
Dr.Amna Shahid[i], Dr.M Faheem Afzal[ii], Dr.Adeela Arif[iii], Dr.Javed Ali[iv]
DOI: 10.36283/pjr.zu.11.2/005
ABSTRACT
Background and Aim: Hemiplegic cerebral palsy children presented with wide variations of lower limb kinematics. The normal limb in children with spastic hemiplegic cerebral palsy shows variations in Q angle. So, this study aimed to determine the different values of Q angle from both legs among hemiplegic cerebral palsy children having age between the 7 to 12 years.
Methodology: An observational cross-sectional study was conducted by using non-probability convenience sampling technique. 71 diagnosed cases with unilateral cerebral palsy in Mobility Quest clinic Lahore and Children Hospital Lahore were enrolled in the study during the duration of six months from September 2019 to March 2020. The consent was taken from those subjects who fulfill the inclusion criteria (n=71) and assessed by the Goniometer that is used to measure the Q angle in hemiplegic Cerebral palsy. Data entry and analysis was done by using SPSS version 25. Descriptive measures of mean and standard deviation were used to summarize data collection.
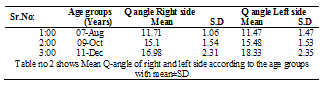
Results: The study included 71 children diagnosed with unilateral cerebral palsy. The Mean Q angle for hemiplegic CP children in right leg is 14.65 ± 2.8 (Normal Range: 11.71-16.98) and in left leg it is 15.09 ± 3.4(Normal Range: 11.47 -18.33) but it differs with the distribution pattern of hemiplegia. Out of 71 children 39 kids were experienced with right sided weakness while 32 were with left sided weakness.
Conclusion: Mean Q angles are higher in the affected leg as compared with the unaffected leg in hemiplegic CP. Q angle increase with age and more in female subjects as compared to male subjects.
Keywords: Hemiplegia, Q angle, quadriceps muscle, spastic perebral Palsy, adolescent
Introduction
Cerebral palsy (CP) is a static injury to the immature brain that covers disorders related to movement and posture and is often associated with other sensory and cognitive disabilities1. It has been reported that more than one and half greater than four of each of thousand’s birth are labeled with cerebral palsy2. According to a study that conducted in Pakistan about the prevalence of CP showed that out of 20 cases, 15 (75%) had spastic type of cerebral palsy, which was further classified as diplegia 7 (35%), quadriplegia 6 (30%) and hemiplegia 2 (10%). Mixed and dystonic types were found in 3 (15%) and 2 (10%) children respectively3. In Unilateral spastic CP, half side the body goes into weakness. These children mostly exhibit better intellectual abilities and may achieve good levels of motor skills depending on the different levels of severity like mild, moderate and severe4.
Hemiplegia occurs due to perinatal insult such as prematurity, birth asphyxia, birth trauma and perinatal infection and as well as due to infection, trauma and developmental abnormalities5. Spastic hemiplegia children develop walk and commonly showed a toe walking pattern due to over contracted planter flexors. The hemiplegic extremities showed limb discrepancies comparative on the unaffected side not cause of disuse or hyper tonicity but as a result of abnormal development due to the cerebral injury6, 7.
Among variables in lower limb, the Quadriceps angle studied often, that explained as the angle between two lines: one from anterior superior iliac spine to the knee cap and a second line from the patella center to the tuberosity of tibia8.
In assessing the knee joint function Q angle is an important determinant. Pathological conditions such as chondromalacia and dislocations of patella exhibit greater Q angle values and greater Q value increase the pronation of foot9. Changes in Q angle can lead to gait problems and increased chances of injuries. According to the evidence mostly studies were focused on Q angle variation among adults but limited studies were found on children. The average range of Q angle for children aged between 7 and 12 years is: males – 15.7 ± 4 (range: 10–17) and females – 15.8 ± 3.4 (range: 10–19)10. Unilateral spastic CP children may present a short leg on the hemiplegic side that affect negatively the kinematic of the normal limb. The normal limb in children with spastic hemiplegic CP shows abnormalities mainly in hip and knee joint movements resulting in increased flexion. Unilateral CP kids may develop a calcaneovalgus deformity on the unaffected side11.During movement of the leg Q angle is play an important function in equal distribution of weight bearing. During the functional activities of lower extremities, the Q angle and biomechanical stress is directly proportional to each other. Quadriceps, Hamstrings, Iliotibial band and gastrocnemius muscles show tightness during the high biomechanically challenged activities12, 13.
