
ABSTRACT
OBJECTIVES
Evaluate the effectiveness of high frequency transcutaneous electrical nerve stimulation at the tender point of upper cervical as adjunctive therapy of fibromyalgia patients.
STUDY DESIGN
It is a randomized control trial study design
STUDY SETTINGS & PARTICIPANTS
The study was conducted on 30 participants with the age group of 20-65 years upon females with clinically diagnosed condition of fibromyalgia in tertiary health care center.
METHODS
In this study, all the participants were divided in to two groups, group 1 (N=15) and group 2 (N=15). Group 1(N=15), received TENS with exercise therapy and group 2 (N=15), received only exercise therapy. Both the groups received 4 sessions per week and in whole the participants were attended 32 sessions in eight weeks of duration.
RESULT
TENS with exercise group 1 (N=15) had a greater pain reduction (6.0±1.13) compared with only exercise group 2 (N=15) (6.2±1.1). There was no such huge difference between both the treatments program, but group 1 shows more improvement in the pain reduction, work performance, stiffness, fatigue, anxiety, and depression.
CONCLUSION
Both the groups demonstrate significant results in pain fatigued, anxiety, work performance, and depression.
KEY WORDS
High Frequency Transcutaneous Nerve Electrical Stimulation, Fibromyalgia, Exercise Therapy, Tender Point, Pain, Cervical
Sania Hassan Ali
Senior Lecturer
Ziauddin College of Physical Therapy
Ziauddin University
Syeda Amool Sakeena Rizvi
Lecturer
Ziauddin College of Physical Therapy
Ziauddin University
Muhammad Usman Khan
Senior Lecturer
Ziauddin College of Physical Therapy
Ziauddin University
[Ali SH, Rizvi SAS, Khan MU. Effectiveness of high frequency transcutaneous electrical nerve stimulation at the tender point of upper cervical as adjunctive therapy of fibromyalgia patients. Pak. j. rehabil. 2014;3(1):29-33]
INTRODUCTION
Traditionally, fibromyalgia was frequently termed as fibrositis and categorized as an inflammatory musculoskeletal disease. Fibromyalgia (FM) is a common painful rheumatic syndrome associated with tender points, sleep disturbance, chronic fatigue, headache, anxiety, depression, and bowel symptoms1.
Fibromyalgia is the second most common disorder observed by rheumatologists after osteoarthritis. In 1990, American College of Rheumatology (ACR) classification criteria for the diagnosis of fibromyalgia required an essential tenderness on pressure (tender points) in at least 11 of 18 specified sites and the presence of extensive pain for analysis but the proper diagnosis in the recent probable changes to these investigative criteria has included the implementation of the Wide spread Pain Index (WPI) and the Symptom Severity (SS) index to enhancement the prior ‘tender point’ criteria. Furthermore, the healthy professional typically a Rheumatologist, will eliminate other circumstances first and then if Fibromyalgia is assumed, conduct the tender point, WPI and SS tests. Even more evidences provided occurrence of Fibromyalgia, that is, about 2% in the United States, including 3.4% of women and 0.5% of men2,3. So, according to these statistics the fibromyalgia is familiar in women as compared to the men.
Silvia et al stated in the study that, there is an association of sleep disturbance, anxiety, and overall physical functional activities4. The study accomplished that disturbed sleep increases pain, worsens physical functioning and worse physical functioning increases depression. This indicates that other relationships between symptoms exists such as, pain interfering with sleep, lack of sleep resulting in anxiety and increased pain and anxiety interfering with sleep5.The American College of Rheumatology defines fibromyalgia criteria to include pain of at least three months duration above and below the waist bilaterally, axial skeletal pain, and 11 of 18 discrete tender points6.Another authors conformed in the studies that, the environmental triggers including, physical trauma and psychosocial stressors, may be involved in the pathophysiology of fibromyalgia7,8.
