
ABSTRACT
BACKGROUND AND AIM: Adhesive capsulitis characterizes progressive increasing pain followed by progressive decreasing ranges of motion at shoulder joint. The objective was to find out the comparison between the effects of Thera-band, co-contraction and isometric exercises in chronic frozen shoulder patients in improving pain, range of motion and function.
METHODOLOGY: Randomized clinical trial conducted at DHQ Hospital, Sheikhupura. 36 patients with age ranged 30-70 years, diagnosed with chronic idiopathic frozen shoulder with limited shoulder ranges were randomly allocated to three groups, Group A,B,C performed Thera-band, co-contraction and isometric exercises respectively. Assessment was done at baseline and after 6-week post-treatment at Numeric Pain Rating Scale, Goniometry for all ranges and Shoulder Pain and Disability Index. SPSS version 25 was used to analyze the results.
RESULTS: One-way ANOVA with multiple comparisons showed that at 6th week, pain was decreased in Group B and C as compared to Group A (p <0.05), however, there was no significant difference between Group B and C. Group A was significantly better in improving ranges as compared to group B and C.
CONCLUSION: The study concluded that co-contraction and isometric exercises were more effective in reducing pain while the Thera-band exercises showed a significant improvement in ranges.
KEY WORDS: Thera-band, Co-contraction, Isometrics, Frozen shoulder, Idiopathic, Adhesive capsulitis
Ayesha Zakir
Faculty of Rehabilitation and Allied Health Sciences, Riphah International University Islamabad, Lahore Campus, Pakistan
ORCID ID: 0000-0002-8822-5751
Mehwish Ikram
Faculty of Rehabilitation and Allied Health Sciences, Riphah International University Islamabad, Lahore Campus, Pakistan
ORCID ID: 0000-0001-7382-0243
Syed Shakil Ur Rehman
Faculty of Rehabilitation and Allied Health Sciences, Riphah International University Islamabad, Lahore Campus, Pakistan
ORCID ID: 0000-0002-6682-9896
[Zakir A, Ikram M, Rehman SSU. Comparison of Thera-Band, Co-Contraction and Isometric Exercises in Patients with Chronic Frozen Shoulder
Pak.j.rehabil. 2022; 11(1):145-154]
DOI: 10.36283/pjr.zu.11.1/018
INTRODUCTION
Another term used for frozen shoulder is adhesive capsulitis which also defined as the condition characterized by stiffness and pain. It restricts both active and passive movement of glenohumeral joint1. Intrinsic shoulder disorder is not present at this stage. Dull aching pain is experienced in the outer area of shoulder and often pain occurs in upper arm. There are various other conditions such as bursitis, arthritis and rotator cuff tear which play role in restricting the joint motion of glenohumeral joint2. Post breast cancer surgery there is high risk of development of frozen shoulder due to dissection of neck and axillary nodes in combination with radiotherapy and surgery3. After 3 months of onset of symptoms pain gradually increases which further can lead to restrict upper limb functions4. Adhesive capsulitis patients experience severe pain which worsens at night along with stiffness. In this condition passive or active external rotation is fully or partially restricted it mostly affects women. There might be restrictions of scapulothoracic and physiologic glenohumeral movement due to post traumatic changes which results in stiffness of glenohumeral joint. Causes for post traumatic shoulder stiffness can be categorized in to 3 main groups. First in which extra articular adhesions such as hematomas, burn and cervical spine injuries impair movement of the joint and gliding structures. Secondly, direct injuries to intra articular structures from fractures or tendon ruptures may also restrict the joint. Thirdly, secondary fibrosis of capsular structures post trauma or scaring of capsule may be one of the major reasons5. Plan of care is given to the patient which comprise of some essential components such as patient education is first and foremost essential among all, treatment with manual therapy and stretching exercise following resistance training, neuromuscular reeducation and functional training in the end6. As shoulder external and internal rotators are humeral head depressors, in order to strengthen them resisted training using resistive elastic bands or free weights considering deltoid muscle in relaxed position by placing towel between body and arm without dropping it by the end of the exercise7. In comparison to other intervention muscle energy technique is an effective method for functional improvement8. Change in cortical motor representations is due to motor trainings with in few days. These changes relates to neuroplasticity. When subject is given task specific training to achieve targeted goal there is co contraction of skeletal muscles and there is interplay between