
ABSTRACT
BACKGROUND
Metabolic alteration such as acidosis and abnormally high levels of lactate productions are responsible for development of disabilities in polymyositis and dermatomyositis. Interestingly, this has been suggested that by proper aerobic training, combined with muscle strengthening exercises, shows improve aerobic capacity and muscle metabolism.
AIM AND OBJECTIVES
The present study was undertaken to evaluate lactate concentrations in myopathy patients and determines the efficacy of exercise therapy in improving aerobic status of such patients.
MATERIALS AND METHODS
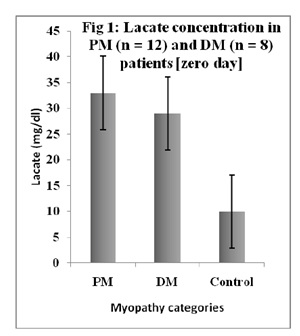
Selected myopathy patients grouped as PM (n = 12 patients) and DM (n = 8 patients). The effects of physical therapy treatments were assessed by lactate estimation at zero, 15th and 28th days.
RESULTS
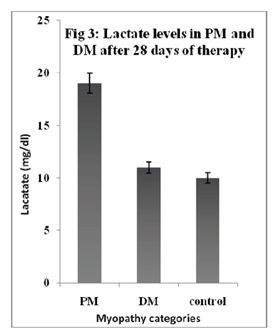
Gradual decline in lactate concentration was noted in both PM and DM group however more prominently in later than in former. The total decline in lactate levels from zero days to 28th day was 42% for PM patients and a considerable 63% for DM patients.
CONCLUSION
It was suggested that estimation of lactate levels in PM and DM patients is of some metabolic importance and physiotherapy treatments did cause improvement in aerobic efficiency of muscles, which was depicted by periodic decline in lactate concentration after 15 and 28 days.
SHORT TITLE
Lactate levels in myopathies
Key Words
Lactate, Polymyositis, Dermatomyositis, Physiotherapy, Aerobic Training Myopathy,
Junaid Mahmood Alam
Department of Biochemistry
Laboratory services
Liaquat National Hospital and Medical College
Sumaira Imran Farooqui
Principal
Ziauddin College of Physical Therapy
Ziauddin University
Amna Hussain
Department of Biochemistry
Laboratory services
Liaquat National Hospital and Medical College
Syed Riaz Mahmood
Govt Lyari General Hospital
Suad Naheed
Jinnah University for Women
Maqsood Ali Ansari
Department of Genetics-University of Karachi
[Alam JM, Farooqui SI, Hussain A, Mahmood SR, Naheed S, Ansari MA. Significance of lactate estimation in debilitated myopathies and treatment programs. Pak. j. rehabil. 2013;2(1):3-5]
INTRODUCTION
Polymyositis (PM) and dermatomyositis (DM), the two characteristic myopathies have idiopathic base, former being distinguished by progressive, symmetric weakness whereas later one by rash accompanied by muscular fragility1,2,3. During past several years, the history of PM and DM and the recommendation regarding their therapy was the topic of many discussion and research work 1,4,5. What was argued after much deliberation is the fact that even after treatments and therapeutic interventions, many of the patients that suffered PM and DM related myopathies, still develops disabilities due to several pertaining and biological factors, one of which is metabolic alteration4 and abnormally high levels of lactate productions6,7. It was suggested by some studies that proper aerobic training combined with muscle strengthening exercises would improve aerobic capacity and muscle metabolism 1,6,7. In this context the present study describes the lactate levels in selected myopathy patients grouped as PM and DM. The effects of physical therapy were also assessed by determining lactate levels at zero, 15 and 28 days after therapy treatments.
