
Maliha Khalid[i], Syed Asadullah Arsalan[ii], Sahar Fatima[iii], Muhammad Musa Asif[iv], Syeda Nabiha Zafar[v]
DOI: 10.36283/pjr.zu.11.2/015
ABSTRACT
Background and Aim: The Fear of Falling Scale (FES-I) was created to investigate people’s concerns of falling. It has 16 elements that should be translated into comprehensible Language to avoid misperceptions. The purpose of this research was to provide an Urdu translation of the fall’s effectiveness scale-International and evaluate its psychometric characteristics.
Methodology: The FES-I was translated using Beaton standards. A final FES-I was produced once forward and backward translations were completed. Adults aged 60 and up from the community of Lahore’s old houses were recruited. Internal consistency and test re-test reliability were evaluated. The Urdu version of the FES-I was compared to the Berg Balance Scale and the Time Up and Go Test to determine its validity.
Results: With 100 respondents, the Urdu – FES-I shows a good test-retest reliability (ICC = 0.989). With a Cronbach’s alpha score of 0.989, FES-I-U has high internal consistency. The construct validity between the FES-I-U and Time Up and Go revealed a good positive correlation when Pearson’s correlation coefficient was calculated. There is a substantial negative correlation between the FES-I-U and the Berg Balance Scale.
Conclusion: The FES-I in Urdu is a clear, valid, and reliable instrument for measuring fear of falling among older Pakistani community.
Keywords: Falls efficacy scale-international, risk of fall, berg balance scale, time up and go test, translation, psychometric testing.
Introduction
Language barriers in the healthcare sector can lead to misunderstandings and errors in care, particularly when circumstances force health care workers or patients to communicate in a language other than their native tongue or national language. Language improvement should be prioritized everywhere in the globe, including in Pakistan1. There are several languages spoken and understood in Pakistan, but Urdu is the national language and the most frequently well-spoken recognized. Keeping this in mind, the current study collected data on the likely to fall amongst elderly people using the Urdu language2.
The initial risk factor for the occurrence or recurring of falls in the elderly is the original fear of falling, as well as the impaired aspect that restricts physical functioning and daily living standards3. Fears of falling is a frequent phobia that relates to an excessive fear of falling or noticeably diminished confidence while doing mobility activities, and, in its most severe form, it generates anxiety. Falls-related injuries have become a major public health concern4. Falls contribute to an increased death and sickness rate, and they have also become a leading cause of inactivity among the elderly. Patients above the age of 60 had the greatest death and morbidity rates related to fall injuries5,6.
The European Prevention of Falls Network created the FES-I to assess the risk of falling or worries about falling7. The FES-I consists of 16 measures, comprising 10 old FES items and six additional items that provide access to more challenging physical and interpersonal activities8. In several nations, The FES-I has been used to assess fear of falling in a variety of senior individuals and has been considered as a reliable and valid instrument for assessing risk of falls in the older population9.
Cleaning the house (e.g., washing the cloth, vacuuming, or dusting), getting dressed and undressed., preparing common meals, showering and bathing, going shopping, walking up and down the stairs, sitting or standing from a chair, walking around the neighborhood., reaching to grasp things above or from the ground, picking up the phone., paying a visit to a friend or relative, walking on a wet or glossy surface (for example, moist ground)., and (e.g., family gathering, club meeting or religious act), form the 16 items of FES-I The total score goes from 16 to 64 points9,10.
Although the FES-I scale has been translated into over 15 languages, it has not yet been culturally adapted for usage in Pakistan. This scale was translated into Urdu for Pakistani community-dwelling older persons in this study. The transcultural reliability and validity of an Arabic version of the FES-I, according to Hadeel Halaweh et al., revealed that it had high reliability and internal consistency11. Eva Kovacs et al. cross-culturally verified the Hungarian version of FES-I in another investigation12. A total of 165 people participated in the study and filled out the questionnaire. Internal consistency and dependability were found to be quite high in the retest. The alpha value for Cronbach’s alpha was 0.95. 0.831 was the intra-class correlation coefficient. The Hungarian FES-I has shown to be a trustworthy and dependable instrument, indicating that it may be utilized in clinical and scientific studies with Hungarian seniors in the future.