learning, memory, emotion and cognitive function9. Prevalence rate of adhesive capsulitis is 2–5% along with significant change in lifestyle and increasing co morbidities but it is idiopathic yet10. It is more common in women 17% of patients had bilateral frozen shoulder11. There are three stages of frozen shoulder. Stage 1 is freezing or painful stage. This stage lasts for 10 to 36 weeks. Patient complains onset of pain in shoulder which gradually worsens at night and with performing activities of daily living furthermore pain radiates toward arm in a downward direction additionally, there is increased stiffness and glenohumeral capsule volume is reduced at the end of this stage. Stage 2 refers to a stiffening phase which lasts for 4 to 12 months which restricts motion in all planes. Daily life activities are totally compromised and restricted during this phase. Patient complains of sharp acute discomfort which is due to the tight capsule. Night pain is the one of common complains in frozen shoulder. Stage 3 is also known as thawing or resolution stage which lasts for 5 to 26 months. There is gradual recovery of range of motion12. Many studies revealed that strengthening exercise program in combination with transcutaneous electrical nerve stimulator (TENS) and joint mobilization results inimprovement of pain and increased range of motion (ROM) in adhesive capsulitis patients13.
Main initial treatment purpose is to increase the end range of joint motion by exerting force passively. Heat should be given prior to treatment it helps to relax the joint and muscles and make treatment more effective. Stretching of external and internal rotators is imperative and should be emphasized. Patient education is very essential component. Towel can be used to increase external and internal rotation14. In many researches it was revealed that during abduction middle aged individuals co contract and which in return during abduction depress humerus will ensure passage of subacromial tissues underneath acromion, in contrary to young individuals there is higher degree of adductor co contraction during abduction. This indicates that to preserve pain free shoulder function there should be alterations in activation pattern during aging15. Scapular retraction exercise contributes as a strengthening for scapular muscles as it gently stretch chest muscles. Isometrics shoulder external rotation can be used for flexion or abduction with care as aggressive regimens can contributes in aggravating capsular synovitis and can cause pain. In last thawing stage there is gradual return of range of motion it is difficult to regain normal range of motion and strength. Hence, strengthening exercises are essential as shoulder is weakened with a little movement after few months. In comparison with frozen state in this stage patient is able to perform mobility exercise and static stretches. There are various forms of strengthening regimen programs which progress from isometric or static contractions using a resistance or therabands leading to free weights or weight machines. Posture correction exercises, rotator cuff exercises or exercise for deltoid and chest muscles can be added in the treatment plan.[16] Strengthening exercise of rotator cuff muscles can aid in aligning, improving shoulder function and decreasing pain. There could be other interventions that can be used to restore shoulder function from adhesive capsulitis which indulge NSAIDS, corticosteroid injections and surgery17. Physiotherapy management protocol involves wide variety of treatments which caters electrotherapy, manual therapy including active and passive exercises. The application of ultrasound therapy as a treatment approach has a positive effect on pain severity, function and range of motion in frozen shoulder cases. Also it would be hypothesized that, Shock wave as a line of treatment have a significant result on pain severity, function and ROM in frozen shoulder cases18. The main goal is to improve the range of motion and return patient to the normal routine restoring function and strength of weakened muscles to optimum level19. Pai cone technique is an effective regimen to address restrictions in external and internal rotation range of motions. Strengthening of the scapular muscles play role in stabilizing glenohumeral mechanics20. A recent study concluded that there is significant reduction in pain and improvement in the joint range of motion with active release technique in adhesive capsulitis patients21.
The purpose of this study was to find out the comparison of Thera-band, co-contraction and isometric exercises on shoulder pain, range of motion and function in frozen shoulder patients. It will be helpful for the clinicians and physiotherapists to apply a better treatment on frozen shoulder patients according to their problems.
