
ABSTRACT
OBJECTIVE
To evaluate the Q/H strength ratio, before and after the isotonic exercises.
MATERIAL AND METHODS
The Quasi-experimental design was selected in this study. 50 female patients with knee osteoarthritis and disturbed Quadriceps – Hamstring (Q/H) ratio were assessed through Visual Analog Scale (VAS), Range of Motion, Kellgren-Lawrence Scale and Repetition Maximum (RM). All of the patients were assessed at 1st visit, and then 15 sessions of isotonic exercises were given. They were examined again at 15th day to assess the effects of isotonic exercises on Q/H ratio.
RESULTS
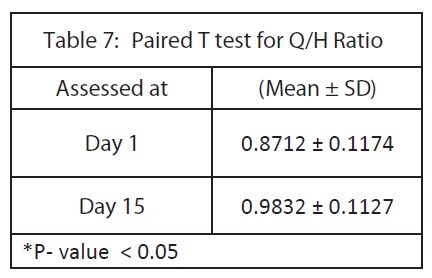
There was a significant difference in Q/H ratio before and after isotonic exercises. The average Q/H ratio before an exercise was less (0.8712 ± 0.1174) as compared to the ratio taken after exercises (0.9832 ± 0.1127). The P-value was less than 0.05 that was significant. The strength of quadriceps and hamstring muscles were increased, hence reduced the intensity of pain.
CONCLUSIONS
The isotonic exercises were found to be effective for strengthening of quadriceps and hamstring muscles. There was a significant increase in Q/H ratio after isotonic exercises, with improvement in pain and ROM. This may improve their daily functional activities.
Keywords
Osteoarthritis, Q/H Ratio, Quadriceps, Hamstring, Isotonic Exercises, Osteoporosis, Repetition Maximum (RM), Strength
Nazish Rafique
Lecturer
Ziauddin College of Physical Therapy
Ziauddin university
Ghazala Noor Nizami
Assistant Professor
Ziauddin College of Physical Therapy
Ziauddin University
Anum Rafique
Physical Therapist
Mamji Hospital
[Rafique N, Nizami GN, Rafique A. Effectiveness Of Isotonic Exercises On Quadriceps – Hamstring Strength Ratio In Osteoarthritic Females. Pak. j. rehabil. 2013;2(2):15-20]
INTRODUCTION
Osteoarthritis (OA) is a progressive disorder that affects the joint capsule, cartilage, synovia and subchondral bone1. In osteoarthritis of knee, narrowing of joint space occur due to destruction or degeneration of articular cartilage, bony sclerosis, sharpening of articular margins, intra-articular structures, marginal lipping, bony cyst and osteophytic changes with the progression of this condition2. Osteoarthritis is a degenerative disease and depends on many etiological factors. It is related to repetitive movements, repetitive mechanical loads and age. The etiological factors are separated into three sub-groups; sex, body mass and anatomy3. Knee joint, thigh and leg muscles work together, that can assess by variety of techniques, such as visual observation, range of motion and Q/H ratio4. Production of tension in the knee joint muscle, termed as its strength; and in knee osteoarthritis, quadriceps muscle is more prone to be affected5-9. Approximately 60% of the population are affected by Osteoarthritis, having the age more than 50 years 10,11. The patients commonly presented with pain, inflammation, decreased range of motion, joint stiffness, muscular weakness, especially in quadriceps (Q) and hamstring (H) muscles in case of knee OA. Osteoarthritis also alters the joint proprioception, which affects the gait pattern of an individual12-14. In osteoarthritis, decreased muscular strength causes the progressive loss of function and joint integrity. Due to this, individuals have problem in stair climbing, walking, rising up from chair and also have restriction of knee range of motion13. In osteoarthritis, gait changes may also observed due to misalignment of the limb and instabilities of the structures related to that particular area. That patient present with limping gait, sometimes that limping is due to pain rather than any misalignment of the limb, and is more common in early stage of osteoarthritis. During walking and joint movement, crepitus can be heard or felt, due to the degeneration of the articular surfaces. Those surfaces become irregular15. Knee complex consists of Tibiofemoral (TF), Patellofemoral (PF) and Tibiofibular joints. Osteoarthritis affects all of these in relation to the severity. The severity of osteoarthritis of the knee can be classified according to the Kellgren- Lawrence scale. This scale consists of five degrees16:
0No osteoarthritis
1 Doubtful osteoarthritis
2 Minimal osteoarthritis
3 Moderate osteoarthritis
4 Severe osteoarthritis
Knee joint stability depends on its internal and external forces with sufficient magnitude. The ability of the quadriceps muscle is to provide dynamic stability to the knee joint and absorbs forces which act on it8.