The Turkish version of the FES-I was culturally modified, according to Yasemin Ulus et al. The sample size was 70 participants, ranging in age from 65 to 81 years old. The Turkish FES-I had a Cronbach’s alpha of 0.94, while the individual item ICCs varied from 0.97 to 0.99. TUG, MBI, and BBS were favorably linked with final results of Turkish version of the questionnaire, whereas Time up and Go, MBI, and Berg balance scale were negatively correlated. The references values to distinguish amongst people who are afraid of falling and those who are not was 24 points. The Turkish version of the Falls Efficacy Scale International was proven in Turkish geriatrics to be a meaningful and accurate indicator of fear of falling [13].
Methodology
Stage 1: The Process of Translation and Cross-Cultural Adaption
Step I: Translation Into Urdu: In the initial step, two forwards translations of the tool from the original language to Urdu were accomplished. The two independent translations were made by bilingual translators with different profiles and backgrounds in order to achieve the best feasible outcomes. One of the translators was familiar with the themes covered in the questionnaire being translated. He was able to provide a more exact scale translation because he was a doctor[14]. The other translator has no prior knowledge of the notions being quantified and, ideally, has no background related to medicine or clinical study. This is considered a basic translation, and the translator was probably than the initial translator to notice differences in the original meaning.
Step II: Putting These Translations Together: In step 2, the third unbiased individual created a synthesis of two translations. The original questionnaire, and the first translator’s edition (T1) as well as the second translator’s variant (T2), were used to create a third translation (T2), resulting in a common translation (T12).
Step III: Reverse Translation: The survey tool was then re-translated into the target English by a translator who proceeded from the T-1, 2 survey forms and had no knowledge of the scale’s original state. This is a method that ensures the translated edition includes the same data as the original[15]. It’s the most efficient way to point out major discrepancies or conceptual mistakes in translation. Two additional back translations were carried out. Back-translations were created by two individuals who know English as their native language (BT1 and BT2). To avoid bias, the two linguists were not provided any knowledge regarding scale concepts.
Step IV: Committee of Experts: This committee’s direction is critical. Experts in the subject, healthcare professionals, language experts, and translators who have been involved thus far make up the committee. Throughout this process, the questionnaire’s original writers communicate with the expert committee on a regular basis. The goal of this committee is to gather together all of the different versions of the questionnaire and create a final draft for field testing. The committee looked over all of the translations and came to an agreement on any differences.
Step V: Preliminary Version Testing: At this stage, the feasibility of a pre-final Urdu version of FES-I was assessed. Ten senior citizens were chosen, and each completed the questionnaire independently and without assistance, as well as was questioned about their thoughts and replies to each questionnaire item. This guaranteed that the revised version remained functional in a real-world situation[15].
Step VI: documentation is submitted to the decision committee to review: The adaption procedure came to a close with the submission of reports and forms to the committee. The committee makes certain that all of the necessary steps are taken and that the procedure is accurately documented in the reporting16.
Stage 2: The Process of Testing the Psychometric Properties
The total number of participants in the study was 100, which was calculated using the Kline technique17, with 52 men and 48 women participating. The data was obtained with the consent of the Institutional Review Board of the University of Lahore(IRB). All actions were followed strictly according to the rules and regulations. Before the data was gathered, all the members involved in the study agreed to a written consent form. To be considered, patient must be over 55 years old. They must be native Urdu speakers who can understand and fill out the questionnaire. They should be able to walk around the house independently, with or without the use of walking aids (non-human)9. Exclusion criteria included communication difficulties, illiteracy, dependent indoor ambulation, substantial cognitive and mental impairment, and alcohol misuse.
Testing and Participants: 100 community-dwelling older persons completed the Falls Efficacy Scale International in Urdu with Berg Balance Scale, TUG test for balance. The pre-test stage’s patient addition or removal from the study was followed using the same standards as before.
Reliability: FES-I-Urdu version’s reliability was evaluated on 100 senior people. During their initial visit, the individuals were required to complete the FES-I-Urdu, BBS, and TUG. Other demographics were recorded as well. The same participants were re – evaluated in the same manner 48 hours later by completing the FES-I-Urdu, BBS, and TUG. During this time, the subject received no therapy of any kind. To measure test-retest reliability, ICC was computed at a 95% CI. ICC values vary from 0 to 1, with 0 being the lowest and 1 being the highest. Based on 95 percent confidence intervals, the reliability of ICC estimation could be poor, moderate, or high with values of 0.5, 0.5-0.75, 0.75-0.9, and > 0.90. Cronbach’s alpha scores and item total correlation were used to measure the FES-I Urdu’s internal consistency.