METHODOLOGY
The study was carried out at DHQ hospital Sheikhupura, physiotherapy department. The study was completed from 6 months after the approval of scientific committee; Reference/RCRS/20/1021.
ClinicalTrials.gov ID clinically registered study: NCT04603768. Sample size was 36 calculated by using online epi tools sample size calculator. Screening was completed as per inclusion criteria and participants were assigned into groups by lottery method. Convenience sampling technique was used. Patients included should have idiopathic frozen shoulder of 6 months chronicity, AROM/PROM less than or equal to 90 degrees, age ranging from 30 to 70 years. Patient’s affected shoulder should not have abduction more than 90 degrees and external rotation decreased 50%. Patients with any history of cervical or thoracic problem, intra-articular injected in glenohumeral joint, trauma, diabetes, compete rotator cuff tear were excluded out of the study. Three outcome measure tools were used. Numeric Pain Rating Scale (NPRS) for pain assessment, if scoring less than 3 were not included, goniometer for ranges (Included 50% less than normal ranges) and shoulder pain and disability index (SPADI) for shoulder function, if scoring less than 50 are not included. Once consent was taken from each participant in the form of agreement, participants were allocated to two groups, group A and group B by lottery method. Inclusion and exclusion listed were determined. Informed consent which was in written form was taken from each participant after collecting data was analyzed at DHQ Hospital Sheikhupura by using SPSS 25. Three study groups, group A, B and C received Thera-band, co contraction and isometric exercises respectively. Patients were recruited in the study by lottery method. Firstly, thorough case history, physical examination and regional assessment were done and basic treatment was given to the allocated groups including mobilizations.
RESULTS
Pre and post assessments for pain were done with Numeric Pain Rating Scale, goniometer was used for shoulder range of motions and Shoulder Pain and Disability Index (SPADI) was used for the assessment of function. Group A performed Thera-band exercises for six weeks. Low resistance Thera-band was used in first 2 weeks. It was gradually progressed by high resistance Thera-band. The exercise with was performed for the strengthening of shoulder flexors ,extensors , internal and external rotators respectively another pattern of exercises including shoulder abduction ,empty can and rowing exercises of 3 sets with 8-10 rep holding for 3 sec was carried out. An essential component is to consider an accurate position of shoulder and upright posture furthermore, another group performed co contraction exercise in which subject is in upright position and contract the agonist muscle and antagonist muscle simultaneously with 5 and 15 seconds duration of sustained self-arm bracing, 3 sets of 6-8 reps. Affected shoulder joint was immobile. Another targeted group C performed isometric exercise for 6 weeks, which included isometric shoulder flexion, extension, abduction, external rotation and internal rotation with 8-10 reps with 5 sec hold and 2 sets. Repeated measure ANOVA was performed within each three groups to determine difference of pain levels among each level of measurements i.e. between, before and post treatment to 3rd week to 6th week. P value was found to be less than 0.05 between all comparisons. In all three groups A, B and C demonstrating significant decrease in pain at all post-treatment measurements. Repeated ANOVA performed to determine with-in group difference of shoulder range of flexion, abduction, extension, internal and external rotation and showed significant increase in range at all post-treatment measurements in all three groups among all three level of measurements in all three groups. between and before treatment to 3rd to 6th week. P-value found to be less than 0.05. One-way ANOVA was performed to determine difference in shoulder flexion range among three group A, B and C. There was no significant difference shown at pre-treatment level, P value was more than 0.05 in flexion range among all three groups. Post Hoc test was applied for multiple comparisons and demonstrated similar flexion before treatment in all groups while at 6th week pain level was significantly decreased in Group B and C as compared to Group A. P value was less than 0.05, however there was no significant difference between Group B and C, p value more than 0.05.