Osteoarthritis affects the joint, both biochemically and biomechanically. The osteoarthritic changes cannot be stopped by any medicine or other, but it can be delayed through physical activities and rehabilitation program. The proper and effective rehabilitation program is more important to delay or slow the process of knee osteoarthritis. Osteoarthritis of knee reduces the strength of quadriceps and hamstring muscles as well as reduces the sensorimotor function of the lower limb, proprioception of the knee joint and hence also affects the gait pattern of an individual17–23.
For the maintenance of good posture and the control of movement, during walking and during loading response on musculoskeletal system, the muscle strength plays a key role. The muscle produces tension for the maintenance of posture and balance24.
Osteoarthritis of knee affects the strength of muscle or group of muscles. Strength is defined as the ability of muscle to develop tension in a muscle or group of muscles during the maximum effort, either dynamically or statically. Muscle strength is a complex phenomenon and difficult to characterized, as it is affected by many factors including age, gender, and cross-sectional area, types or contraction of muscle. Muscle is the contractile part of the musculoskeletal system of the body and plays a most important role for maintaining the joint structure and function. Any weakness or injury in the muscle of the knee, mostly in quadriceps femoris muscle, causes the knee joint pain2. In osteoarthritis, the flexor- extensor ratio or Quadriceps-Hamstring ratio may be disturbed. That ratio depends on the age of an individual, gender, measuring equipment, tested population, testing position, angular velocity of the joint and the type of the activity in which the persons are involved4.
The cross-sectional area of the extensor of the knee joint is double of the cross-sectional area of the knee flexor and knee extensors also have longer force arm distance as compared to the flexors of the knee joint. Flexors and extensors of the knee joint work together in a rhythmic pattern to produce functional activities related to the knee joint movement. Therefore, it is very important to maintain the strength ratio of both of those muscles. Normally, the quadriceps– hamstring ratio is 2:1 and this flexor-extensor ratio of the knee may vary between 0.4 and 0.925-27. Muscle adapts with the environmental changes and training. It is very important for the performance of targeted or purposeful movement of the body or a specific body part in respect to the environment. Muscle helps to perform very fine movement for fine activities2.
METHODOLOGY
Study Design
The quasi experimental design was used for this study, to evaluate the effects of exercises on Q/H ratio, before and after treatment.
Sample Size
50 patients were included in this study with knee osteoarthritis and disturbed Q/H ratio.
Study Duration
The duration of this study was seven months.
Inclusion Criteria
Female with the age between 45 and 75 years,BMI ≤ 30, knee osteoarthritis, disturbed Q/H ratio, Kellgren- Lawrence scale less than 3, with or without osteoporosis and hypertension were included in this study.
Exclusion Criteria
Females having morning stiffness for more than 30 minutes, inflammatory arthritis, any deformity, any bone pathology, traumatic injuries, any evidence of malignancy, infection on the skin over knee joints were excluded from this study.
Outcome Measures
In this study, we measured the strength of quadriceps and hamstring muscles through Repetition Maximum (RM) and hence the Q/H ratio was calculated.
Instruments
Metal weights of 2kg, 3kg and 4kg, weighing machine were used.
Procedure
a. Isotonic Exercises
Visual Analog Scale (VAS), Range of Motion (ROM) and muscle strength were assessed at day 1. Then, 15 sessions (6 sessions in a week) of isotonic exercises were given to them. It consisted of isotonic quadriceps exercise, straight leg raises, short arc, hamstring strengthening and wall sets. 10 repetitions of every exercise were performed initially by the patients. Later, it was progressed to 15-20 repetitions. Home plan of these exercises as performed in clinic, was given for 3 times per day. Patients were educated to modify their daily activities to reduce the intensity of pain. They were examined again at day 15 to assess the effects of these isotonic exercises on Q/H ratio.