MATERIALS AND METHODS
Patients were selected according to described criteria earlier 1,3,8. PM group consist of 12 patients (males = 8, females = 4) whereas DM with 8 (males = 5 and females = 3). The study period was Dec 2006 to November 2009 and multi- centered. No difference was noted in the details of PM and DM in both groups of males and females and thus considered heterogeneous. Where necessary it was advised to the treating physicians to keep the pharmacological interventions, where applicable, constant for the period of exercises and lactate determinations, to avoid bias. Control group of individuals (n = 10) were also went through same exercise regiments as recommended for the PM and DM patients. Exercise treatments were same for all patients as per recommendations of physiotherapy department protocols and where required referred to guidelines provided earlier9. All biochemical and enzymatic components including, creatine kinase (CK), lactate dehydrogenase (LDH), C-reactive protein (CRP) and lactate were determined using standardized methods and commercial kits on Hitachi 912 (Roche Diagnostics, Basil) and Borengier Manheim photometer 1010. Lactate determination was also performed after 15 and 28 days of physiotherapy treatments for comparison. Data were analyzed by using P < 0.05.
RESULTS
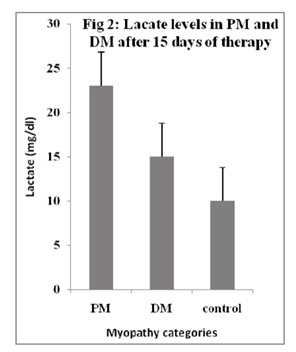
Results are summarized in Fig 1-3. During the entire period of study and exercise regiments, it was ensured that the therapy remained uniform for all patients of PM and DM regardless of gender. It was noted that after 15 days of therapy, lactate levels in PM patients decline around 30% (from 33.2±5.60 mg/dl to 23.45±3.25 mg/dl), whereas nearly 49% in DM patients (from 29.5±3.55 mg/dl to 15.20 ± 2.30 mg/dl), depicting more effectiveness of aerobic status enhancements by exercise therapies in DM than in PM. After 28 days of aerobics and recommended therapy, lactate levels in PM drops further 17%, where as in DM up to further 23%. The total decline in lactate levels from zero days to 28th day was 42% for PM patients and a considerable 63% for DM patients. The lactate levels of control subjects remain comparatively constant during the whole study period (10.10±1.50 mg/dl to 10.70±1.70 mg/dl).
DISCUSSION
It was reported that blood lactate and the H+ it generates were the causative agents of muscle weakness and the oxidative capabilities of muscle fibers 10, 11. Although few studies argued that significance of blood lactate is of no importance, as direct impact of lactate concentration is minimal 12, researchers suggested its importance in declining aerobic capacities of muscle cells, capability force and inducing fatigue, especially in myopathies1,13-15. In addition, certain past and recent studies emphasized that a relationship do exist between muscular fatigue, lactic-acidosis and performance reduction1,16. In a very recent study, it was shown that abnormal lactate concentration is suggestive of impaired muscle activity and oxidative potentials, especially in myopathies related to PM and DM. In another study.
the authors revealed that by increasing muscle strength (through rehabilitation regiments) in patients suffering from mitochondrial myopathies, the system can reduce lactate levels and improve aerobic capacity of muscles 6. In agreement with these two studies conducted a decade apart, the preset study also depicted considerable levels of improvement in oxidative activity of patients, which was apparent by declining levels of lactate after 15 and 28 days of enduring and physiotherapy treatments in PM and DM as groups and also individually. It was noted that after 15 days of therapy, lactate levels in PM patients decline around 30% whereas nearly 49% in DM patients illustrating more efficient aerobic status. Interestingly the decline is more apparent in DM than in PM. Similarly, after 28 days of aerobics and recommended therapy, lactate levels in PM drops further 17%, where as in DM up to further 23%. The total decline in lactate levels from zero days to 28th day was 42% for PM patients and a considerable 63% for DM patients, thus corroborating the scientific suggestions reported earlier 1,6. The outcome of our study and those reported earlier were supported by yet another study where it was documented that specific aerobic exercise treatments can actually reduce lactate concentration by 30% with concurrent increase in aerobic capacity 17.
In conclusion, the present study describes the estimation of lactate levels in PM and DM patients and the improvement in aerobic efficiency of muscles, that was depicted by periodic decline in lactate concentration after 28 days of physiotherapy treatments.
