
ABSTRACT
OBJECTIVE
Occurrence of Low Back Pain (LBP) at an early age, the associated causal factors and resulting consequences in adulthood have been an area of interest for many researchers around the globe. A systematic review in accordance with PRISMA was performed to explore the prevalence of LBP and significant role of carrying heavy backpacks as a risk factor among various others for developing mechanical low back pain among school going children.
METHODS
An electronic search of databases from 2000 to 2013 was carried out. The selected articles reported LBP due to mechanical loads in children and adolescents aged 9-18 years as main outcome. Our analysis was conducted on prevalence rates and associated risk factors.
RESULTS
The results of the review revealed mostly the outcome measure based upon prevalence, risk factors of mechanical LBP and the association with backpack. Adolescent girls and children reported higher prevalence. The review reported the use of heavy backpack as dominant risk factor followed by psychological factors and physical inactivity. Only 1 study outlined incorrect posture and structural anomalies as the resulting cause.
CONCLUSION
A positive correlation is found between heavy backpack and childhood LBP. The review exhibits a higher prevalence with increasing age.
Keywords
Low Back Pain, School, Children, Adolescents, Backpacks
Mehek Qamar
Senior Lecturer
Ziauddin College of Physical Therapy
Ziauddin University
Amna Aamir Khan
Assistant professor
Ziauddin College of Physical therapy
Ziauddin University
Muhammad Nadeem
Senior Lecturer
Department of Computer Science
Sir Syed University of Engineering & Technology.
Navaid-us-Saba
Senior Lecturer
Ziauddin College of Physical therapy
Ziauddin University
[Qamar M, Khan AA, Nadeem M, Navaid-us-Saba. Backpacks– Lumbago affect adolescent & children: A Review. Pak. j. rehabil. 2013;2(2):3-9]
INTRODUCTION
Low Back Pain (LBP) is a physical and psychological disorder1 defined as pain limited to the region between the lower margins of the 12th rib and the gluteal folds2. It is one of the most frequent health concern encountered both by adults and children1,3-7. Previously, occupation was considered as a prerequisite of LBP to affect adults and old age, but recently children and adolescents are also being observed as the victims.
Generally, the two most common identified groups of LBP are Mechanical Low Back Pain3 (MLBP) that is non-specific and Non-Mechanical Low Back Pain (NMLBP) characterized by specific low back pain. MLBP is the leading cause among sufferers3. It consists of no underlying pathology or structural anomaly of the back. Spinal joints, vertebrae and soft tissue surrounding the spinal column may act as the source of pain. NMLBP occurs due to definite and identifiable pathological conditions such as spondylolisthesis, kyphosis and scoliosis3. Furthermore, epidemiological studies of past 20 years concluded that, the back pain in children falls mainly under the category of MLBP without any relation to deformity or underlying pathology8.
LBP initiates during childhood2 and constitutes a chief health issue globally4,9. Increasing age escalates the occurrence10 specifically among early teenagers5,11. Interestingly, children experience at least one episode of LBP by the time they reach the age of 14-17 and 5-19% encounters recurrence5. Moreover, 50% are sufferers until the age of 18-20 years8. Life time prevalence for the particular age group is estimated to be 13-51% and point prevalence as 1-33%4. The subject is of an interest to researchers currently, because LBP at an early age leads to persistent pain in adulthood. Patients at age 14 are more likely to develop pain later in life than those without pain earlier on1. One of the most common suggested cause of LBP in children is muscle sprain and strain, that occurs while playing, falling or carrying a heavy school bag8,12. The risk factors for LBP in children are broadly being characterized into the following four sections: psychological, physical, lifestyle and school related factors9.
Considerable research studies conducted to determine the prevalence of LBP among children and adolescents in various countries of the world identify heavy back pack3,7,12-18 as one of the risk factors among many others for developing LBP at a younger age 8,14. The load carried by an 11-year-old child daily to school is 9.3 kg and average maximum is 11.5 kg weekly8. This heavy mechanical load is potentially harmful since it causes negative effects on the posture11,12,14,18, development of spine19 and may result in structural injuries11,14 to the child in addition to pain. The risk of the above-mentioned damage is increased in children less than 15 years as the proportion of their body size, that is, comparatively smaller1. The recommended back pack load bracket is 10-15% of the child’s Body Weight (BW)11,14.