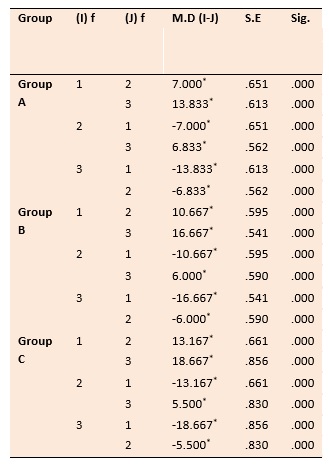
Table 1 within group pairwise comparison
Table 1 demonstrates repeated measure ANOVA was performed to determine within group difference of pain section of SPADI among three levels of measurements i.e. between before treatment to 3rd week and to 6th week. P value found to be less than 0.05 between all comparisons in all three groups A, B and C showing a significant improvement in SPADI Pain Score at all post-treatment measurements in all three groups.
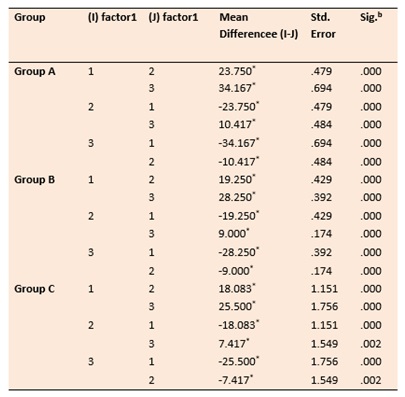
Table 2 Within Group pairwise comparison for SPADI Disability score
Table 2 represents repeated measure ANOVA was performed to determine within group difference of disability section of SPADI among three levels of measurements i.e. between before treatment to 3rd week and to 6th week. P value found to be less than 0.05 between all comparisons in all three groups A, B and C showing a significant improvement in SPADI Disability Score at all post-treatment measurements in all three groups.
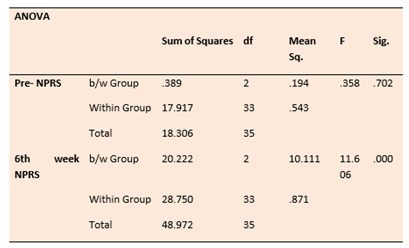
Table 3 Between Group comparison of pain by ANOVA
Table 3 shows One-way ANOVA was performed to determine difference in level of pain among three groups A, B and C. It was shown that at pre-treatment level there was no significant difference, p value more than 0.05 in pain level, however at 6th week there was significant difference, p value less than 0.05 in pain level among three groups.
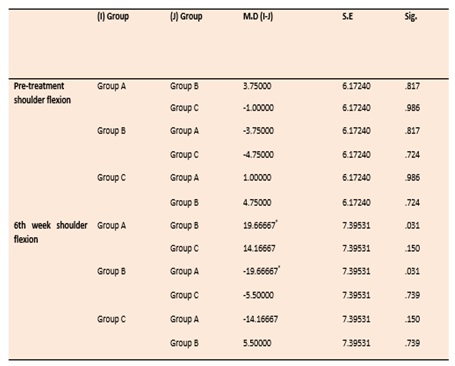
Table 4 Post HOC multiple comparison of pain
Table 4 shows multiple comparisons measured by Post-Hoc tests. It showed that before treatment shoulder flexion was similar in all groups, p value more than 0.05, while at 6th week, shoulder flexion significantly improved in Group A in association with Group B and Group C, with p<0.05, however, there was no significant difference between Group B and C, p>0.05.
DISCUSSION
Glenohumeral joint represents a dynamic relationship of the force applied by the muscle ligaments and bony articulations. There are static and dynamic stabilizers which contribute in range of motion at extreme level of any joint additionally, maintains hand and elbow in position. Elastic bands used in resistance training is a well-defined tool in adhesive capsulitis patients unlike other methods used traditionally, as it is elastic in nature and has tensile properties of latex or other elastic polymers as a form of resistance. There are levels of resistance according to the stretch which are termed as low medium and hard according to the patient’s condition or requirement.[14] According to the study conducted by Hughes and Mcbride revealed that using thera band in strengthening program is a gold standard approach in treatment of adhesive capsulitis of shoulder. In deceleration pattern theraband is an effective method in boosting the eccentric strength at slow speed. Harishkumar et al study revealed that Thera-band was effective in all aspects including; pain, range of motion and function22.According to current study conducted on 36 targeted individuals revealed Theraband to be an effective method in improving range of motion in adhesive capsulitis.