It is evident that leg position may change the bony points used for the Q angle, with the reference of the position of tibia and femur. Biomechanically the toes turned inward when the tibia is internally rotated. Among the children of younger age generally shows external tibial rotation. It is mostly one sided and more common on the right14. Anatomically the adults have usually less Q angle values as compare to adolescents.15 The quadriceps angle is highly sensitive to error in the defining the anatomical landmarks16. It is very important for lower limb posture. Normal values of quadriceps angle assessment may predict the probable factors which have direct effect on the knee functions17.
Stability of the posture may be dynamically challenged by malalignment of lower extremity18. Individuals who experienced altered lower extremity posture leads to potential injuries to the knee joint or any weight bearing joint of the body19 Q angle is an important predictor for lower limb injuries in any population who experienced changed biomechanics20.
There is lack of evidence that describes the variation of Q angle occur in preadolescent children with hemiplegic cerebral palsy. The Q angle is highly sensitive to error in the defining the anatomical landmarks. So, the objective of the study was to determine the Q-angle variations in preadolescent children with hemiplegic cerebral palsy.
Methodology
Subject
This observational cross-sectional study was conducted at Mobility Quest Center and children hospital Lahore in the duration of 6 months from September 2019 to March 2020. Seventy-one sample size was calculated through Rao soft with the population of 10% by using the formula n = (Z_ (1-α/2) ^2 P (1-P))/d^2). 11
All the children with abnormalities of tone, movement and posture diagnosed as hemiplegic cerebral palsy were included in the study. Inclusion Criteria of the study was Children diagnosed with hemiplegic Cerebral Palsy, Children were 7 to 12 years of age, Children who were able to understand and communicate properly and hose Children who scored Gross Motor function Classification System (GMFCS) level I-II.
Exclusion criteria for this study were Children with history of epilepsy and with sight and hearing problems and children who had undergone prior orthopedic surgery at lower limbs. The study was started after taking approval from hospital ethical committee and making sure that there was no ethical issue involved in this study. A written consent form was given to parents of each child and confidentiality was highly maintained.
Procedure
Data was collected from 71 children between 7 -12 years of age from two settings. Written informed consent was received from the parents to permit their children to take part in the study. Demographic data of children were recorded. A physical therapist assessed the children using the Gross Motor Scale. Data was collected by measuring Quadriceps angle with the use of goniometer. Q angle was assessed with children in lying position to maintain homogeneity of the data.
Measurement of Q Angle
The Quadriceps angle was recorded by the use of goniometer with children lying supine and legs in relaxed position. The anatomical land marks ASIS, center of patella and tibial tuberosity was highlighted with pen. The highlighted point at ASIS and midpoint of patella were linked with to ensure precise alignment of goniometer. The center of goniometer placed on center of patella with its fixed arm positioned at tibial tuberosity and adjustable arm on ASIS. Measurement was recorded between two arms of goniometer.
Data Collection Tools
After collecting demographic data, measurement of Q angle was taken by the use of the goniometer of normal and affected side of hemiplegic Cerebral palsy in supine lying.
Data Analysis
SPSS version 25 was used to analyze the data, variables like age, mean Q angle values according to age were presented as mean±SD, and the data was depicted using percentage and frequency measurements.
Ethical Concerns
The study will be started after taking approval from hospital ethical committee and making sure that there is no ethical issue involved in this study. A written consent form will be given to parents of each child and confidentiality will be highly maintained.
Results
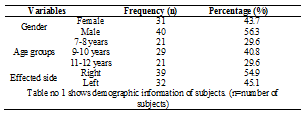
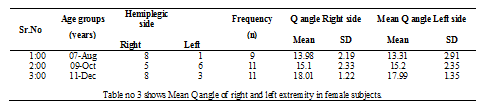
The study included 71 children diagnosed with unilateral cerebral palsy. Out of 71 children of 9 females and 12 males in 7-8 age group and 11 females and 18 males in the 9-10 age group and 11 females and 10 males in 11-12 of age groups. All cases were categorized into three age groups. 29.6% were included in 7-8 age groups, 40.8% were included in9-10 years and 29.6% were included in 11-12 years of age group. Out of 71 children 39 kids were experienced with right sided weakness while 32 were with left sided weakness.