According to a meta-analysis conducted by Damian et al on global prevalence of LBP in June 2012, the overall mean prevalence was found to be 31.0%, whereas annual prevalence being 38.0% and the mean point prevalence is 18.3%20. He revealed that, the frequency of LBP was highest among females and individuals aged between 40-80 years. The prevalence among adolescent population was also shown to be high. It continued to increase throughout adolescent period6, with prior onset predominantly among females2,3,6,11,13,20-22. The early onset onset of puberty in girls is the suggested cause20. In contrast to the studies conducted in other parts of the world, a relatively low prevalence rate of LBP was observed in Pakistan20. The results of mean lifetime prevalence of LBP were 38.9%, contradictory to reviewer’s expectation. The scores were affected specifically by studies conducted in Pakistan, China, Nepal, and Cuba, representing a low and middle income economic countries20. The Meta-analysis reveals a low prevalence of LBP in the above-mentioned developing countries. Higher level of exercise and pain threshold with shorter height was less accessible to industrial insurance while comparing with countries of high-income economies. In addition, methodological factors such as survey planning methods, differing case definitions, age of sample population, gender and barriers to publishing studies may also have influenced the final results20.
The purpose of this research is to systematically review, based on observational findings, the global prevalence of LBP specifically among children and adolescents (both males and females). To determine the causes and risk factors associated with LBP in children of ages 9-18 years. To describe whether carrying heavy back packs is a significant risk factor in causing LBP among school going children or not.
METHODS
Protocol and Registration
This systemic review has been written in accordance with PRISMA statement. The PRISMA check list can be accessed by visiting www.prisma-statement.org
Eligibility Criteria
To be included in the systemic review, the studies had to meet the following criteria-
- The study must be an observational research (epidemiological, cross-sectional or cohort) that reports for non-specific LBP among children, associated significance of backpack carriage and weight of backpack to LBP in children.
- Sample size of minimum 25, both genders included.
- Updated research carried out between 2000 to October 2013, published in national and international journals.
- Studies written in English Language.
- Experimental research studies such as case controls, randomized controlled trials, clinical trials were excluded.
- Any studies related to LBP in adults, specific LBP, published in any other language than English, conducted on single gender, above or below the specified age group, outside the time range provided, incomplete articles or availability of abstracts alone were all excluded from the review.
Information Sources
NCBI, BMJ, Medline, EurMed, Eurspine, Biomed central, Scopemed, Oxford Journals, JPMA, JCE, PAIN, SPINE were the databases searched from 2000-2013. The key words such as low back pain, school, children, adolescents, backpacks, mechanical low back pain and heavy school bag were used during search. Observational research studies and systematic reviews on LBP among children and adolescents were sought.