Nakandala N et al in 2020 found that isometrics, continuous passive motion, PNF stretches, ultrasonic therapy combined with other conventional methods of physical therapy showed moderate evidence in terms of improvement in range of motion and reducing pain at 2 and 3 stage of adhesive capsulitis.[14] There is high degree of muscular contraction in combined contraction of muscles having eccentric and concentric force and PNF techniques in comparison of exercising with dumbbells. Agonist and antagonist muscle act in opposite directions which react to voluntary and involuntary stimulus in concentric or eccentric manner which directly acts as dynamic joint stabilization.23
Another study conducted by Kotagiri S et al in 2019 and concluded muscle energy technique to be more effective way in treating frozen shoulder. 60 individuals participated in the study divided in to two groups. Group A and group B 30 each assigned randomly respectively. Pre -test measurement were done by VAS, SPADI and goniometer.24
One more study conducted by Jongchan Jung et al on Effects of combining both mobilization and hold-relax technique on the function of post-surgical patients with shoulder adhesive capsulitis. Findings concluded that hold relax in combination with movement with mobilization improve range of motion and shoulder function and more effective way post-surgery adhesive capsulitis.25 A recent study in 2021 revealed that electrically eccentric contractions combining with voluntary concentric contractions is an effective way of improving external rotator muscle strength.[26] There are different exercises with multiple combinations, proved as effective in the treatment of frozen shoulder. In this study Thera-band was effective in improving ranges of motion while other treatments were effective in pain and function.
CONCLUSION
The study concluded that co-contraction and isometric exercises were significantly more effective as compared to Thera-band exercises in reducing pain in patients of frozen shoulder while Thera-band exercises were significantly more effective as compared to both co-contraction and isometrics in improving shoulder ranges in frozen shoulder.
LIMITATIONS
Population from a specific area were involved in the study. Further research can be conducted on higher levels including different areas and more population.
AUTHORS’ CONTRIBUTION
AZ collected the data, MI; data analysis and interpretation and SSR supervised the project.
REFERENCES
- Hammad SM, Arsh A, Iqbal M, Khan W, Shah A. Comparing the effectiveness of kaltenborn mobilization with thermotherapy versus kaltenborn mobilization alone in patients with frozen shoulder [adhesive capsulitis]: A randomized control trial. J Pak Med Assoc. 2019;69:1421-4.
- GoPinath Y, SeenivaSan SK, Veeraraghavan SNC, Viswanathan R, Govindaraj MK. Effect of Gong’s Mobilisation versus Muscle Energy Technique on Pain and Functional Ability of Shoulder in Phase II Adhesive Capsulitis. J Clin Diagn Res 2018;12(9).
- Yang S, Park DH, Ahn SH, Kim J, Lee JW, Han JY, Kim DK, Jeon JY, Choi KH, Kim W. Prevalence and risk factors of adhesive capsulitis of the shoulder after breast cancer treatment. Support Care Cancer 2017;25(4):1317-22.
- Sukumar Shanmugam D, Mathias L, Manickaraj N, Kumar KD, Kandakurti PK, Shanmugam S, Mathias L, Nagarajan Manickaraj N, Kumar KUD, Kandakurti PK, Dorairaj SK, Ramprasad Muthukrishnan R, Intramuscular Electrical Stimulation Combined with Therapeutic Exercises in Patients with Shoulder Adhesive Capsulitis: A Randomised Controlled Trial. Int J Surg Protoc 2021;25(1):71.
- Itoi E, Arce G, Bain GI, Diercks RL, Guttmann D, Imhoff AB, et al. Shoulder stiffness: current concepts and concerns. Arthroscopy: J Arthrosc Relat Surg 2016;32(7):1402-14.
- Wong CK, Strang BL, Schram GA, Mercer EA, Kesting RS, Deo KS. A pragmatic regional interdependence approach to primary frozen shoulder: a retrospective case series. J Man Manip Ther 2018;26(2):109-18.
- Duzgun I, Eraslan LS, Yildiz TI, Demirci S. Shoulder Rehabilitation. The Shoulder: The Shoulder. Orthopaedic Study Guide Series. Springer, Cham; 2017. p. 215-55.
