
ABSTRACT
BACKGROUND
The transaminases, ALT and AST (alanine and aspartate transaminases, respectively), that are generally considered to be the hepatic enzymes, also found in skeletal muscles. Continual elevated levels of both enzymes in patients with several forms of muscular dystrophy and musculoskeletal diseases have been documented in several studies.
AIM AND OBJECTIVES
The present study is undertaken to examine the possibility of highlighting transaminases elevation in muscular dystrophy as an indicator of concomitant muscular damage, rather than hepatic injury due to medications, and relate its significance with underlying myofibrillar damages.
MATERIALS AND METHODS
Data of a total of 52 patients (males = 38, females = 14) were obtained during December 2006 to December 2011 and complied as per criteria. Plasma CK enzyme and transaminases (AST and ALT) levels were performed by enzymatic methods on Hitachi 912. A specific hepatic marker gamma glutamyl transpeptidase (GGT) was also measured to assess the extent or presence of hepatic damages. All enzymatic data were analyzed using regression correlation analyses with significance level of P < 0.05.
RESULTS
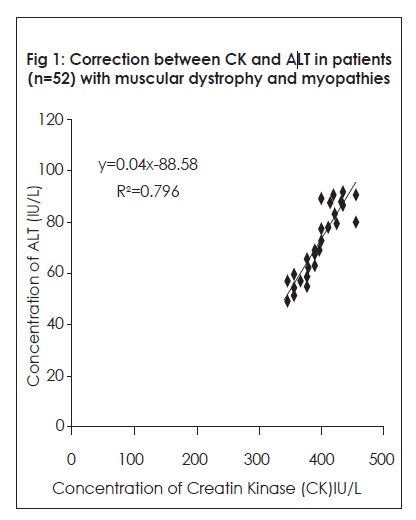
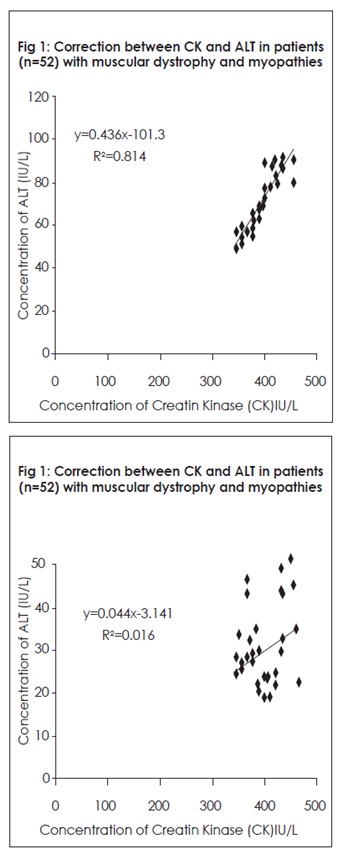
Cumulative as well as individual data analysis showed significant correlation of transaminases with CK, which is the distinct indicator of muscle damage. ALT R2 correlation with CK showed linear regression correlation of R2 = 0.796 and for AST R2 = 0.814. Cumulative mean of CK was 406.83 ± 20.15 IU/L; ALT = 70.86 ± 10.21 IU/L, AST = 68.78 ± 8.30 IU/L and GT = 20.13 ± 4.30 IU/L.
CONCLUSION
The present study describes the elevated level of transaminase, ALT and AST in patients of muscular dystrophy and myopathies. It was also exhibited that both transaminases concentration linearly correlated with muscle marker CK. No hepatic damage was noted in all patients as manifested by normal levels of GGT, a distinct marker of hepatic origin.
KEY WORDS
Creatine Kinase, Alanine transaminase (ALT), Aspartate Transaminase-(AST), Muscular Dystrophy, Myopathy, Regression.
Junaid Mahmood Alam
Department of Biochemistry
Laboratory services
Liaquat National Hospital and Medical College
Sumaira Imran Farooqui
Principal
Ziauddin College of Physical Therapy
Ziauddin University
Fatima Hussain
Department of Biochemistry
Laboratory services
Liaquat National Hospital and Medical College
Syed Riaz Mahmood
Govt Lyari General Hospital Karachi
[ALam JM, Farooqui SI, Hussain F, Mahmood SR. Determination Of Transaminases And Creatine Kinase Levels In Patients With Muscular Dystrophy And Musculoskeletal Diseases. Pak. j. rehabil. 2014;3(1):15-18]
INTRODUCTION
Continual elevated levels of serum transaminases (Alanine transaminase-ALT; Aspartate transaminase-AST) in patients with several forms of muscular dystrophy and musculoskeletal diseases have been documented in earlier studies1-5. Additionally, similar biochemical manifestations have also been observed in inflammatory myopathies1,6. The transaminases, ALT and AST, generally considered to be the hepatic enzymes, are also found in skeletal muscle 1,6,7. However, the concentration or activity of both in skeletal musculature is one tenth of those occur in hepatocyte origin. Creatine kinase (CK) or creatine phosphor-kinase (CPK), on the contrary, is a susceptible marker of skeletal muscle dystrophy, such that its concentration reaches 100 times higher in muscle than in hepatocytes after onset or progression of a disease 1,8. Previous studies regarding determination of transaminases in patients with muscular dystrophies and myopathies suggested that ALT and AST elevation might also be due to myofibrillar damages, which causes their release in the blood stream7,9. It was also pointed out that restricting ALT/AST in the determination of the hepatocyte damages, which might be caused by usage of myopathy treating medications, such as steroids, azathioprine and methotrexate, could sometimes be misleading and may end in halting the treatment9-12.