b. Hamstring Muscle Strength Testing
The hamstring strength was tested with the patients in a prone lying position. Their feet hanging over the edge of the couch and a towel roll was placed under the knees to prevent compression of the patella between the femur and the couch. According to the patient tolerance, a weight was selected and strapped around the ankle of the patient who was then instructed to flex her knee against the resistance offered by the load. Each patient lifts the weight within their limits of pain and muscle fatigue. That weight should be noted and kept constant for that patient, to check the strength of muscle before and after the isotonic exercises. The number of times the patient lifts that load through full range of motion (from knee extension to knee flexion) before getting fatigue, was recorded as the equivalent repetition maximum (RM) of the load.
c. Quadriceps Femoris Strength Testing
The isotonic quadriceps strength was determined with the patient in a high sitting position with back support. The load should be selected according to the patient tolerance. The metal weight was attached to the ankle, and the patient was instructed to lift the load from 90o knee flexion to full knee extension. Each patient lifts the weight within their pain limits and muscle fatigue. That magnitude of weight was noted and kept constant for that patient, to check the strength of muscle before and after the isotonic exercises. The number of times the patient lifted the load before getting fatigue, from 90o flexion to full extension, was recorded as the equivalent repetition maximum (RM) of the load.
Calculation
i. Isotonic Hamstring and Quadriceps Strength
The RM for the hamstrings and quadriceps of each patient was estimated by using the formula2:
The above calculated RM values were taken as the isotonic quadriceps (Q) and hamstring (H) strength values for every patient.
ii. Isotonic Q/H Strength Ratio
The isotonic Q/H strength ratio was calculated through following formula 2:
RESULT
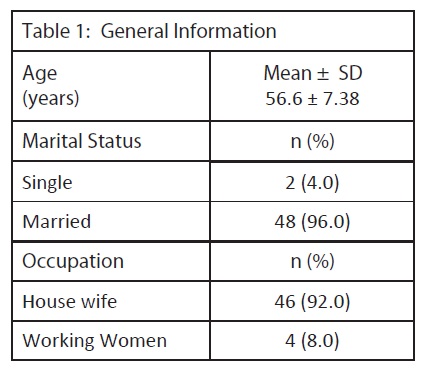
The general information of the patients including gender, age, marital status and occupation are shown in Table 1. 50 females were included in this study with the mean age of 56 years. Among them, 96% were married, 4% were single, 92% were house wives and 8% were working women.
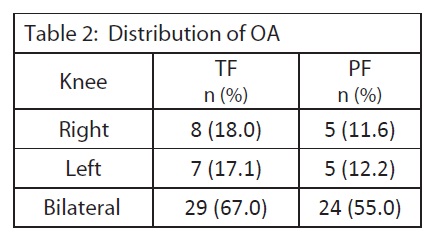
The patients came with the presenting complains of the bilateral, unilateral right or left knees. The presence of osteoarthritis in Tibiofemoral (TF) and Patellofemoral (PF) of that knee was examined by the x-ray. With complain in right knee, there were 18% patients with TF osteoarthritis and 11.6% patients with PF osteoarthritis. With complain in left knee, there were 17.1% patients with TF osteoarthritis and 12.2% patients with PF osteoarthritis. With complain in bilateral knees, there were 67% patients with TF osteoarthritis and 55% patients with PF osteoarthritis. Distribution of OA is shown in Table 2.
The Average Range of Motion (ROM) of all patients was assessed at day 1. Among patients with bilateral knee osteoarthritis, right knee Active ROM (AROM) of flexion (125.75o) was less as compared to Passive ROM (PROM) of 138.3o. AROM of extension shows that they had limited terminal extension by 10.15o and their PROM was 0o. While, left knee AROM of flexion (126.1o) was less than PROM (138.79o). AROM of extension shows that they had limited terminal extension by 10.15o and their PROM was 0o.
In patients with right knee osteoarthritis, right knee AROM of flexion (130o) was less as compared to PROM (140o), AROM of extension shows that they had limited terminal extension by 10o and their PROM was 0o.
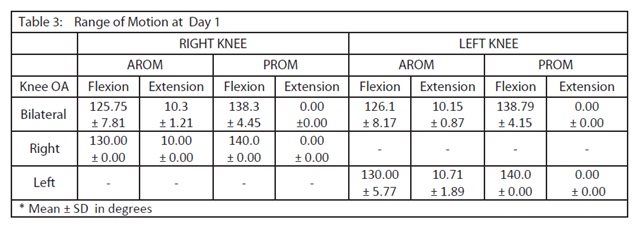
In patients with left knee osteoarthritis, left knee AROM of flexion (130o) was less than PROM (140o), AROM of extension shows that they had limited terminal extension by 10.71o and their PROM was 0o. ROM of all patients at Day 1 is shown in Table 3.