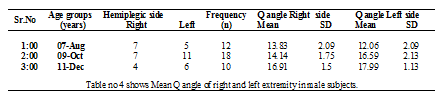
This study also recorded mean Q angle value in females and males separately according to age ranges. Mean Q angle of males in age range of 7 to 8 years was 13.83 ± 2.09 in right leg and 12.06 ± 2.09 in left leg (7 were right sided and 5 were left sided hemiplegic). Mean Q angle in males aged between 8 to 9 years was 14.14 ± 1.75 in right leg and 16.59 ± 2.13 in left leg (7 were right hemiplegic and 11 were left sided weakness). Mean Q angle in males aged between 11 to 12 years was 16.91 ± 1.50 in right leg and 17.99 ± 1.13 in left leg (4 were presented with right sided weakness and 6 were left sided hemiplegics.
Discussion
The present study shows the Q angle values in different age groups ranges between 7-12 years with the respective side affected by the hemiplegia. Above findings were focused to find out Q angle values in both legs of diagnosed cases of hemiplegic CP. These findings showed that Q angle values increases with the age, lower in 7 to 8 years of age group and higher in 11 to 12 years of age and these findings were similar with the previous study22.
Another study was conducted on Q angle related with the age and activity shows that Q angle increases with age because of increase quadriceps strength as it straightens the Q angle23.
The present study shows that Q angle is relatively high in hemiplegic leg as explained as it all because of lateral tracking of patella and changes of foot and most importantly foot pronation considered as major factor to change the alignment of lower extremity. These results were consistent with the study conducted on the Q angle measurement24.
There is study conducted on health children with age 2 to 8 and concluded that positional change and weight bearing did not change the position of knee.25 .Values of Q angle higher than 15 degrees in male and 20 degrees in females are considered abnormal for adults and Q values lower than 10 degrees are also not a healthy may cause knee pain or patellar and foot issues in future26.
Conclusion
Value of Q angle in children aged from 7 to 12 were more than normal range. With increase in the age there is increase in values of Q angle in children of both the sexes. The Q angle was higher in affected side as compared to normal leg.
References
- Van Gorp M, Hilberink SR, Noten S, Benner JL, Stam HJ, van der Slot WM, Roebroeck ME. Epidemiology of cerebral palsy in adulthood: a systematic review and meta-analysis of the most frequently studied outcomes. Archives of Physical Medicine and Rehabilitation. 2020 Jun 1;101(6):1041-52.
- Anderson LL, Larson SA, MapelLentz S, Hall-Lande J. A systematic review of US studies on the prevalence of intellectual or developmental disabilities since 2000. Intellectual and developmental disabilities. 2019 Oct;57(5):421-38.
- Ortiz AÁ, Cuesta HV, Pelier BY, del Valle AE, Rodríguez EM, López YP. Physical activity in the motor recover of the children with spastic brain palsy. Investigaciones Medicoquirúrgicas. 2019;11(S1).
- Pinto TP, Fonseca ST, Gonçalves RV, Souza TR, Vaz DV, Silva PL, Mancini MC. Mechanisms contributing to gait speed and metabolic cost in children with unilateral cerebral palsy. Brazilian journal of physical therapy. 2018 Jan 1;22(1):42-8.
- Eyong K, Torty C, Asindi A, Ekanem E. Acute hemiplegia: aetiology and outcome in Nigerian children. The Pan African Medical Journal. 2020;36.
- Yoo YH, Lee SJ, Jeong SW. Effects of quadriceps angle on patellofemoral contact pressure. Journal of Veterinary Science. 2020 Sep;21(5).
- Evans, A. M., K. Rome and L. Peet (2012). “The foot posture index, ankle lunge test, Beighton scale and the lower limb assessment score in healthy children: a reliability study.” Journal of foot and ankle research 5(1): 1.
- Mohanty NR, Tiwari A, Koley S. Bilateral correlation of Q-angle with selected lower extremity biomechanical alignment variables in state level female basket-ball players. European Journal of Physical Education and Sport Science. 2019 Mar 22.
- Khasawneh RR, Allouh MZ, Abu-El-Rub E. Measurement of the quadriceps (Q) angle with respect to various body parameters in young Arab population. PloS one. 2019 Jun 13;14(6):e0218387.
- Bhalara A, Talsaniya D, Nikita GN. Q angle in children population aged between 7 to 12 years. Int. J. Health Sci. Res. 2013;3:57-64.
- Bangash AS, Hanafi MZ, Idrees R, Zehra N. Risk factors and types of cerebral palsy. JPMA. The Journal of the Pakistan Medical Association. 2014 Jan 1;64(1):103-7.