The present study is undertaken to examine the possibility of highlighting transaminases elevation in muscular dystrophy as an indicator of concomitant muscular damage, rather than hepatic injury due to medications, and relate its significance with underlying myofibrillar damages.
MATERIALS AND METHODS
Study Design and Data Collection
The study design followed for the presented research was established methods and protocols documented earlier13. Briefly, the inclusion period for this cohort study was from December 2006 to December 2011, of which data were collected retrospectively from November 2006 to December 2004 and prospectively from December 2006 to Dec 2011. Patients who met the following criteria were eligible for the study. Thus, the inclusion criteria were patients aged > 20 years to <75 years and had a diagnosis of myopathies as per description of reported earlier14,15. Data of total 52 patients (males = 38, females = 14) were obtained and complied as per criteria. Data was also collected from LIS and HIMS archives, where possible.
Blood sample Collection and Analysis
Blood samples were collected by venipuncture on Li-heparinate 5 ml tubes from patients after 72 hours of resting and an overnight fasting. Plasma CK enzyme and transaminases (AST and ALT) levels were performed by enzymatic methods at admittance and at the diagnosis of myopathy. AST, ALT and CK levels were measured on Hitachi 912 (Roche Diagnostics-Basel) using commercial kits and both internal and external quality controls. A specific hepatic marker Gamma Glutamyl Transpeptidase (GT) was also measured to assess the extent or presence of hepatic damages. The normal ranges for enzymatic analytics are plasma CK/CPK, males > 18 years: 52-336 IU/L, females > 18 years: 38-176 IU/L; AST, 8-48 IU/L; and ALT, 7-45 IU/L, and GT Males = 12-48 IU/L and females = 6-29 IU/L, respectively.
Statistical analysis
All enzymatic data obtained were analyzed using SPSS 13 (USA), considering significant level of P < 0.05. Additionally, regression analysis was also performed to correlate AST and ALT levels with that of CK.
RESULTS
A total of 52 patients (males = 48, females = 14) were selected for the present study. Initially over the period of December 2006 to December 2011, data sets of around 160 patients (Males = 103 and females = 57) were screened and analyzed, out of them 52 falls into our required criteria. Cumulative as well as individual data analysis showed significant correlation of transaminases with CK, which is the distinct indicator of muscle damage. ALT R2 correlation with CK showed linear regression correlation of R2 = 0.796 (Fig 1) and for AST R2 = 0.814 (Fig 2). To distinguish the fact that the correlation of transaminases determined in serum/plasma was that from muscle injury and not from hepatocyte damage, a prominent hepatocyte marker GT was also estimated and analyzed for correlation with CK. Interestingly, no significant relationship was obtained, as GT levels were found to be mostly within the normal ranges and thus manifested R2 values of less than 02 (R2 CK versa GT = 0.016) (Fig 3). Cumulative mean of CK = 406.83 ± 20.15 IU/L; ALT = 70.86 ± 10.21 IU/L, AST = 68.78 ± 8.30 IU/L and GT = 20.13 ± 4.30 IU/L.
DISCUSSION
It was discussed in several studies and even proven that high transaminase levels in patients with muscular dystrophy and myopathies, and also in those undergoing treatments, were from muscle damage rather than hepatocyte injury1,9,16.
The researcher have argued that evidently manifesting proximal muscle weakness with high CK level in patients also suggests that occult muscular dystrophy or inflammatory myopathy might also be responsible for the same1,4,5. In our study high levels of transaminases correlated well with elevated levels of CK, with mostly normal levels of GT, a prominent hepatic injury marker, thus suggesting evidently, that transaminases leakage in blood stream was from muscular cells rather than hepatocytes. Moreover, several past studies also noted that, without taken into consideration the linearly correlated high levels of transaminases with CK, or establishing the fact that there might be some underlying, undiagnosed myopathies, without any hepatic damages due to medications; treatments were halted or altered, thus causing hardships for patients 9-12,17.