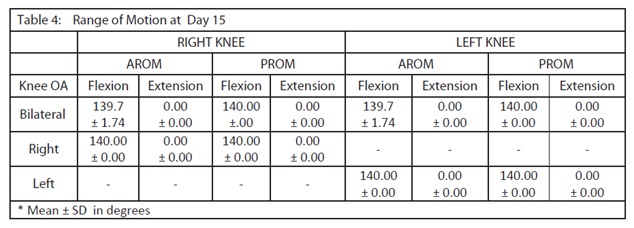
The average range of motion of all patients was assessed again at day 15, after receiving 15 sessions of exercises. In patients with bilateral knee osteoarthritis, right knee AROM of flexion was 139.7o, while PROM was 140o, AROM and PROM of extension was 0o. Among them, left knee AROM flexion was 139.7o, its PROM was 140o, AROM and PROM of extension was 0o.
In patients with right knee osteoarthritis, right knee AROM and PROM of flexion were 140o, while, AROM and PROM of extension were 00. Whereas, same values of AROM and PROM of left knee were obtained in patients with left knee OA.
These results show that ROM of all patients was improved at day 15 (shown in Table 4).
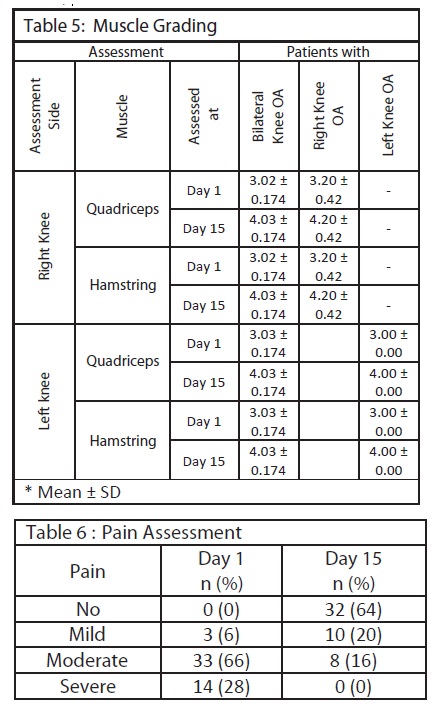
The average muscle grading of quadriceps and hamstring muscles were examined at day 1 and day 15, as shown in table 5. In patients with bilateral knee osteoarthritis, when assessed right knee, the muscle grading of quadriceps and hamstring muscles at day 1 were less as compared to day 15. Among them, left knee muscle strength of quadriceps and hamstring were also improved at day 15.
In patients with right or left knee osteoarthritis, the muscle grading of quadriceps and hamstring muscles showed improved strength after isotonic exercises at day 15. Pain assessment was done on day 1 and 15, by using VAS scale. 0 on VAS was equivalent to ‘No Pain’. 1-2 on VAS scale was considered as mild pain, while 3-6 and 7-10 as moderate pain and severe pain respectively. Results show that pain of patients was improved after treatment. Patients with severe pain at day 1 were 14 and at day 15 no patient had severe pain. Whereas number of patients having no pain, were increased from 3 to 32 (shown in table 6).
The paired T test for Q/H ratio before exercises at day 1 (0.87) was less as compared to the T test for Q/H ratio after exercises at day 15 and after exercises at day 15 (0.98). The P- value was less than 0.05, which was significant. This Q/H ratio is shown in table 7.
DISCUSSION
In this study we assessed the strengths of quadriceps and hamstring muscles in knee osteoarthritis by using Repetition Maximum (RM) method and we found more strength in quadriceps muscle as compared to hamstring muscle. Other studies also found lower strength of hamstring muscle groups, while quadriceps weakness is also a great risk factor for the progression of osteoarthritis. Those studies measured muscle strength by Isotonic RM or 10 RM method and kendall scale 1,2. A study showed that knee osteoarthritic individuals had 30% – 50% lower muscular strength and endurance as compared to the individuals without osteoarthritis1. The function of quadriceps and hamstring muscles is very important in performance of knee. Both of them worked with co-activation. At a time, one muscle acts concentrically and the other eccentrically3. This study focused on isotonic exercises for muscle strengthening. Previous studies also worked with different exercise programs and machines for the strengthening of flexor and extensor muscle groups. A study used eccentric strengthening program twice a week for 6 weeks6. Other study used moderate exercise program, including isotonic and isometric exercises and Medx machine for the strengthening of quadriceps and hamstring muscle groups30.
