
ABSTRACT
A case report study conducted in a tertiary care hospital to determine the effectiveness of supervised exercise diet plan along with behavioral therapy to reduce weight in the metabolic syndrome. A 54 years old obese male was selected to conduct the study that suffering from diabetes for last 10 years, hypertensive previous 13 years, knee osteoarthritis previous 8 years back and also has complaint of dyspnea as a result facing severe problems in his ADL. He was on 8 different medications when he visited a Physiotherapy OPD in a tertiary care hospital by his consultant to secure his health status. He was than enrolled in fitness program to reduce weight under supervision of a physical therapist. According to his lab reports he was highly on health risk and was going in severe depression due to the difficulty facing in his daily life. The out measures of our study was Visual Analogue scale, Exercise and diet plan with counseling sessions, after 16 weeks supervised exercise diet plan and counseling sessions we observe a marked improvement in glucose tolerance, exercise tolerance, lipid profile and hypertension. The patient was following exercise plan for 5days/week and diet plan throughout the month with a single counseling session in a week with marked reduction in medications. Our study concludes that the medically supervised weight-loss program facilitates is safe and effective in weight reduction with significant decrease in expenses of medications.
Keywords
Diabetes, Overweight, Obesity, Weight Reduction, Metabolic Syndrome, BMI
Muhammad Sarfraz
Assistant Professor
Ziauddin College of Physical Therapy
Ziauddin University
Erum Naz
Senior Lecturer
Ziauddin College of Physical Therapy
Ziauddin University
Arham Shamsi
Incharge Physiotherapist
M.S Hospital
Syeda Amool Sakeena Rizvi
Lecturer
Ziuddin College of Physical Therapy
Ziauddin University
Dr. Rubina Kanwal
Incharge
Ahmed’s Healing Hands
Roomi Ilyas
Physiotherapist
Self Employed
[Sarfraz M, Naz E, Shamsi A, Rizvi SAS, Kanwal R, Ilyas R. Weight Loss causes Improvement in Metabolic Syndrome and cost effective: Case Study. Pak. j. rehabil. 2013;2(2):45-47]
INTRODUCTION
Overweight and obesity are defined as abnormal or excessive fat accumulation that presents a risk to health which can be measure by body mass index (BMI)1 which can be calculated by dividing a person’s weight (in kilograms) by the square of his or her height (in meters). A person with a BMI of 30 or more is generally considered obese2. A person with a BMI equal to or more than 25 is considered overweight 2,3. Overweight / obesity are major risk factors for a number of chronic diseases, including DM, cardiopulmonary, cardiovascular diseases and cancer2. Obesity is not only affecting elders but Worldwide childhood obesity is also at large 4,5 and this epidemic is also becoming a challenging issue in developing countries like Pakistan6-8. Once obesity was considered as a problem of high-income countries only but now overweight and obesity are dramatically on the rise in low- and middle-income countries, particularly in urban settings. In Pakistan the prevalence of obesity is 10.3%9.
Obesity has a strong relation with diabetes. In 2000, diabetes was the 6th leading cause of life loss, based on the 69,301 death certificates listing it as the underlying cause. This number undervalues the actual numbers because diabetes is likely underreported as the cause of death. In a survey conducted in 2002, 18.2 million people had diabetes, and only 13 million of them were diagnosed10.
CASE STUDY
Mr. A is an obese, 54 years old married man with 3 children. By profession he is banker. Mr. A has been suffering from DM for last 10 years. He was diagnosed hypertensive in 2001, type 2 diabetes in 2003 and bilateral knee osteoarthritis in 2005. He has a history of shortness of breath and excessive weight since long. On Visual Analogue Scale he has rated his knee pain to 8 out of 10 which has made him compromised in terms of his daily activities.
He regarded his excess weight as a result of overeating, oversized portions and an increased use of confectionaries and oily food. He has already tried a lot of things to reduce his weight like use of different weight reducing pills, weight reducing belts, and diet plans but every attempt resulted fruitless.
Mr. A’s, average expenditure on medications is around PKR 8,000 a month, according to him.
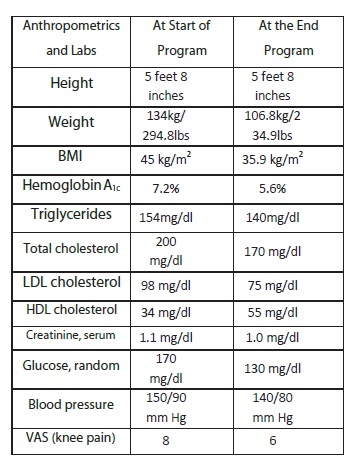
Now Doctor has advised him to supervise weight reduction under the guidance of a physical therapist. Therefore, he has been placed on a 16 weeks medical supervision of weight loss plan at Physiotherapy department of Ziauddin Hospital (north campus). At the start of the supervised weight reduction program that is January 2012, he has following anthropometric and laboratory readings which were recorded as baseline impressions to see the difference after 16 weeks plan.