- Mertens MG, Meert L, Struyf F, Schwank A, Meeus M. Exercise therapy is effective for improvement in range of motion, function and pain in patients with frozen shoulder: a systematic review and meta-analysis. Arch Phys Med Rehabil. In press,
- Sawant AR, Shinde S. Effect of Task-Specific Training in Frozen Shoulder.
- Cho C-H, Bae K-C, Kim D-H. Treatment strategy for frozen shoulder. Clin Orthop Surg 2019;11(3):249-57.
- Anjum R, Aggarwal J, Gautam R, Pathak S, Sharma A. Evaluating the outcome of two different regimes in adhesive capsulitis: a prospective clinical study. Med Princ Pract 2020;29(3):225-30.
- Patil S. Chapter-6 Frozen Shoulder: A Physiotherapeutic Evidence Based Practice. Advances in Academic Research and Development. Dehli, India, 2020:75.
- Rawat P, Eapen C, Seema KP. Effect of rotator cuff strengthening as an adjunct to standard care in subjects with adhesive capsulitis: A randomized controlled trial. J Hand Ther. 2017;30(3):235-41. e8.
- Nakandala N, Nanayakkara S, Wadugodapitiya S, Gawarammana I. The efficacy of physiotherapy interventions in the treatment of adhesive capsulitis: A systematic review. J Back Musculoskelet Rehabil 2020(Preprint):1-11.
- Overbeek CL, Kolk A, de Groot JH, de Witte PB, Gademan MG, Nelissen RG, et al. Middle-aged adults cocontract with arm ADductors during arm ABduction, while young adults do not. Adaptations to preserve pain-free function? J Electromyogr Kinesio 2019;49:102351.
- Chan HBY, Pua PY, How CH. Physical therapy in the management of frozen shoulder. Singapore Med J 2017;58(12):685.
- Brenner H. A Case Report: Adhesive Capsulitis and Physical Therapy Intervention. 2019.
- Alarab A, Shameh R, Shaheen H, Ahmad MS. Shock wave therapy and ultrasound therapy plus excercises for frozen shoulder joint clients. Adv Nursing Patient Care Int J 2018;1(2):1-7.
- Anthonia EU, Ozoemene EV, Paulinus IC, Anthoninus EO, Eneje EL, Nkemdilim OC, et al. Response Of Frozen Shoulder To Six Weeks Of Short Wave Diathermy And Supervised Active Exercises: A Case Report.
- Adamov E, Ilizarov S. Adhesive Capsulitis. Musculoskeletal Sports and Spine Disorders: Springer; 2017. p. 59-64.
- Rajalaxmi V, Vasanthi S, Sathya S, Kirupa K, Mary SD, Aravind V, et al. Efficacy of Dynamic VS Closed Kinematic Exercise Combined with Stretching in Adhesive Capsulitis-a double blinded randomized controlled trial. Bangladesh J Med Sci 2021;20(2):368-73.
- Harishkumar S, Kiruthika S, Arunachalam R, Kumerasan A. Motion in patients with adhesive capsulitis.Int J Pharma Bio Sci 2017;8(4):214-227.
- Comel JC, Nery RM, Garcia EL, da Silva Bueno C, de Oliveira Silveira E, Zarantonello MM, et al. A comparative study on the recruitment of shoulder stabilizing muscles and types of exercises. J Exerc Rehabil 2018;14(2):219.
- Kotagiri S, Mathur N, Balakavi G, Songa AK. The Effectiveness of Muscle Energy Technique and Mobilization to Improve the Shoulder Range of Motion in Frozen Shoulder. 2019.
- Jung J, Chung Y. Effects of combining both mobilization and hold-relax technique on the function of post-surgical patients with shoulder adhesive capsulitis. Phys Ther Rehabil Sci 2020;9(2):90-7.
- Hara K, Matsuse H, Hashida R, Iwanaga S, Bekki M, Hara M, et al. The effect of rotator cuff physical exercise combined with electrically stimulated antagonist on shoulder rotator cuff strength. J Orthop Sci, in press, 2021.