Therefore, living well with fibromyalgia – the valuable approach is self-management strategies that includes regular exercise; such as, yoga or stretching exercise, medications, eating a healthy and balanced diet, relaxation exercises (breathing or aerobic exercises) and good sleep9. Furthermore, recent studies recommended that, the treatment of fibromyalgia patients is based upon the interdisciplinary approach10, with physical therapy, pharmacological, cognitive behavioral and educational interventions. Eventually, the use of yoga in the management of fibromyalgia is essential5.In the field of physical intervention, physical therapy offers a great variety of therapeutic modalities and exercises that can be used to deal with fibromyalgia11.
Pain is constant and a key symptom of fibromyalgia for which exercise is generally endorsed, but can sometimes induce pain. The frequent treatment for musculoskeletal pain is transcutaneous Electrical Nerve Stimulation (TENS). Davis11 and Okonkwo et al12, independently found evidence about inducing negative mood and stress exposure could worsen pain ratings in patients with fibromyalgia. TENS is an electrotherapeutic method used for pain management that has been examined in the medical journalism since its inception by Wall and Sweet in 196713.
TENS may differentially affect a multiplicity of outcomes related to pain. Pollster having expertise in clinical pain research, proposed guidelines for the measurement of pain treatment outcomes beneath Initiative on Methods, Measurement and Pain Assessment in Clinical Trials (IMMPACT) that focuses on foundation outcome domains, such as, pain, physical function, emotional function, comprehensive improvement, symptoms and unsympathetic effects14.
In a clinical trial, patients with neuropathic pain, TENS reduces allodynia when compared with a placebo intervention. Similarly, patients with fibromyalgia and osteoarthritis, deep tissue hyperalgesia (pressure pain threshold measure) were also reduced15.
In other words, Transcutaneous electrical nerve stimulation is an electro physical agent, capable of inducing electro analgesia by means of pulsed electrical current delivered over the skin surface16. This definition is consistent with the historical association in the scientific and clinical literature between the terms transcutaneous electrical nerve stimulation and pain management, because the use of Transcutaneous electrical nerve stimulation therapy is fundamentally for the management of pain. Pain is by far the dominating symptom that prompts people to consult health-care practitioners. The medical approach to pain therapy is to offer drugs and if drugs are not successful, then surgery is usually taken into consideration17.
Transcutaneous electrical nerve stimulation (TENS) is often used for the treatment of pain. The low frequency, high-intensity TENS activates Aα and C fibers via the recruitment of descending inhibition mechanism. Low frequency TENS (<10Hz) seems to induce analgesia by inhibiting pain transmission through mu-opioid receptors at the spinal and supra spinal levels and it is more generally used for the treatment of chronic pain. Whereas, the high-frequency TENS present as the main mechanism of action for pain, relief by the gate control theory18. Furthermore, few clinical investigate application of high-frequency TENS in fibromyalgia hence its worth must be superiorly defined15,19.
In combination of electrotherapy, exercises play an important role. In the year 1988, various studies were published, claiming that the moderate-intensity to high-intensity aerobic exercise by approach of cycling and whole-body exercise for patients with fibromyalgia, the effects of moderate-intensity to high-intensity ergo meter cycling, found that the improvements in aerobic capacity, tender point pain threshold in the group that exercised three times a week for 20 weeks19. Additionally, the objective of the study is to investigate the efficiency of high frequency TENS at the tender point (upper cervical) at the adjunctive therapy in fibromyalgia patients
MATERIAL AND METHOD
Study Population and Duration
The time period of the study was 6 months, carried out in a tertiary care center, on females, ranging age between 35-65 years being diagnosed with fibromyalgia.
Study Design and Sample Size
It is an experimental study conducted on 30 participants with the present condition of fibromyalgia. All the participants were divided in to two groups, group 1 (N=15) and group 2 (N=15).
Sampling Technique
Data were collected by using simple random sampling technique.
Data Collecting Tool:
Tools were Assessment Form and Visual Analogue Scale (VAS).