Validity: The correlation between the FES-I Urdu and the Berg Balance Scale, TUG Test was used to determine convergent validity. Very low correlation is shown by r = 0–0.25; low correlation is shown by r = 0.26–0.49; moderate correlation is seen by r = 0.5–0.69; high or strong correlation is shown by r = 0.7–0.89; extremely high or very strong correlation is shown by r = 0.9–1.018.
Analyzing the Data: The data was analyzed with SPSS version 23, which included quantitative aspects like mean and SD as well as categorical data like frequency and percentage. The intra-class correlation coefficient (ICC2,1) and 95 percent confidence intervals were used to investigate reliability across repeated measures, internal consistency, and measurement error (CIs). The significance threshold is less than 0.05. Internal consistency was determined using Cronbach’s alpha.
Ethical Concerns
The data was gathered with the permission of the University of Lahore’s Institutional Review Board. The study was conducted in the private universities of Lahore within the 9 months after the approval from the ethical committee (Jan 21- Oct 21). All acts were carried out in strict accordance with the established laws and rules. All participants in the study signed a permission form before the information was acquired.
Results
Cultural Adaptation and Translation
Urdu is a language spoken in Pakistan. Face validity of the pre-final version of FES-I was evaluated on twenty participants; these participants were compromised of both male and female representation, ranging in age from 60 to 90. Major modifications were not made throughout the translation to keep the translated version near to the FES-I original survey. Overall imprint of this translated Urdu version of the FES-I was that it was simple to understand and complete all of the questionnaire’s questions. All of the objects and questions were relevant to the topic it was measuring. As a consequence, there were no significant changes in the pre-test findings of the Urdu version of FES-I.
Testing For Reliability
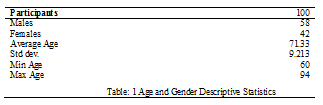
A total of 100 patients were involved in this research. Patients were 53.68 years old in mean. There were 54 men (46.20 percent) and 63 females (53.80 percent). Table 1 shows demographic data whereas the Table 2 reviews reliability statistics of the translation. The test-retest reliability of the FES-I(U) has been outstanding. Internal consistency was determined to be excellent, as all of the findings above Cronbach’s alpha’s suggested standard (0.80). The range of values (0.60–0.80) was deemed suitable, while outcomes of 0.80–0.95 were regarded good19.
Testing For Validity
When Pearson’s correlation coefficient was determined, the construct (convergent) validity between the FES –Urdu and TUG Test showed positive correlation. Amongst FES Urdu and BBS, there was a substantial negative connection.
Discussion
FES-I has been translated into multiple other languages and their validity and reliability has been proved in those languages . These translations include Norwegian12, Greek20, Turkish13, Dutch, Portuguese21, Persian22, Swedish23, Arabic24, and Chinese25 languages.
The FES-I Urdu version was shown to be an effective instrument for assessing the risk of falling in older people in this study. The “Multicultural adaption of FES-I into Urdu” is provided in this paper. To begin with, this instrument was translated into Urdu in order to control its “psychometric characteristics” among senior respondents. The FES-I-U was then utilized among the elderly. This tool was used again after 48 hours to ensure its authenticity26. The FES-I (Urdu translated variant of FES-I) was shown to have reasonable reliability and coherency, as well as good psychometric features in older people. To all demographics, the Urdu version FES-I appeared to be well comprehended and straightforward in comprehension.
Typically, this type of study is performed when we are attempting to make adjustments to a standard instrument in order to eliminate cultural variations and their validity and reliability. Forward and reverse translations were part of a step-by-step translation procedure. A review group was formed to examine the most recent edition of FES-I critically. Decisions were taken after various phases in the translation process. A total of 100 senior people, both men and women, were enrolled in the research.
In this study, 48 percent of men and 52 percent of women were recruited, which is similar to prior polls. Several studies, however, have included more women than men. Patients with somewhat significantly lower scores for age were enrolled in some of the other studies, while the average age in the current study was 71.33 years.
The most challenging tasks in this study were walking over slick plane area and walking on an rough place. These findings are in line with those of other researches. When this was compared with the actual version of the original FES-I, the observed scores of these two additional items reflected more demanding tasks in the FES-I show that there is a need for such a refined instrument27.
All of the a priorly established hypotheses were verified in the current investigation, indicating that the FES-I has excellent construct validity. Fear of falling as a single category issue was shown to be strongly associated with the entire FES-I score, which is consistent with previous research. The FES-I total score and TUG had a substantial positive correlation[28], showing that higher FES-I scores may represent reduced mobility and independence among community-dwelling elderly. The danger of falling increases as the TUG score rises, and the chance of falling also rises as the falls efficacy scale score rises.