It was reported earlier that elevated transaminase levels were noted in myositis9-12 and muscular dystrophy17,18. High transaminase levels, especially that of ALT up to 50% (and AST up to 17%) were reported in a study carried out in patients with myotonic dystrophy type 216. Similarly, another study documented that transaminase performs several metabolic functions in many cells, including that of muscles, and its leakages into the blood stream might be due to myofibrillar damages, as usually observed in case of elevated LDH and CK concentrations9,19. In conclusion, the present study describes the elevated level of transaminase, ALT and AST in patients of muscular dystrophy and myopathies. It was also exhibited that both transaminases concentration linearly correlated with muscle marker CK. No hepatic damage was noted in all patients as manifested by normal levels of GT, a distinct marker of hepatic origin.
ACKNOWLEDGEMENTS
The authors wish to thank Prof Dr Hugh McMillan (Department of Neurology, Boston Children’s Hospital, Boston, USA) and Prof Dr K Edge (Rheumatic Disease Center, Hope Hospital, Safford, UK) for providing relevant articles and information.
REFERENCES
- McMillan HJ, Gregas M, Darras BT, Kang PB. Serum transaminase levels in boys with Duchenne and Becker muscular dystrophy. Pediatrics 2011; 127:132-136.
- Kohli R, Harris DC, Whitington PF. Relative elevations of serum alanine and aspartate aminotransferase in muscular dystrophy. J Pediatr Gastroenterol Nutr. 2005;41(1):121–124.
- Munsat TL, Baloh R, Pearson CM, Fowler W. Serum enzyme alterations in neuromuscular disorders. JAMA. 1973;226(13):1536 –1543.
- Tay SK, Ong HT, Low PS. Transaminitis in Duchenne’s muscular dystrophy. Ann Acad Med Singapore. 2000; 29(6):719–722.
- Zamora S, Adams C, Butzner JD, Machida H, Scott RB. Elevated aminotransferase activity as an indicator of muscular dystrophy: case reports and review of literature. Can J Gastroenterol. 1996;10(6):389–393.
- Wroblewski F. The clinical significance of transaminase activities of serum. Am J Med. 1959;27:911–923.
- Pratt DS, Kaplan MM. Evaluation of abnormal liver-enzyme results in asymptomatic patients. N Engl J Med. 2000;342(17):1266–1271.
- Tsung SH. Creatine kinase isoenzyme patterns in human tissue obtained at surgery. Clin Chem. 1976;22(2):173–175.
- Edge K, Chinoy H, Cooper RG. Serum alanine aminotransferase elevations correlate with serum creatine phosphokinase levels in myositis. Rheumatology 2006;45:487–488.
- Morton BD III, Statland BE. Serum enzyme alterations in polymyositis. Possible pitfalls in diagnosis. Am J Clin Pathol 980;73:556–7.
- Helfgott SM, Karlson E, Beckman E. Misinterpretation of serum transaminase elevation in ‘‘occult’’ myositis. Am J Med 1993;95:447–9.
- Nathwani RA, Pais S, Reynolds TB, Kaplowitz N. Serum alanine aminotransferase in skeletal muscle diseases. Hepatology 2005;41:380–2.
- Alam JM, Farooqui SI, Hussain A, Mahmood SR. Correlation of Creatine kinase and myoglobin concentrations in patients suffering from debilitated conditions related to myopathies. Pak. j. rehabil. 2012;1(1):22-28.
- Hoogendijk JE, Amato AA, Lecky BR, Choy EH, Lundberg IE, Rose MR, et al: 119th ENMC International Workshop: trial design in adult idiopathic inflammatory myopathies, with the exception of inclusion body myositis, 10-12 October 2003, Naarden, The Netherlands. Neuromuscular Disord 2004;14:337-345.
- Tolédano C, Gain M, Kettaneh A, Baudin B, Johanet C, Chérin P et al. Aldolase predicts subsequent myopathy occurrence in systemic sclerosis. Arthritis Research & Therapy 2012;14:2-9.
- Heatwole C, Johnson N, Goldberg B, William BS, Martens, BA, Moxley III R. Laboratory Abnormalities in Patients with Myotonic Dystrophy Type 2. Arch Neurol. 2011;68(9):1180–1184
- Kamath BM, Dhawan A, Mieli-Vergani G. Raised serum transaminases: not always liver disease. Arch Dis Child. 2000;82:270–1.
- Zamora S, Adams C, Butzner JD, Machida H, Scott RB. Elevated aminotransferase activity as an indication of muscular dystrophy: case reports and review of the literature. Can J Gastroenterol, 1996;10:389–93.
- Janssen GM, Kuipers H, Willems GM, Does RJ, Janssen MP, Geurten P. Plasma activity of muscle enzymes: quantification of skeletal muscle damage and relationship with metabolic variables. Int J Sports Med 1989; 10 (Suppl. 3):S160–S168.