Inclusive Criteria
Participants included females with the age bracket of 35-65 years, with clinically diagnosed condition of fibromyalgia, attending at tertiary care center. Informed consent forms were provided by all patients and the study was approved by the ethics committee.
Exclusive Criteria
The exclusion criteria of this study were males and those who were suffering from neurological deficit, fractures, recent surgery, and cardiovascular diseases. Additionally, any person with the history of pacemaker, seizure or chronic disorders was also excluded from this study.
Procedure
The data was collected on the female fibromyalgia participants with their verbal consent before participating in to the study. All participants were divided into two groups, group 1 (N=15) and group 2 (N=15). Both the groups received the same protocol of treatment that included neck exercises and static stretching of upper neck. The only difference between both the groups was that, group 1 received high frequency Transcutaneous electrical nerve stimulation (TENS) of more than 50 Hz for 20 minutes. The pain intensity was assessed on the VAS scale before and after completing the treatment procedure. In addition, other symptoms were also assessed, such as: depression, anxiety, fatigue, sleeps symptom, work performance and social life of the included participants with the revised Fibromyalgia Impact Questionnaire (FIQR). The same physical therapist made the initial and final assessment and led the treatment. Tender point on the upper trapezium muscle was selected for the TENS application and adjunctive therapy, since hyper analgesia in the muscle seen frequently in patients with fibromyalgia.
Data Analysis
Data was entered and analyzed on SPSS version 20. All qualitative variables were presented as frequency and percentages, whereas quantitative variables were presented as mean and standard deviation. To check the significance of both the treatment, Paired t-test was applied with P value less than 0.05 considered as significant.
Ethical Consideration
The data remained confidential and subjects were fully educated about the study objectives. A verbal consent was obtained from the participants after illuminating the study. Patient privacy and hygiene factor also maintained properly.
RESULTS
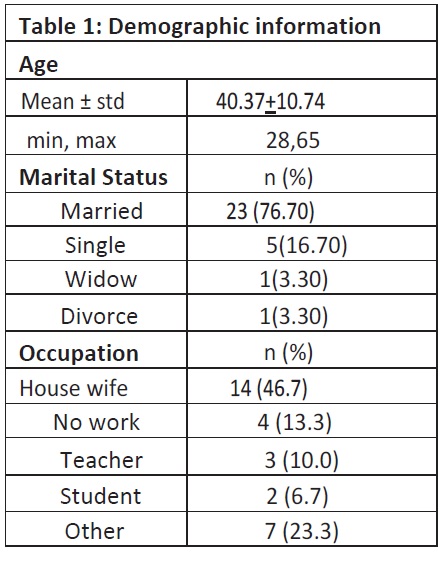
Inter-group baseline comparison was conducted for the variable pain. The data was analyzed which included mean, ± standard deviation, minimum and frequencies, maximum age, occupation and marital status. Groups (TENS and without TENS) were used as descriptive statistics to summarize the data.
The descriptive statistics of table I shows the minimum and maximum age mean ± SD (40.37±10.74) of both the groups (N=30) of the study. According to the marital status in the data, 76.7% were married women, 16.7% being single women whereas, 3.3% were widows and divorcees. Furthermore, according to the occupation 46.7% were housewives, 13.3% perform less work, 10% were teachers, 6.7% were students and 23.3% were belonging to other profession.
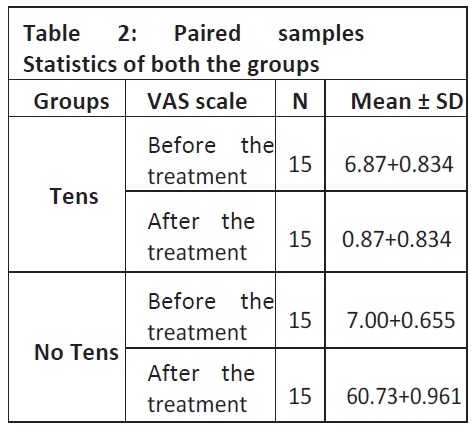
The expressive statistics (table II) shows a useful statistic for both groups 1 and 2. The tables show the pre-VAS and post VAS of the treatment efficiency. The sample size is 30, group 1 (N=15) and group 2 (N=15), female age ranges from 20 to 65 years.
