etiology of chronic pain conditions there may be a role of vitamin D deficiency8.
METHODOLOGY
Study Participants & Settings
Respondents from undergraduate program of pharmacy and physiotherapy domains were selected.
Study Design
Cross-Sectional study. Sampling Technique Randomized sampling technique was used.
Sample Size
100 subjects were selected from Private Universities in Karachi. The prepared questionnaire regarding the awareness on the topic of deficiency of vitamin D and the role of sunlight exposure in vitamin D deficiency is provided to respective students including Pharmacy and physiotherapy program.
Inclusion Criteria
1st, 2nd, 3rd and final year students of their respective graduate programs were included in this study.
Exclusion Criteria
Teachers, Medical professionals and general public were not included in this study.
Data Collection Procedure
Randomized survey after distributing the questionnaire
Ethical Aspect
Ethical research committee has approved.
Data Analysis Procedure
The collected data is analyzed to conclude the knowledge level of these students in relation to the awareness of vitamin D deficiency and sunlight exposure. To analyze the results SPSS was used
Data Collection Tools
The selected subjects were guided properly to fill the questionnaire according to the academic knowledge provided in their respective universities or the information they acquire from other academic sources.
RESULTS
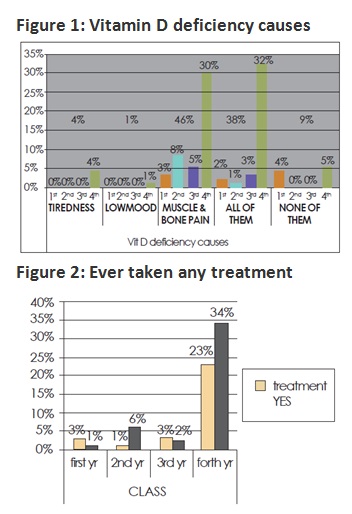
The mean age of the Respondents was 21.67 years + 1.393. 36% students know that Vitamin D is important for health and is required for calcium absorption while 3% had no knowledge about what Vitamin D does as shown in table 1. 38% of the students had the knowledge that deficiency of vitamin D causes tiredness, muscle pain and low mood as shown in Figure 1. 18% took Vitamin D supplements, 84% took vitamin D enriched foods like milk, fish, oil, egg and so many. 36% experienced muscle pain and fatigue for more than a week. 43% took treatment for pains and fatigue figure 2, 11% took analgesics, 7% took physiotherapy treatment, 6 % took vitamin D supplements and 6% took sun exposure.4% said vitamin D deficiency can cause tiredness, 1% said low mood,46% said it causes muscle pain and fatigue while 38% said that its deficiency causes all of them figure 2. About 42% liked to go into the sun, 51% took sunlight exposure in the afternoon while 44% took in the morning, 64% know that early morning sunlight exposure for 10-15 is beneficial for health.
DISCUSSION
Luminosity of the sun rays radically inflict to diurnal yielding of vitamin D, not only that just 10 minutes of sunlight exposure is considered as sufficient to put off deficiencies. Two formulations of vitamin D:ergocalciferol (vitamin D2) and cholecalciferol (vitamin D3). Vitamin D3 is engineered in epidermis of human skins after its exposure to ultraviolet B (UVB) rays from solar resourses 6,8.
One of the principal nutrients of the human body is Vitamin D. This study’s contemplation is to embed many health benefits of vitamin D, part that the deficiency of vitamin D plays in increasing peril of many general and severe diseases, together with few commonly occurring cancers, adult onset diabetes, cardiovascular disease, and osteoporosis9,11. This important nutrient has the contribution to healthy bones and to control amount of calcium in the blood. But it is really very difficult to obtain the regular prescribed amount of vitamin D12-13. Therefore vitamin D deficiency cases are increasing day by day. It is important to aware the people about Vitamin D sources and deficiencies causing severe outcome14,15. First of all, low cost far and wide vitamin D supplementation availability should be made possible. Secondly, genuine urges to identify some important resources of Vitamin D and implementing it in the daily diet7,16. Unfortunately in today’s modern era still the health care professionals are not well trained17.