ACKNOWLEDGEMENTS
The author wishes to thank Dr F. Bertolucci and Prof Dr C. Chisari, University Hospital of Pisa, Italy, for providing access to their articles and references, which is a great help in completion of our study. Accessibility to articles of J. Neurosurgery Psychiatry by Prof Dr John M. Pearce is also highly appreciated.
REFERENCE
- Bertolucci F, Neri R, Dalise S, Venturi M, Rossi B, Chisari C. Abnormal lactate levels in patients with polymyositis and dermomyositis: the benefits of a specific rehabilitative program. Eur J Phys Rehabil Med 2013;49:1-9
- Harris-Love MO, Shrader JA, Koziol D, Pahlajani N, Jain M, Smith M, Cintas HL, McGarvey CL, James-Newton L, Pokrovnichka A, Moini B. Distribution and severity of weakness among patients with polymyositis, dermatomyositis and juvenile dermatomyositis. Rheumatology. 2009 Feb 1;48(2):134-9.
- Tanimoto K, Nakano K, Kano S, Classification criteria for polymyositis and dermatomyositis. J Rheumatol 1995;22:668-674
- Alexanderson H. Exercise: an important component of treatment in the Idiopathic inflammatory myopathies. Curr Rheumatol Rep 2005;7:115-124
- Nader GA, Alexanderson H, Grundtman C, Gernapudi R, Esbjorssson M, WangZ, Rönnelid J, Hoffman EP, Nagaraju K, Lundberg IE. A longitudinal, integrated, clinical, histological and MRNA profiling study of resistance exercise in myositis. Molecular Med 2010;16(11-12):455-464.
- Taivassalo T, Gardner JL, Taylor RW, Schaefer AM, Newman J, Barron MJ, Haller RG, Turnbull DM. Endurance training and detraining in mitochondrial myopathies due to single large-scale mtDNA deletions. Brain 2006;129(pt12):3391-3401
- Ziogas GG, Patras KN, Stergiou N, Georgoulis AD. Velocity at lactate threshold and running economy must also be considered along with maximal oxygen uptake when testing elite soccer players during preseason. J Strength Cond Res 2011;25(2):414-419.
- Bohan A, Peter JB. Polymyositis and dermomyositis. N Engl J Med 1975; 292(7):344-347
- Escalante A, Miller I, Beardmore TD. Resistive exercise in the rehabilitation of polymyositis and dermatomyositis. J Rheumatol 1993;20(8):1340-1344.
- Fitts RH. Mechanisms of muscular fatigue. In: editor. Principles Biochemistry. 3. 279–300. Poortmans JR, of Exercise Basel: Karger 2003;
- Sahlin K, Harris RC, Nylind B, Hultman E. Lactate content and pH in muscle samples obtained after dynamic exercise. Pflugers Arch 1976;367(2): 143–149
- Westerblad H, Allen DG, Lannergen J. Muscle fatigue: Lactic acid or inorganic phosphate the major cause? New Physiol Sci 2002;17:17-21.
- Andrews MAW, Godt RE, Nosek TM. Influence of physiological L(+)-lactate concentrations on contractility of skinned striated muscle fibers of rabbit. J Appl Physiol 1996;80(6):2060– 2065.
- Gladden LB. Lactate metabolism: a new paradigm for the third millennium. J Physiol 2004;558:5–30
- Hogan MC, Gladden LB, Kurdak SS, Poole DC. Increased [lactate] in working dog muscle reduces tension development independent of pH. Med Sci Sports Exerc. 1995;27(3):371–377
- Karlsson J, Bonde-Peterson F, Hentiksson J, Knuttgen G. Effects of previous exercise with arms or legs on metabolism and performance in exhaustive exercise. J Appl Physiol 1975;38(5):763-767.
- Taivassalo T, de Stefano N, Argov Z, Matthews PM, Chen J, Genge A, Karpati G, Arnold DL. Effects of aerobic training in patients with mitochondrial myopathies. Neurology 1998;50(4): 1055-1060.