- Height: 5 feet 8 inches/68 inches
- Weight: 134 kg/294.8 lbs
- BMI: 45 kg/m2
- Hemoglobin A1c (HbA1c): 7.2%
- Triglycerides: 154mg/dl
- Total cholesterol: 200 mg/dl
- LDL cholesterol: 98 mg/dl
- HDL cholesterol: 34 mg/dl
- Creatinine, Serum: 1.1 mg/dl
- Glucose, Random: 170 mg/dl
- Blood pressure: 150/90 mm Hg
- VAS (knee pain) : 8/10
- At the beginning of the 16 weeks program the patient
- was on following medications and supplements:
- Losartan/hydrochlorothiazide 50/12.5 mg twice
- daily (HCTZ)
- Metoprolol extended release, 200 mg
- daily/once a day
- Verapamil SR: 240 mg once a day
- Glyburide: 5mg twice daily Glyburide/metformin:
- 5/500mg twice daily
- Pioglitazone: 45 mg once a day
- Meloxicam: 7.5 mg once a day
- Ursodiol: 300 mg twice daily
INTERVENTION
In light of above readings Mr. A was given a Plan consisted of 16 weeks supervised weight loss treatment, providing lifestyle education and modifications. This consisted of physical activity/exercise plan, nutritional alterations, and changes in daily routine and counseling sessions.
Exercise plan included aerobic workout for 30 min on recumbent bike at 60 RPM, muscle conditioning exercises for 15 repetition of all major muscle groups of body (Pectoralis, Lattissmus Dorsii, Deltoid, Biceps, Triceps, Quadriceps, Hamstrings, Calves, Rectus Abdominus and Erector Spinae) and stretching exercises.
Nutritional alterations consisted of 1200 kcal/day including all necessary macro and micronutrients with emphasis on high fiber diet to counteract constipation and to satisfy the hunger. Additionally, he was advised to take 4 short meals of 300 kcal to aid caloric consumption.
Furthermore, 1-hour behavioral education/counseling session per week was also included to maintain the motivation level.
RESULT AND DISCUSSION
In the case above, Mr. A needed to lower his blood glucose and A1C to help him lose weight. To achieve his goal he had to increase his exercise tolerance, control his portion sizes, and decrease his intake of fats and sugars. Before starting the program, his blood glucose, blood pressure, and A1C were all above target range.
After the 16weeks, he had lost 60 lbs/27.2 kgs (134 kg to 106.8 kg); and his BMI was improved from 45kg/m2 to 35.9 kg/m2. His glucose levels improved from 170 to 130 mg/dl; his average blood pressure was enhanced from 150/90 to 140/80 mmHg. Mr. A also showed marked improvement in triglycerides, HDL and LDL levels which became 140, 75 and 55 mg/dl respectively from 154, 98 and 34mg/dl respectively. Due to weight reduction and increase muscle endurance and strength the knee pain was decreased to 6 from 8 rated out of 10 at visual analogue scale.
As a result, Mr. A was able to decrease the number and dosages of medications he was previously taking. Over the course of the program, three medications (glyburide/ metformin, metoprolol extended release) were stopped completely and one was decreased by half (losartan/HCTZ). This netted a cost savings of PKR 4500 per month or PKR 54000 per year. His Losartan/HCTZ, 50/12.5 mg, was decreased to once daily; A1C decreased 1.6 percentage points to 5.1% even as the oral diabetes medications were discontinued.
This weight-loss program mimics that, used in the successful Diabetes Prevention Program with ongoing support from health coaches. An ongoing dilemma is that weight is often regained after a weight-loss program and its coaching ends. A feature of the program used here is the availability of a maintenance phase including exercise plan, diet plan and counseling sessions.
CONCLUSION
As this case demonstrates, weight loss brings many benefits related to diabetes, metabolic syndrome, and cost reduction of medical care. Medically supervised weight-loss programs facilitate safe and effective weight reduction. The next critical step is for clinicians to continue to follow patients and ensure their participation in maintenance programs.
REFERENCES
- Hoeger WK. lifetime physical fitness and wellness. 10th edition. Australia: wadsworth; 2011.110-111.
- Hoeger WK, Hoeger A. principal and labs for fitness and wellness. 6th Ed. USA: wadsworth; 2010.202-05.
- Anspaugh JD, Hamrick HM, Rosato DF. Wellness concepts and applications. 6th edition. America: MsGrawHill; 2006.232-233.
- Gupta DK, Shah P, Mishra A, Bharadwaj S, Gulati S, Gupta N et al. Secular trends in prevalence of overweight and obesity from 2006-2009 in urban Asian Indian adolescents aged 14-17 years. JPMC 2011;6(2):172-21.
- Frayling MT, Timpson NJ, Weedon MM. A Common Variant in the FTO Gene Is Associated with Body Mass Index and Predisposes to Childhood and Adult Obesity. 2007;316:889-94.
- Mushtaq MU, Gull S, Abdullah HM, Shahid U, Shad MA, Akram J. Prevalence and socioeconomic correlates of overweight and obesity among Pakistani primary school children. BMC Public Health 2011;11:724.
- Qidwai W, Ashfaq T. Imminent Epidemic of Diabetes Mellitus in Pakistan: Issues and Challenges for Health Care Providers. JLUMHS 2010;9(3):231-34.
- Chopra M, Galbraith S, Darnton-Hill I. A global response to a global problem: the epidemic of over nutrition. Bull World Health Organ 2002;80(12):952–958.
- Jaffer TH. Prevalence of overweight and obesity and their association with hypertension and diabetes mellitus in an Indo-Asian population. CMAJ 2006;175(9):1071-1077.
- National Diabetes Statistics. last updated: 2011 December 6, cited 2012 December 16 Available at: http://diabetes.niddk.nih.gov/dm/pubs/statistics/- index.aspx