From the sample size out of 100 every student regardless of his class had the knowledge about Vitamin D , all of them knew that Vitamin D is required for calcium absorption while the study conducted at Prince Sultan University Riyadh the students were not aware of Vitamin D and its importance 3,6,18,19.
Our study revealed that very lesser amount of students i.e. 38% had the awareness that Vitamin D deficiency can cause low mood, tiredness ,muscle pain and fatigue while the interventional study conducted at Oslo ,Norway and it had been found out that Vitamin D deficiency can cause low mood, tiredness, myalgia and fatigue 7,20,21.
In this study only 6 % students responded that for muscle pain and fatigue they took Vitamin D supplements or sunlight exposure while the study conducted at Occupational and Social Medicine unit, University of Gottingen Germany with the purpose of demonstrating the association of vitamin D supplements and sunlight exposure with myalgia and fatigue 9,22.
Students had the knowledge that early morning sunlight exposure for 10-15 minutes is essential for body’s daily vitamin D requirement which had already been proven by the study conducted by Agha khan university hospital, but this duration is for maximum body exposure if people are going in sun with just hands, feet and face exposed than this duration is very less23-25.
CONCLUSION
Students of pharmacy and physiotherapy of Pakistani universities are more aware of Vitamin D and its importance that it causes low mood, tiredness, myalgia and fatigue and one can overcome it by taking vitamin D supplements and sun exposure but knowledge about the proper timings and duration is still lacking.
RECOMMENDATION
Since students are aware of importance of vitamin D and the effects that its deficiency can cause so they can run a campaign initially on a small scale and later on larger scale that initially instead of taking analgesics for muscle and bone pains people should start taking vitamin D through the natural resources.
And as the lab tests for Vitamin D levels are so expensive so, if it will be the first line of remedy, people get benefit out of it than it may be cost effective.
REFERENCE
[1] Smith Y. What is Vitamin D? [Internet]. 2015 [updated May 2013, cited 2013]. Available from:h t t p : / / w w w . n e w s – m e d i -cal.net/health/What-is-Vitamin-D
[2] The free dictionary. [internet]. [cited 2014]. Available from: http://medical-dictionary.thefreedictionary. com/vitamin+D+deficiency
[3] Khan AH, Iqbal R, Naureen G, Dar FJ, Ahmed FN. Prevalence of vitamin D deficiency and its correlates: results of a community-based study conducted in Karachi, Pakistan. Arch Osteopo. 2012;7(1-2);275-82.
[4] Humayun Q, Iqbal R, Azam I, Khan AH, Siddiqui AR, Baig-Ansari N. Development and validation of sunlight exposure measurement questionnaire (SEM-Q) for use in adult population residing in Pakistan. BCM Public Health. 2012;10:1186-1471
[5] Kung AW, Lee KK. Knowledge of Vitamin-D and perceptions and attitudes towards sunlight among Chinese middle-aged and elderly women: a population survey in Hong kong. BMC Public Health. 2006;6:226
[6] Christie FT, Mason L. Knowledge, attitude and practice regarding vitamin D deficiency among female students in Saudi Arabia: a qualitative exploration. Int J Rheum Dis. 2011;14(2):22-29.
[7] Mason L, Moore RA, Edwards JE, McQuary HJ, Derry S, Wiffen PJ. Systematic review of efficacy of topical rubefacients containing salicylates for the treatment of acute and chronic pain. BMJ. 2004; 328(7446):995.
[8] Straube S, Derry S, Moore RA, McQuay HJ. Vitamin D for the treatment of chronic painful conditions in adults. Cochrane Database Syst Rev. 2012;1.
[9] Pannu PK, Zhao Y, Soares MJ. Reductions in body weight and percent fat mass increase the vitamin D status of obese subjects: a systematic review and meta regression analysis. Nutr Res. 2014,;36(3):201-213.