Paired t-test applies with respect to groups. In group 1(N=15), Tens with exercise therapy – before the treatment, the VAS scale 6.87± 0.834 and after the treatment the VAS scale was 0.87±0.84 whereas, the group 2 (only exercise therapy) before the treatment 7.00± 0.655 and after the treatment the VAS scale 0.73± 0.96 was recorded respectively.
As table III shows the mean± SD of group 1 (N=15) is 6.00±1.134 and group 2 (N=15) was 6.26±1.16 by applying the paired sample test.
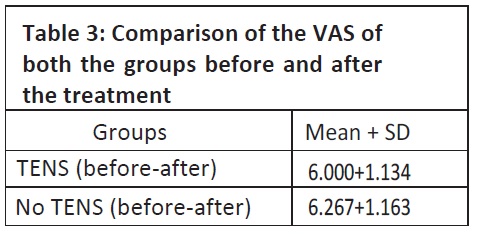
As the combination of both the groups, results, it shows significant consequences and there is no huge difference between both the treatment and the group 1 shows more significant results as compared to group 2 in the VAS scale and reducing the pain.
Ultimately, our results show improvement and in FIQR questionnaire also, we found healthier consequences in relation to depression, anxiety, fatigue, sleep symptoms, work performance and social life.
DISCUSSION
This study included exercise regime as an intervention, that comprised aerobic and static stretching exercises at the level of upper cervical region (trapezius and supraspinatus), given to two groups. From these two groups, group 1 has received high frequency TENS therapy along with the exercise regime that is combined therapy, while group 2 received only exercises.
In Physiotherapy, TENS has a traditional use in reducing pain. The procedure by which pain modulation occurs with the use of TENS is still unknown. In 1965, Melzack and Wall proposed the mechanism of the analgesia that is produced after the application of TENS, in the gate control theory20. Exercises play very important role in relieving pain in several chronic muscular conditions. To improve the Activity of Daily Livings (ADLs) and wellbeing in women, the supervised exercise program is found to be very successful21. FM symptoms can be reduced by the effective use of exercises22. According to the study by Dadabhoy and Clauw, the most effective intervention to treat fibromyalgia is exercise and second to that is cognitive behavioral therapy23. A meta-analysis of six studies also revealed that aerobic-only exercise had high-quality effects on general well-being and comfort of patients. Moreover, great improvement in the signs and symptoms were observed. Bergman in its article illustrated that, emotional and cognitive factors determine how a patient responds to sensory input and perceives pain and thus modifies the behavior and attitude towards pain that can increase pain threshold in patients with fibromyalgia. Studies also show meditation, relaxation and stress management options as an efficient adjuvant treatment24.
The results found in this study indicates that, the functional status and quality of life improved in group 2 since they were receiving effective exercise regime as compared to the group 1 who was receiving the combined therapy. This means that the effectiveness of exercises has a vital role in relieving FM pain.
According to the meta-analysis written by Kelley et al, they found that the Quality of Life and general wellbeing has improved a lot in women through exercises suffering with FM measured by FIQR25, while in another study done by Thomas et al, moderate evidence was found related to aerobic exercises and pain in FM, after the data analysis in their review26.
Whereas, from clinical perception, it is difficult to treat FM and patients present with comparatively severe levels of disability, but without obvious markers of pathology. Recently, a study by Walitt et al, conducted in 2011 consisted of longitudinal data from 1555 FM patients revealed that, over the course of 10 years, most patients experienced fluctuation in symptom severity, 35–40% of patients steadily worsened, and only 25% improved gradually over time27.
Some of the systemic reviews have a doubt on efficacy of exercises in fibromyalgia28, while others show little or no effect on pain or tender point, whereas other shows significant improvements. But in our study, we have found significant results in both the groups, group 1 show more significant results as compared to group 2 in the VAS scale and reducing the pain.