Search
One of the full search strategies of the database, JCE (Journal of Clinical Epidemiology) is given. Electronic search on web address http://www.jclinepi.com/ for LBP among children and its association with back pack carriage was done using the following items:
- Low back pain in children
- Back pain among children
- Low back pain in adolescents
- Low back pain in children and adolescents
- Back pain in children due to back packs
- Effects of back packs on children
- Systemic review of back pain among children
- Prevalence of low back pain in Pakistan
- Prevalence of low back pain in children
- Prevalence of low back pain among children
- and adolescents
- Low back pain in Pakistani children
- Risk factors of low back pain in children
- Effects of bag pack use in children
Study Selection
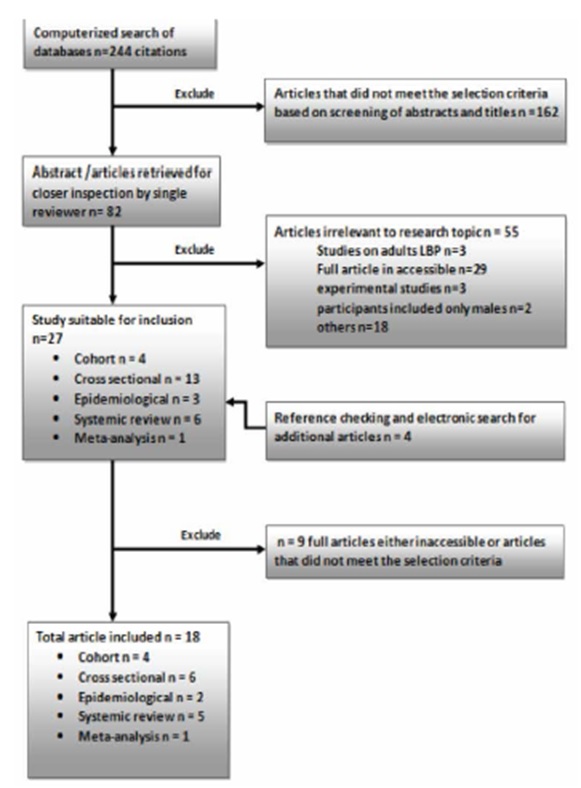
An electronic search of 248 databases was initially performed by a single reviewer using the above given keywords. Research articles were rejected if the main outcome measure was not LBP among children. Based upon the screening, 162 abstracts that did not meet the selection criteria were excluded, that is, LBP studies on adults, experimental trials, articles published in language other than English, participants involving single gender or of age outside the given range, and studies involving treatment of LBP. 27 potentially relevant articles were extracted for a closer inspection by two reviewers. Finally, 18 full text articles fulfilling our selection criteria were included.
Data Extraction and Analysis
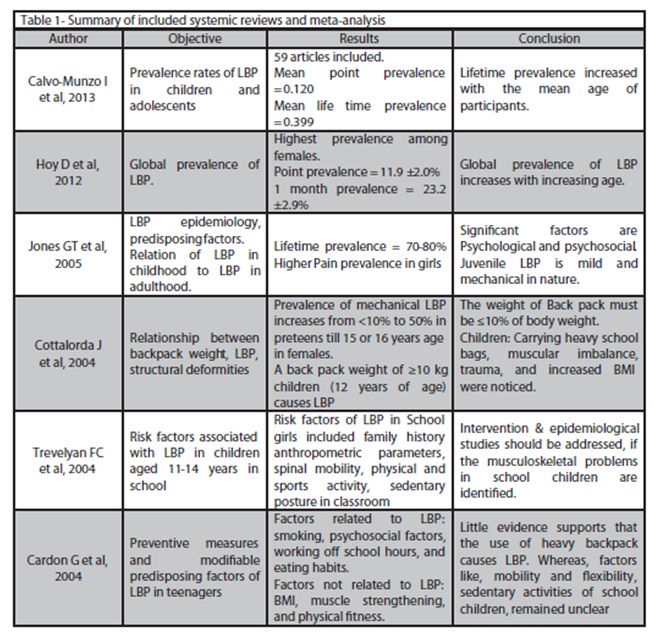
Each article’s year of publication, the number of participants, the first author, the country in which the research was conducted, study type (cross-sectional= CSS, cohort=CS, epidemiological study= ES), results of research, conclusion (describing the outcomes of research and its relation to LBP; risk factors for LBP; significance of backpack or its weight in causing LBP was identified) and study duration were extracted and presented in a tabulated form (Table 1).
Risk of Bias in Individual Studies
Moderate risk of bias may be present in the review. The outcomes were reported and tabulated by a single reviewer. Inclusion, selective reporting, and presentation of few research studies might slightly affect the overall result.
Synthesis of Result
The data was gathered and its summary presented in a tabulated form. The studies selected were performed in different countries of the world. Frequency of articles reporting prevalence rates of LBP, positive relationship of back pack to LBP in children, psychosocial factors, physical inactivity and other risk factors associated with mechanical LBP in children was noted.
RESULTS
Study Selection
Among the 244 databases initially screened on electronic media, 162 were withdrawn on the basis of irrelevance to the research topic. A further of 55 articles from 82 were excluded due to the following reasons: sample inclusive of adult participants (age>18 years) or children of age<9, only abstracts were available, research studies were RCTs, studies published in language other than English, sample inclusive of single gender.