[10] BinSaeed AA, Torchyan AA, AlOmair BN, AlQadhib NS, et al. Determinants of vitamin D deficiency among undergraduate medical students in Saudi Arabia. Eur J Clin Nutr. 2013;69(10):1151-1155.
[11] Touvier M, Deschasaux M, Montourcy M, Sutton A,et al. Determinants of vitamin D status in caucasian adults: influence of sun exposure, dietary intake, sociodemographic, lifestyle, anthropometric, and genetic factors. J Invest Dermatol. 2013;135(2):378-388.
[12] Zittermann A, Ernst JB. Foods and Dietary Supplements in the Prevention and Treatment of Disease in Older Adults. USA: Elsevier; 2013.
[13] Caillet P, Jaglal SB, Laforest L, Chapurlat R, et al. Impact of vitamin D supplementation on health-care use in a 25-hydroxyvitamin D-tested population in France: a population-based descriptive cohort study. Public Health Nutr. 2013;18(3):554-561.
[14] Smolensky MH, Sackett-Lundeen LL, Portaluppi F. Nocturnal light pollution and underexposure to daytime sunlight: complementary mechanisms of circadian disruption and related diseases. Chronobiol Int. 2012;32(8):1029-1048.
[15] Pereira-Santos M, Costa PR, Assis AM, Santos CA, Santos DB. Obesity and vitamin D deficiency: a systematic review and meta-analysis. Obes Rev. 2012;16(4):341-349.
[16] Mow TC, Stokes CM, Sutherland AG. Patients presenting with fractures are likely to be vitamin D deficient: are we getting enough sun? ANZ J Surg. 2013;85(10):766-769.
[17] Alkerwi A, Sauvageot N, Gilson G, Stranges S. Prevalence and correlates of vitamin D deficiency and insufficiency in Luxembourg adults: evidence from the observation of cardiovascular risk factors (ORISCAV-LUX) Study. Nutrients. 2013;7(8):6780-6796.
[18] Jungert A, Neuhäuser-Berthold M. Sex-specific determinants of serum 25-hydroxyvitamin D3 concentrations in an elderly German cohort: a cross-sectional study. Nutr Metab. 2013;12(1):2.
[19] Moran LJ, Teede HJ, Vincent AJ. Vitamin D is independently associated with depression in overweight women with and without PCOS. Gyneco Endocrino. 2014;31(3):179-182.
[20] Black LJ, Jacoby P, Ping-Delfos WCS, Mori TA, et al. Low serum 25-hydroxyvitamin D concentrations associate with non-alcoholic fatty liver disease in adolescents independent of adiposity. J Gastroent Hepatol. 2014;29(6):1215-1222.
[21] Kimlin MG, Lucas RM, Harrison SL, van der Mei I, et al. The Contributions of solar ultraviolet radiation exposure and other determinants to serum 25-hydroxyvitamin D concentrations in Australian adults: the AusD study. Am J Epidemiol. 2014;179(7):864-874.
[22] Arash H, Holick MF. Optimize dietary intake of vitamin D: an epigenetic perspective. Curr Opi Clin Nutr Metabol Care. 2012;15(6):567-579.
[23] Sharmaine A, Abdalqader MA, Ghazi HF, Hasan TN. Knowledge regarding Vitamin D among private University students in Malaysia. Ann Nutr Disord Ther. 2014;1(2):1008-1013.
[24] Kung AW, Lee KK. Knowledge of vitamin D and perceptions and attitudes toward sunlight among Chinese middle-aged and elderly. Asian J Pharm Clin Res. 2014;9(1):308-313.
[25] Ho-Pham LT, Nguyen MT. Survey on knowledge and attitudes on Vitamin D and sunlight exposure in an urban population in Vietnam. J Asean Fed Endocr Soc. 2012;27(2):55-59.