Carbonario et al, found in their study that, High frequency TENS in association with aerobic and stretching exercises is effective in treatment of FM symptoms, as compared to the TENS or exercises alone29. But in our study, there is no such huge difference found between the groups.
To assess the current health (physical function, symptoms) of patients with fibromyalgia in clinical and research settings the FIQR are frequently used and applicable for the better and authentic results. The FIQR was developed from information gathered from client reports, functional status instruments, and clinical observations. This instrument measures physical functioning, work status, depression, anxiety, morning tiredness, pain, stiffness, fatigue, and well-being over the weeks.
There was significant improvement found in depression, anxiety, fatigue, sleep symptoms, work performance and social life through FIQR. We build that, our protocol of invention with TENS yielded significant and was clinically important in several of these symptoms, and it may be moderately improved in the pain also. Furthermore, fibromyalgia is a multi-factorial disorder, our study suggested that, the combination of different physical therapy techniques, modified according to the therapist assessment and patient’s needs; it is an also effective option to treat the disorder.
CONCLUSION
This study was conducted to find out the effectiveness of high frequency Transcutaneous electrical stimulation at the tender point of upper cervical as adjunctive therapy of fibromyalgia patients, the results interpreted that after multiple treatment sessions, there is significant reduction in pain intensity as well as in other signs and symptoms. However, there was no huge significant difference found between both the groups, high frequency TENS and adjunctive therapy at the tender point of upper cervical in fibromyalgia.
ACKNOWLEDGEMENTS
My respect and appreciation go to the teachers and my guiders who direct me in a use full path to perform good efforts and the space to accomplish this commonly has to be carved out of non-existent spare time. I truly cannot thank any of you enough. I wish to express gratitude to Pakistan Journal of Rehabilitation team; on the way to encourage me to entre in the world of evidence-based practice. My profound thanks also go to the remarkable group of health care professionals who have contributed their time and efforts to collect the data of the research.
REFERENCES
- Valim V, Oliveria L, Suda A, Silva L. Aerobic fitness effects in fibromyalgia. J Rheumatol. 2003;30(5):1060-9.
- Wolfe F, Cathey MA. Prevalence of primary and secondary fibrositis. J Rheumatol. 1983;10:965-96.
- Thomas EN, Blotman F. Aerobic exercise in fibromyalgia: a practical review. Rheumatol Int. 2010;30:1143-50
- Sanudo B, Galiano D, Carrasco L, Blagojevic M, Hoyo M, Saxton J. Aerobic exercise versus combined exercise therapy in women with fibromyalgia syndrome: a randomized controlled trial. Arch Phys Med Rehabil. 2010;91:1838-43.
- Wolfe F, Smythe HA, Yunus MB, Bennett RM, Bombard.ier C, Goldenberg DL, et al. The American College of Rheumatology 1990 Criteria for the Classification of Fibromyalgia. Report of the Multicenter Criteria Committee. Arthritis Rheum. 1990;33(2):160-72
- Demitrack MA, Crofford LJ. Evidence for and pathophysiologic implications of hypothalamic-pituitary- adrenal axis dysregulation in fibromyalgia and chronic fatigue syndrome. Ann N Y Acad Sci. 1998;840:684-97.
- Al-Allaf AW, Dunbar KL, Hallum NS, Nosratzadeh B, Templeton KD, Pullar T. A case-control study examining the role of physical trauma in the onset of fibromyalgia syndrome. Rheumatology (Oxford) 2002;41(4):450-3.
- Liebanio RE, Rakel B, Vance CG, Walsh DM, Shukla KA. An investigation of the development of the analgesic tolerance to TENS in humans. Pain. 2011;152(2):335-42.
- Curtis K, Osadchuk A, Katz J. An eight-week yoga intervention is associated with improvements in pain, psychological functioning and mindfulness, and changes in cortisol levels in women with fibromyalgia. Journal of Pain Research. 2011;4:189-201.