Isotonic strengthening exercises has great role to reduce the pain intensity and improve the daily functional activities of knee osteoarthritic patients. Previous study showed that strengthening exercises of hamstring and quadriceps muscles enhances the functional activities like walking, daily living of the patient with knee osteoarthritis, reduces the pain and improves the muscle strength, muscle endurance and joint proprioception29.
This study results shows that isotonic exercises improve the Q/H ratio by improving muscle strength. Pain intensity of the patients was improved. With improvement of pain, ROM and muscle strength, the patients will be able to perform their activities of daily living with ease, which improve their quality of life.
Through strengthening exercises with dietary modification, we can slow the rate of disease progression and improves the functional activities and daily living of an individual. The age and weight of an individual are the risk factor for the occurrence of osteoarthritis and muscular weakness. As the age, weight or body mass increase, the quadriceps – hamstring ratio will necessarily be decreased. It is not possible that with the increasing body mass, the muscle strength also increases7.
Increased body weight of patients can put more compressive stress on their knee joints. Therefore, body weight also play role in development of OA in aged individuals. That can also limit their daily activities and increase pain; as a result, muscle strength decreases. This factor might be present in patients of our study, that decreased their muscle strength and hence Q/H ratio. Q/H ratio is important for stability of knee joint 28. The Q/H ratio is approximately 2:1 in healthy individuals but in osteoarthritis this ratio becomes decreased28.
The result of this study shows that, muscle strengths are improved after isotonic exercises and hence improved the Q/H ratio. This is confirmed by the P- value (less than 0.05) which is significant, for the Q/H ratio before and after isotonic exercises.
In our study, we found the significant increased in Q/H ratio after giving the isotonic exercises. The result of our study was similar to the previous study, that is, in osteoarthritis Q/H ratio decreased to normal and through isotonic strengthening exercises can lead the significant difference in that ratio29. In osteoarthritis the hamstring muscle is affected more than the quadriceps muscle due to that the strengthening of hamstring are more important than quadriceps to improve the Q/H ratio29.
CONCLUSION
There was a significant difference in Q/H ratio before and after the isotonic exercises. The isotonic exercises play a key role in the strengthening of quadriceps and hamstring muscles.
REFERENCE
- Carvalho NA, Bittar ST, Pinto FR, Ferreira M, Sitta RR. Manual for guided home exercises for osteoarthritis of the knee. Clinics (Sao Paulo) 2010;65(8):775-80.
- Adegoke BOA, Mordi EL, Akinpelu OA, Jaiyesimi Isotonic Quadriceps-Hamstring Strength Ratios of Patients with Knee Osteoarthritis and Apparently Healthy Controls. Afr. J. Biomed. Res 2007;10:211–216.
- Weiss E, Jurmain R. Osteoarthritis revisited: a contemporary review of etiology. International Journal of Osteoarchaeology 2009;17:437–50.
- Coombs R, Garbutt G. Developments in the use of the hamstring/quadriceps ratio for the assessment of muscle balance. J Sports Sci Med 2002;1(3):56-62.
- Jaiyesimi AO, Jegede J. Hamstring and quadriceps strength ratio: Effect of age and gender. Journal of the nigeria society of physiotherapy 2005;15(2):54-58.
- Kong PW, Burns SF. Bilateral difference in hamstrings to quadriceps ratio in healthy males and females. Phys Ther Sport 2010;11(1):12–17.
- Kaminski TW, Wabbersen CV, Murphy RM. Concentric Versus Enhanced Eccentric Hamstring Strength Training: Clinical Implications. J Athl Train 1998;33(3):216-221.
- Segal NA, Torner JC, Felson D, Niu J, Sharma L, Lewis CE, Nevitt M. Effect of Thigh Strength on Incident Radiographic and Symptomatic Knee Osteoarthritis in a Longitudinal Cohort. Arthritis Rheum 2009;61(9):1210–1217.