When Pearson’s correlation coefficient was determined, the construct (convergent) validity between the Falls Efficacy Scale International –Urdu and TUG Test showed good positive correlation. According to TUG analysis, people with greater recorded FES-I scores may be at a higher risk of falling. The TUG test took more than 14 seconds for those who scored considerably better on the FES-I. Between FES-I-U and BBS, there was a substantial negative connection.
By comparing the scores from the first and second readings of the FES-I, test–retest reliability was investigated. the ICC calculates the test–retest reliability, which is a measure of a measurement’s repeatability. The FES-I Urdu’s Intra-class Correlation Coefficient proved its high dependability. The Urdu – FES-I has high test-retest reliability (ICC = 0.989) with 100 responders. FES-I-U has excellent internal consistency, with a Cronbach’s alpha score of 0.989 (= 0.98). The item total correlation score was 0.978, indicating that the FES-I-U is internally consistent.
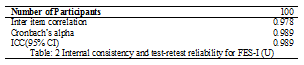
Internal consistency (Cronbach’s) of the FES-I total score was computed as 0.989 to improve international comparability of reliability ratings. This finding is close to the FES-original version (0.96) as well as research in Greece (0.92), Turkey (0.94), and China (0.95). (0.94). This shows that the findings of this study are consistent with those of other relevant studies looking at the FES-I in diverse groups.

The analysis’ main strength was that they looked at the psychometric characteristics of the FES-I Urdu, as opposed to previous research that used pre-defined hypotheses. It was the sole study investigation that the writer understood that computed item total correlation could be utilized to evaluate the scale’s internal consistency.
Conclusion
The FES-I was shown to be an understandable, valid, and reliable tool for assessing fear about falling amongst community-dwelling senior Pakistanis. The FES-I might be utilized effectively in clinical settings, academics and studies to come to measure fear of falling in Urdu-speaking elderly people.
References
- Al Shamsi H, Almutairi AG, Al Mashrafi S, Al Kalbani T. Implications of Language Barriers for Healthcare: A Systematic Review. Oman Med J 2020; 35(2): e122.
- Fatima S, Arslan SA, Sharif F, Ahmad A, Gillani SA, Zaheer A. Translation, cross-cultural adaptation and psychometric properties of the Urdu version of knee injury and osteoarthritis outcome score questionnaire for Pakistani population. BMC Musculoskeletal Disorders 2021; 22(1): 1-7.
- Lindh-Rengifo M, Jonasson SB, Mattsson N, Ullén S, Nilsson MH. Predictive Factors of Concerns about Falling in People with Parkinson’s Disease: A 3-Year Longitudinal Study. Parkinsons Dis 2019; 2019: 4747320.
- Kantow S, Seangpraw K, Ong-Artborirak P, et al. Risk Factors Associated with Fall Awareness, Falls, and Quality of Life Among Ethnic Minority Older Adults in Upper Northern Thailand. Clin Interv Aging 2021; 16: 1777-88.
- Luk JK, Chan T, Chan D. Falls prevention in the elderly: translating evidence into practice. Hong Kong Med J 2015; 21(2): 165-71.
- James SL, Lucchesi LR, Bisignano C, et al. The global burden of falls: global, regional and national estimates of morbidity and mortality from the Global Burden of Disease Study 2017. Injury Prevention 2020; 26(Suppl 2): i3.
- Yardley L, Beyer N, Hauer K, Kempen G, Piot-Ziegler C, Todd C. Development and initial validation of the Falls Efficacy Scale-International (FES-I). Age and ageing 2005; 34(6): 614-9.
- Gazibara T, Stankovic I, Tomic A, et al. Validation and cross‐cultural adaptation of the Falls Efficacy Scale in patients with Parkinson’s disease in S erbia. Geriatrics & gerontology international 2013; 13(4): 936-41.
- Marques-Vieira CMA, Sousa LMM, Severino S, Sousa L, Caldeira S. Cross-cultural validation of the falls efficacy scale international in elderly: systematic literature review. Journal of Clinical Gerontology and Geriatrics 2016; 7(3): 72-6.
- Fabre JM, Ellis R, Kosma M, Wood RH. Falls risk factors and a compendium of falls risk screening instruments. Journal of geriatric physical therapy 2010; 33(4): 184-97.
- Halaweh H, Svantesson U, Rosberg S, Willen C. Cross-cultural adaptation, validity and reliability of the Arabic version of the Falls Efficacy Scale-International (FES-I). Medical principles and practice 2016; 25(1): 1-7.