- Carville SF, Arendt-Nielsen S, Bliddal H, Blotman F, Branco JC, Buscila D. EULAR evidence-based recommendations for the management of fibromyalgia syndrome. Ann Rheum Dis. 2007;67:536–541.
- Davis MC, Zautra AJ, Reich JW. Vulnerability to stress among women in chronic pain from fibromyalgia and osteoarthritis. Ann Behav Med. 2001; 23(3):215–26.
- Okonkwo R, Bradely L, Sotolongo A, Cannon R, Fillingim R. Effect of stressful imagery on thermal pain ratings of patients with fibromyalgia: what mediates this relationship? J Pain. 2007;8(4):S25.
- Wall PD, Sweet WH. Temporary abolition of pain in man. Science 1967;155(3758):108-109.
- Dworkin RH, Turk DC, Farrar JT, Allen RR, Bellamy N, Brandenburg N, et al. Core outcomes domains for chronic pain clinical trials: IMMPACT recommendations. PAIN. 2003;106:337-345.
- Dailey DL, Vance CGT, liebano RE. Trancutaneous Electrical nerve stimulation (TENS) reduces and improve the physical performance in people with fibromyalgia. J pain 2012;12:23.
- Sluka KA, Walsh D. Transcutaneous electrical nerve stimulation: Basic science mechanisms and clinical effectiveness. J pain. 2003;4(3):109-21
- Robertson V, Ward A, Low J, Reed A. Electrotherapy explained principle and practice. 3rd ed. Bostan: Butterworth Heinemann; 2006.
- Lofgren M, Norrbrink C. Pain relief in women with fibromyalgia: A cross over study of superficial warmth stimulation and transcutaneous electrical nerve stimulation. J Rehabil Med. 2009;41(7):557-62.
- McCain GA, Bell DA, Mai FM, Halliday PD. A controlled study of the effects of a supervised cardiovascular fitness training program on the manifestations of primary fibromyalgia. Arthritis Rheum. 1988;31(9):1135-1141.
- Melzack R, Wall PD. Pain mechanisms: a new theory. Science. 1965;150(3699):971-9.
- Imamura M, Cassius DA, Fregni F. Fibromyalgia: From treatment to rehabilitation. Eur J Pain. 2009;3(2):117–122.
- Kelley GA, Kelley KS, Hootman JM, Jones DL. Exercise and global wellbeing in community-dwelling adults with fibromyalgia: A systematic review with meta-analysis. BMC Public Health. 2010;10:198.
- Dadabhoy D, Clauw DJ. Therapy insight: Fibromyalgia – a different type of pain needing a different type of treatment. Nat Clin Pract Rheumatol. 2006;2(7):364–72.
- Busch AJ, Schachter CL, Overend TJ, Peloso PM, Barber KA. Exercise for fibromyalgia: A systematic review. J Rheumatol. 2008;35(6):1130–44.
- Busch AJ, Barber KA, OverendTJ,Peloso PM, Schachter CL. Exercise for treating fibromyalgia syndrome. Chochrane Database Syst Rev. 2007;(4):20-29
- Hauser W, Thieme K, Turk DC. Guideline on the management of fibromyalgia syndrome –A systematic review. Eur J Pain. 2010;14(1):5-10.
- Walitt B, Fitzcharles MA, Hassett AL, Katz RS, Häuser W, Wolfe F. The longitudinal outcome of fibromyalgia: A study of 1555 patients. J Rheumatol. 2011;38(10):2238-46.
- Büssing A, Ostermann T, Lüdtke R, Michalsen A. Effects of yoga interventions on pain and pain-associated disability: A meta-analysis. J Pain. 2012;13(1):1-9.
- Carbonario F, Matsutani LA, Yuan SL, Marques AP. Effectiveness of high frequency TENS at tender points as adjuvant therapy for patients with FM. Eur J Phys Rehabil Med. 2013;49(2):197-204.