- Segal NA, Glass NA, Felson DT, Hurley M, Yang M, Nevitt M, Lewis CE, Torner JC. Effect of Quadriceps Strength and Proprioception on Risk for Knee Osteoarthritis. Med Sci Sports Exerc 2010;42(11):2081–2088.
- Lawrence RC, Helmick CG, Arnett FC, Deyo RA, Felson DT, Giannini EH. Estimates of the prevalence of arthritis and selected musculoskeletal disorders in the United States. Arthritis Rheum 1998;41:778–99.
- Guccione AA, Felson DT, Anderson JJ, Anthony JM, Zhang Y, Wilson PW. The effects of specific medical conditions on the functional limitations of elders in the Framingham Study. Am J Public Health 1994;84:351–8.
- Davis MA, Ettinger WH, Neuhaus JM, Mallon KP. Knee osteoarthritis and physical functioning: evidence from the NHANES I Epidemiologic Follow up Study. J Rheumatol 1991;18(4):591–8.
- Kaufman KR, Hughes C, Morrey BF, Morrey M, An KN. Gait characteristics of patients with knee osteoarthritis. J Biomech 2001;34(7):907–915.
- McCloskey DI. Kinesthetic sensibility. Physiol Rev 1978;58:763–820.
- Easton BT. Evaluation and treatment of the patient with osteoarthritis. J Fam Pract 2001;50(9):791–7.
- Kellgren JH, Lawrence JS. Radiological assessment of osteo-arthrosis. Ann Rheum Dis 1957;16(4):494–502.
- Fisher NM, Pendergast DR. Reduced muscle function in patients with osteoarthritis. Scand J Rehabil Med 1997;29(4):213–21.
- Hall MC, Mockett SP, Doherty M. Relative impact of radiographic osteoarthritis and pain on quadriceps strength, proprioception, static postural sway and lower limb function. Ann Rheum Dis 2006;65(7):865–70.
- Hassan BS, Mockett S, Doherty M. Static posturalsway, proprioception, and maximal voluntary quadriceps contraction in patients with knee osteoarthritis and normal control subjects. Ann Rheum Dis 2001;60(6):612–8.
- Hurley MV. The role of muscle weakness in the pathogenesis of osteoarthritis. Rheum Dis Clin North Am 1999;25(2):283–98.
- Koralewicz LM, Engh GA. Comparison of proprioception in arthritic and age-matched normal J Bone Joint Surg Am 2000;82-A(11):1582–8.
- Sharma L, Pai YC, Holtkamp K, Rymer WZ. Is knee joint proprioception worse in the arthritic knee versus the unaffected knee in unilateral knee osteoarthritis? Arthritis Rheum 1997;40(8):1518–25.
- Slemenda C, Brandt KD, Heilman DK, Mazzuca S, Braunstein EM, Katz BP, Wolinsky FD. Quadriceps weakness and osteoarthritis of the knee. Ann Intern Med 1997;127(2):97–104.
- O’Sullivan SB. Strategies to improve motor control and motor learning. In: Physical Rehabilitation: Assessment and Treatment. 3rd Ed. Philadelphia: FA Davis Co Publication 1994;231.
- Parker MG, Ruhling RO, Holt D, Bauman E, Drayna Descriptive analysis of quadriceps and hamstring torque in high school football players. J Orthop Sports Phys Ther 1983;5(1):2-6.
- Gross MT, Credle JK, Hopkins LA, Kollin MT. Validity of of knee flexion and extension peak torque prediction Phys Ther 1990;70(1):3-10.
- Aagaard P, Simonsen EB, Magnusson SP, Larsson B, Dyhre-Poulsen P. A new concept of isokinetic hamstring: Quadriceps muscle strength ratio. Am J Sports Med 1998;26(2):231-7.
- Hayes KW, Falconer J. Differential muscle strength decline in osteoarthritis of the knee. A developing Arthritis Care Res 1992;5(1):24-28.
- Hafez AR, Al-Johani AH, Zakaria AR, Al-Ahaideb A, Buragadda S, Melam GR, Shajji JK. Treatment of knee osteoarthritis in relation to hamstring and quadriceps strength. J Phys Ther Sci 2013;25(11):1401-5.
- Iwamoto J, Sato Y, Takeda T, Matsumoto H. effectiveness of exercise for osteoarthritie of the knee: A review of the literature. World J Orthop 2011;2(5):37-42.