After 27 remaining articles suitable for inclusion, 9 were further exempted from the review as complete text was not available or they did not meet the selection criteria. Finally, a total of 18 articles were included consisting of 4 cohort15,17,23,24, 6 cross-sectional 3-6,13,21,2 epidemiological 14,25, 5 systemic reviews 11,20,22,26,27 and 1 meta analysis2.
Study Characteristics
a) Participants:
This review comprises of participants aged between 9 and 18 years (mean 13.5 years) of both genders. The particular age group being selected since LBP in children is specifically related to possible LBP in adulthood 1,11,19, with 50% of individuals experiencing LBP till reaching 188. There is a rapid growth in LBP with increasing age2,9,11,19,22 principally in females3,6,11,20-22,24,26. Participants under the age of 12 years are referred to as children and considered adolescents if their age is between ages 12 to 18 years6. Psychological1,17,22,23,28 states such as anger, irritation, depression, school related and other mental stress are all related to causing LBP among children1,28. A few other studies suggest muscular imbalance11, trauma6,11, increasing BMI 11,12, carrying heavy school bag3,11-15, poor general health11, physical inactivity5,25, incorrect posture24, spinal mobility, physical and sports activity, duration and posture while sitting in school26, muscle strengthening, smoking, eating habits27 as a potential risk for causing LBP. There was conflicting evidence describing different significant causal factors for LBP in children.
b) Sample Size:
All studies included in the review contained sample size greater than 25.
c) Predisposing Risk Factors:
Time spent on leisure sitting, sleeplessness Risk of Bias within Studies The review included studies conducted in separate countries of the world and disparate research design, each with different objectives and unique outcomes. Observation of such diverse research studies minimizes the effect of bias within the selected studies and their outcome measures.
Synthesis of Results
After close inspection of the selected articles, 18 were incorporated in this review. Consisting articles were 6 cross-sectional studies, 4 cohort, 2 epidemiological, 5 systemic reviews and 1 meta-analysis.
7 out of 18 studies demonstrated high prevalence rates of LBP 2,3,5,13,15,22,24 especially in girls. 6 showed a positive correlation of LBP with heavy backpack use in school children3,11,13-15,26 (2 systemic reviews, 2 cross-sectional studies, 1 cohort and 1 epidemiological study supported heavy back pack use for causing LBP among children). A further 3 (2 cohort, 1 systemic review) emphasized mental health profile as the leading cause of LBP among young individuals17,22,23. 1 cohort study proposed incorrect posture during sleep and structural deformities as reasons for LBP and 2 others, a case-control25 and cross-sectional study related LBP to reduced physical activity in children 5,25.
Summary of Study Selection
DISCUSSION
Among the included reviews given above in table 1, according to the most recent review article on LBP prevalence rates of adolescents and children, the result values were shown as mean point prevalence= 0.120; mean period prevalence (12 months) =0.336; mean period prevalence at one week=0.177 and mean life time prevalence=0.3992, thus affirming the proposed assumption and highlighting the fact that LBP in this particular group persists as a global health issue as well20. The authors’ comparison of their work with the previous ones demonstrated a considerable rise in the research studies on our specific subject2,20. They suggested standardization of LBP definition to aid in upcoming subsequent reviews allowing additional collation between countries and an enhanced understanding of this particular musculoskeletal condition among them20. Nonetheless, irrespective of the number of studies, a major drawback is its type, that is, major of studies belonging to the category of being cross-sectional. As a result, it becomes difficult to differentiate etiology from prognosis27.
The average time a patient spends suffering LBP is greater than three days with a pain score of 4-6 on VAS score indicating moderate intensity pain. This certainly points out the considerable seriousness of LBP symptoms, given the higher pain duration and intensity. Moreover, sufferers reporting pain radiating down the leg also show a greater degree of disability, hence, causing a significant disturbance in their activities of daily living3. Low back health awareness and education is substantial to reduce the effects and prevent LBP altogether4,24.