- Nguyen, A.-D., M. C. Boling, B. Levine, S. J. Shultz, A. Nguyen, M. Boling, B. Levine and S. Shultz (2010). “Relationships Between Lower Extremity Alignment and the Quadriceps Angle.” Journal of Orthopaedic & Sports Physical 40(3): A33.
- Tveter AT, Holm I. Influence of thigh muscle strength and balance on hop length in one-legged hopping in children aged 7–12 years. Gait & posture. 2010 Jun 1;32(2):259-62.
- Özden F. Letter to the editor “A reliable Q angle measurement using a standardized protocol”. The Knee. 2020 Dec 1;27(6):2021-2.
- France, L. and C. Nester (2001). “Effect of errors in the identification of anatomical landmarks on the accuracy of Q angle values.” Clinical Biomechanics 16(8): 710-713.
- Bayraktar,B., Yucesir, I., Ozturk, A., Cakmak, A. K.,Taskara, N.,Kale, A., Demiryurek, D., B ayramoglu, A.& Camlica,H.2004.Change of quadriceps angle values with age and activity. Saudi medical journel, 25,756-760.
- Çankaya T, Dursun Ö, Davazlı B, Toprak H, Çankaya H, Alkan B. Assessment of quadriceps angle in children aged between 2 and 8 years. Turkish Archives of Pediatrics/Türk Pediatri Arşivi. 2020;55(2):124.
- Jimshad, T., S. Mainali, K. Swethankh and A. T. John (2016). “Does Q angle change in spastic diplegia children?” Indian Journal of Cerebral Palsy 2(2): 85.
- Wu CC, Yeow KM, Yeow YJ. Imaging Approaches for Accurate Determination of the Quadriceps Angle. Orthopaedic surgery. 2020 Aug;12(4):1270-6.
- Choudhary R, Malik M, Aslam A, Khurana D, Chauhan S. Effect of various parameters on Quadriceps angle in adult Indian population. Journal of clinical orthopaedics and trauma. 2019 Jan 1;10(1):149-54.
- Camathias C, Rutz E, Götze M, Brunner R, Vavken P, Gaston MS. Poor outcome at 7.5 years after Stanisavljevic quadriceps transposition for patello-femoral instability. Archives of orthopaedic and trauma surgery. 2014 Apr 1;134(4):473-8.
- Wu CC, Yeow KM, Yeow YJ. Varied influence of the femoral or tibial component on quadriceps angles: Verified by imaging studies. Acta orthopaedica et traumatologica turcica. 2019 Jul 1;53(4):287-91.
- Maine ST, O’Gorman P, Barzan M, Stockton CA, Lloyd D, Carty CP. Rotational Malalignment of the Knee Extensor Mechanism: Defining Rotation of the Quadriceps and Its Role in the Spectrum of Patellofemoral Joint Instability. JBJS Open Access. 2019 Oct;4(4).
- Denızoglu Kulli H, Yeldan I, Yildirim NU. Influence of quadriceps angle on static and dynamic balance in young adults. Journal of back and musculoskeletal rehabilitation. 2019 Jan 1;32(6):857-62.
- Çankaya T, Dursun Ö, Davazlı B, Toprak H, Çankaya H, Alkan B. Assessment of quadriceps angle in children aged between 2 and 8 years. Turkish Archives of Pediatrics/Türk Pediatri Arşivi. 2020;55(2):124.
- Hespanhol Junior LC, De Carvalho AC, Costa LO, Lopes AD. Lower limb alignment characteristics are not associated with running injuries in runners: Prospective cohort study. European journal of sport science. 2016 Nov 16;16(8):1137-4.
The Ziauddin University is on the list of I4OA (https://i4oa.org/) & I4OC (https://i4oc.org/).
![]() This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY 4.0). https://creativecommons.org/licenses/by/4.0/
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY 4.0). https://creativecommons.org/licenses/by/4.0/
Conflict of Interest: The author (s) have no conflict.
[i] Lecturer, Physical Therapy Department, Lahore Medical and Dental College, Lahore, Pakistan.
ORCID ID: 0000-0003-2308-6751
[ii] Assistant Professor, Physical Therapy Department, Lahore Medical and Dental College, Lahore, Pakistan.
ORCID ID: 0000-0003-2099-632X
[iii] Senior Lecturer, Physical Therapy Department, Riphah International University, Lahore, Pakistan.
ORCID ID: 0000-0002-3938-1520
[iv] Physical Therapist, Physical Therapy Department, Mobility Quest Center, Lahore, Pakistan.
ORCID ID: 0000-0002-6552-4505