- Kempen GI, Todd CJ, Van Haastregt JC, et al. Cross-cultural validation of the Falls Efficacy Scale International (FES-I) in older people: results from Germany, the Netherlands and the UK were satisfactory. Disability and rehabilitation 2007; 29(2): 155-62.
- Ulus Y, Durmus D, Akyol Y, Terzi Y, Bilgici A, Kuru O. Reliability and validity of the Turkish version of the Falls Efficacy Scale International (FES-I) in community-dwelling older persons. Archives of gerontology and geriatrics 2012; 54(3): 429-33.
- Povoroznyuk R, Dzerovych N, Povoroznyuk V. A new voice: translating medical questionnaires. Journal of World Languages 2016; 3(2): 139-59.
- Beaton D, Bombardier C, Guillemin F, Ferraz MB. Recommendations for the cross-cultural adaptation of health status measures. New York: American Academy of Orthopaedic Surgeons 2002; 12: 1-9.
- Lipardo DS, Leung AY, Gabuyo CMA, et al. Cross-cultural adaptation and psychometric properties of the Falls Efficacy Scale–International in Filipino community-dwelling older adults. Disability and rehabilitation 2020; 42(9): 1292-8.
- Kline RB. Principles and practice of structural equation modeling: Guilford publications; 2015.
- Munro BH. Statistical methods for health care research: lippincott williams & wilkins; 2005.
- Taber KS. The use of Cronbach’s alpha when developing and reporting research instruments in science education. Research in science education 2018; 48(6): 1273-96.
- Billis E, Strimpakos N, Kapreli E, et al. Cross-cultural validation of the Falls Efficacy Scale International (FES-I) in Greek community-dwelling older adults. Disability and rehabilitation 2011; 33(19-20): 1776-84.
- Figueiredo D, Santos S. Cross-cultural validation of the Falls Efficacy Scale-International (FES-I) in Portuguese community-dwelling older adults. Archives of gerontology and geriatrics 2017; 68: 168-73.
- Baharlouei H, Salavati M, Akhbari B, Mosallanezhad Z, Mazaheri M, Negahban H. Cross-cultural validation of the Falls Efficacy Scale International (FES-I) using self-report and interview-based questionnaires among Persian-speaking elderly adults. Archives of gerontology and geriatrics 2013; 57(3): 339-44.
- Nordell E, Andreasson M, Gall K, Thorngren K-G. Evaluating the Swedish version of the falls efficacy scale-international (FES-I). Advances in Physiotherapy 2009; 11(2): 81-7.
- Alghadir AH, Al-Momani M, Marchetti GF, Whitney SL. Cross-cultural adaptation and measurement properties of the Arabic version of the Fall Efficacy Scale International. Neurosciences Journal 2015; 20(3): 230-5.
- Kwan MM, Tsang WW, Close JC, Lord SR. Development and validation of a Chinese version of the Falls Efficacy Scale International. Archives of gerontology and geriatrics 2013; 56(1): 169-74.
- Mijnarends DM, Meijers JM, Halfens RJ, et al. Validity and reliability of tools to measure muscle mass, strength, and physical performance in community-dwelling older people: a systematic review. Journal of the American Medical Directors Association 2013; 14(3): 170-8.
- Stenhagen M, Ekström H, Nordell E, Elmståhl S. Both deterioration and improvement in activities of daily living are related to falls: a 6-year follow-up of the general elderly population study Good Aging in Skåne. Clinical interventions in aging 2014; 9: 1839.
- Shumway-Cook A, Brauer S, Woollacott M. Predicting the probability for falls in community-dwelling older adults using the Timed Up & Go Test. Physical therapy 2000; 80(9): 896-903.
The Ziauddin University is on the list of I4OA (https://i4oa.org/) & I4OC (https://i4oc.org/).
![]() This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY 4.0). https://creativecommons.org/licenses/by/4.0/
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY 4.0). https://creativecommons.org/licenses/by/4.0/
Conflict of Interest: The author (s) have no conflict.
[i] Physical Therapist University Institute of Physical therapy
ORCID ID: 0000-0001-7803-9675
[ii] Head of department University Institute of Physical therapy
ORCID ID: 0000-0003-3492-7050
[iii] Lecturer University Institute of Physical therapy
ORCID ID: 0000-0002-2662-8213
[iv] Physical Therapist University Institute of Physical therapy
ORCID ID: 0000-0001-7569-2927
[v] Physical Therapist University Institute of Physical therapy, University of Lahore
ORCID ID: 0000-0001-8993-5504