For the formation of constructive health education or health policy programs directed towards our targeted population; it is necessary first to investigate the health, their health behavior, and the factors influencing them4. Modification of risk factors such as school bag weight7 or physical inactivity25 might prove beneficial, but it is essential to create awareness regarding maintenance of correct back posture whether during activity or at rest24 and practice good ergonomics so as to minimize its occurrence. Irrespective of the cause, 94% of the adolescent LBP sufferers21 experience some kind of disability due to LBP, yet they rarely seek medical assistance 3,21.
Summary of Evidence
The supporting literature was from research carried out in various regions of the globe. The review closely analyzed 18 high quality studies. Diversity of the included evidence proved extremely beneficial. The evaluation of results confirmed the hypothesis that, there is a strong association between mechanical low back pain and students carrying hefty schoolbags 3,11,13,14,15,26 since they affect both health14 and induce changes in posture14,15, both short term and long term. One of the most important findings was the high vulnerability of females to this particular medical condition3,4,6,11,13,21,22,24,26. The proposed reasons being genetics, physical parameters19, increased physical stress and strain to their soft bones at growing age, carrying heavier school bags in comparison with their male counter parts of same age8 and they being more influenced by the parental role model than boys19. Apart from increased mechanical loads, the outcomes also affirm psychological and psychosocial factors as an equally predominant cause of LBP in 9-18 years old individuals 11,17,22,23,26,27. Childhood sufferers are probable victims of MLBP during adult life as well11,21. In addition to the above, advancing age significantly raise the potential of developing LBP2,6,20,22,26 although the severity of pain remained more or less the same and the increase in pain intensity with age was to a lesser extent19. The elucidated crucial risk factors necessitate the elimination or modification if possible. It is fairly substantial to highlight the issue and create awareness among layman. The most successful strategy identified to promote the children’s health, is the school. Health programs conducted at school manifest their compound effect on health problems reduction, improve efficacy of education system and enhance social development. Various health education schemes within the school setting have proven to greatly reduce the incidence of LBP despite its multiple causes. WHO enumerated four key elements in the accomplishment of the goal: a) promoting a healthy environment, b) health education, c) opportunities for physical and recreation, d) offering programs for social support4.
At the moment, limited research is available to evaluate the effectiveness of preventive approach whether at primary or secondary level, to LBP in our selected study group4. Furthermore, whether psychosocial risk factors which also greatly contribute to LBP21,22 in school children are modifiable remains still a question. A distinction between the different psychosocial risk factors is also required27.
Study Limitations
A few methodological limitations accompany this review. Initially, the article searches and selection only included full reported publications in English Language. Research studies published in any other language were discarded. The heterogeneity of included studies resulted in variable outcomes (variation in sample size, resulting LBP prevalence rates, and variety of associated risk factors). Thus, diversity of results may be indicative of incorrect estimates for outcomes.
CONCLUSION
As a strategy to reduce the incidence of LBP at an early age, the weight of the backpack carried daily to school must not exceed 10% of the child’s body weight 11,14. Despite the wide variation in studies, the outcomes showed high prevalence rates of LBP. Mental health of included age group in this review must be considered an area for further investigation. The research on our topic must be carried out in Pakistan as well.
REFERENCE
- Onofrio AC, Silva MC, Domingues MR, Rombaldi AJ. Acute low back pain in high school adolescents in Southern Brazil: prevalence and associated factors. Eur Spine J 2012:21(7);1234-1240.
- Calvo-Muñoz I, Conesa AG, Meca JS. Prevalence of low back pain in children and adolescents: a meta-analysis. BMC Pediatrics 2013:13;14 online available on, http://www.biomedcentral.com/- content/pdf/1471-2431-13-14.pdf
- Dhanesh KKU, Putti BB, Manjula S. Prevalence of mechanical low back pain in school children of adolescent group – An observational study. JARBS 2012;4(3):213-218.
- Jones MA, Stratton G, Reilly T, Unnithan VB. A school-based survey of recurrent non-specific low-back pain prevalence and consequence in children. Health educ Res 2004;19(3):284-289.
- Skoffer B, Foldspang A. Physical activity and low-back pain in school children. Eur Spine J 2008;17(S3):373-379.
- Sato T, Ito T, Hirano T, Morita O, Kikuchi R, Endo N, et al. Low back pain in childhood and adolescence: a cross- sectional study in Niigata City. Eur Spine J 2008;17(11):1441-1447.
- Negrini S, Carabalona R, Sibilla P. Backpack as a daily load for school children. Lancet 1999;354(9194):1974.
- Farhood HF. Low back pain in schoolchildren: the role of school bag weight and carrying way. Journal of Natural Sciences Research 2013;3(8):156-164.
- Habybabady RH, Ansari-Moghaddam A, Mirzaei R, Mohammadi M, Rakhshani M. Efficacy and impact of back care education on knowledge and behavior of elementary school children. J Pak Med Assoc 2012;62(6):580-584.
- Al-Hazza H. School backpack; how much load do Saudi school boys carry on their shoulders. Saudi Med J 2006;27(10):1567-1571.
- Cottalorda J, Bourelle S, Gautheron V. Effects of Backpack Carrying in Children. Orthopedics 2004;27:1172-1175.
- Rai A, Agarawal S. Back Problems Due To Heavy Backpacks in School Children. IOSR-JHSS 2013;10(6):22-26.
- Sheir-Neiss GI, Kruse RW, Rahman T, Jacobson LP, Pelli JA. The Association of Backpack Use and Back Pain in Adolescents. Spine 2003;28(9):922-30.
- Choy JAG, Flores FEG, Merinos O, Cobos FJS, Hernandez MFC, Ramirez PH, et al. An assessment of the anthropometric and external variables that influence the weight of backpacks of junior high school Students. Ergonomia Occupational 2012;5:45-51.
- Negrini S, Politano E, Carabelona R, Tartarotti L, Marchetti ML. The backpack load in schoolchildren: clinical and social importance, and efficacy of a community-based educational intervention. Eur Med Phys 2004;40(3):185-190.
- Negrini S, Negrini A. Postural effects of symmetrical and asymmetrical loads on the spines of school children. Scoliosis 2007;2:8.
- Hulsegge G, Oostrom SH, Susan H, Picavet J, Twisk JWR, Postma DS, et al. Musculoskeletal Complaints Among 11-Year-Old Children and Associated Factors Am J Epidemiol 2011;174(8):877-884.
- Steele E, Bialocerkowski A, Grimmer K. The postural effects of load carriage on young people – a systematic review. BMC 2003;4:12
- Wirth B, Knecht C, Humphreys K. Spine day 2012: spinal pain in Swiss school children-epidemiology and risk factors. BMC Pediatrics 2013;13:159.
- Hoy D, Bain C, Williams G, March L, Brooks P, Blyth F, et al. A Systematic Review of the Global Prevalence of Low Back pain. Arthritis & Rheumatism 2012;64(6):2028–2037.
- Watsona KD, Papageorgioua AC, Jonesa GT, Taylora S, Symmons DP, Silman AJ, et al. Low back pain in school children: occurrence and characteristics. Pain 2002;97(1-2):87–92.
- Jones GT, Macfarlane GJ. Epidemiology of low back pain in children and adolescents. Arch Dis Child 2005;90:312-316.
- Jones GT, Watson KD, Silman AJ, Symmons DPM, Macfarlane GJ. Predictors of Low Back Pain in British Schoolchildren: A Population-Based Prospective Cohort Study. Pediatrics 2003;111:822.
- Kovacs F, Oliver-Frontera M, Plana MN, Royuela A, Muriel A, Gestoso M. Improving School children’s Knowledge of Methods for the Prevention and Management of Low Back Pain. Spine 2011;36(8):505–512.
- Jones MA, Stratton G, Reilly T, Unnithan VB. Biological risk indicators for recurrent non-specific low back pain in adolescents. Br Sports Med 2005;39:137-140.
- Trevelyan F, Legg S. Back pain in school children—Where to from here? Appl Ergon 2006;37:45–54.
- Cardon G, Balague F. Low back pain prevention’s effects in school children. What is the evidence? Eur Spine J 2004;13:663-679.
- Roth-Isigkeit A, Thyen U, Sto ven H, Schwarzenberger J, Schmucker P. Pain Among Children and Adolescents: Restrictions in Daily Living and Triggering Factors. Pediatrics 2005;115(2):e152-62.