
ABSTRACT
BACKGROUND AND AIM
Lateral epicondylitis or tennis elbow is a pain pattern most commonly seen in tennis player due to forceful repetitive movements in a wrong way. So, the Objective was to determine the comparison of mobilization with movement and soft tissue mobilization on pain, grip strength and functional activity in patients with tennis elbow.
METHODOLOGY: In this Randomized Controlled Trial, Non probability sampling technique was used. Thirty tennis players having lateral epicondylitis pain were included in the study. Two interventions were used i.e. Mobilization with movement and soft tissue mobilization. Pain, Muscle power and function activity were 3 outcome measure in both groups.
RESULTS: In both groups the mean age of the participants was 24.30 ± SD 3.01. There was a significant Mean difference in the pain scores for MWM (5.34) and Soft Tissue Mobilization (3.74) after treatment. P value is significant for both group but there was greater difference with group MWM
CONCLUSIONS: The present study concluded that Mobilization with movement has greater effect than the Soft Tissue Mobilization in relieving pain and improving Hand grip strength and functional activity in patients with tennis elbow.
Key words: Movement, soft tissue, pain, grip, hand strength functional status, tennis elbow
Sidra Shafique
Senior Lecturer
RCRS
Riphah International University, Lahore.
ORCID ID: 0000-0003-4228-1691
Hafiza Neelam Muneeb
Senior Lecturer
RCRS
Riphah International University, Lahore.
ORCID ID: 0000-0002-3221-7445
Naseem Abbas
Student
RCRS
Riphah International University, Lahore.
ORCID ID: 0000-0002-3472-9081
Iqra abdul ghafoor
Lecturer
RCRS
Riphah International University, Lahore. Pakistan
ORCID ID: 0000-0003-3926-2916
[Shafique S, Muneeb HN, Abbas N, et al. Comparison of Mobilization with Movement and Soft Tissue Mobilization on Pain Severity, Hand Grip Strength and Functional Activity in Tennis Elbow Patient
Pak.j.rehabil. 2022; 11(1):72-79]
DOI: 10.36283/pjr.zu.11.1/010
INTRODUCTION
Lateral epicondylitis injury affecting the origin of tendons of main wrist extensors muscle1. Lateral epicondylitis was most commonly seen in tennis player and it as seen less commonly in different professionals like electricians or carpenters and also in plumbers2. Nearly 45% of professional tennis players are mostly affected with Lateral epicondylitis due to forceful repetitive movements like pronation and supination of forearm movements in a wrong way3.
Tennis elbow was expected to affect almost 1–3% of adult per year and mostly occur in the dominant side arm4. It is commonly considered as overuse injury which involve repeated movements like wrist extension mostly against resistance, but it can be due to any acute injury1. Almost 50% of all tennis player may develop sign and symptoms due to different factors during the game including bad posture especially poor swing, technique and by using heavier racquets5. Tennis elbow exhibits as an inflammation over the main lateral epicondyles of arm bone i.e. humerus, and severe pain due to any type of such activity which involve some resisted dorsiflexion at wrist joint6 Its main symptoms can remain almost for 6 months to almost 2 years, but symptoms may be resolve itself or own its own within a year . The Tennis elbow pain mostly involve and affects a person s dominant side / arm, and the its severity may be increase over time and may persist for more than 2 years even in female7 Tennis elbow was expected to affect almost 1–3% of adult per year and mostly occur in the dominant side arm. It is commonly considered as overuse injury which involve repeated movements like wrist extension mostly against resistance, but it can be due to any acute injury8.
A common demonstration and clinically presentation of the disorder may mainly just pain and tenderness at the location of injury i.e. lateral epicondyle at elbow , the radial or lateral head, and over the fascia in between both the origins of mainly extensor muscles that may radiate towards the forearm9. Many people do complaint of weak strength and grip of hand and painful grasp, ultimately resulting in shaking hands during usual activities of daily living for example turning or opening a door handle, picking or lifting something in hand may be just a cup of tea of a glass of water, or holding a briefcase or any weight may create or aggravate pain around the lateral epicondyle. Mobilization with movement is consider an effective management for patients suffering from tennis elbow5.
Evidence said that an extensors fasciotomy, Extracorporeal shock wave therapy, ultrasound therapy, local corticosteroid injections, conservative management like physical therapy, or acupuncture also shown to be an effective therapeutic techniques for long-term relief of pain and improvement in function in patients of tennis elbow . (8)Mobilization with movement is consider an effective management for patients suffering from tennis elbow5.Mobilization with Movement /MWM is combination of manual – therapy techniques as well as exercise and special movement patterns which claim to offer an immediate relief of pain and improvement in the range of motion of that joint also improves the functional activities7.Theoretically, MWM work by repositioning the main positional faults .MWM correct these faults by repositioning the joint and muscular balances and causing it to retract them back normally10.
The rationale of this study was to compare the effects of Mobilization with Movement and Soft Tissue Mobilization in Patients of Tennis Elbow .The main purpose of this research was to check which is more beneficial in reducing pain and improving Hand grip Strength and Functional Activity either Mobilization with Movement or Soft Tissue Mobilization technique.
METHODOLOGY
The study design was Randomized Clinical Trial. Non probability sampling technique was used. The study was conducted at Pakistan sports board Lahore and Hidayat Gillani orthopedics, trauma and rehabilitation center Sahiwal. The study was conducted in between October 2020 to June 30, 2021.Sample size is 30, calculated by Epitool. Tennis players with Age group between 15-30 years with Positive specific tests (cozen test, mills test) were included in this study. Patients having pain intensity >3 on Numerical pain rating scale were included in the study. Tennis player with any history of neurological disorder or other elbow deformity or joint pathology were excluded.
Ethical approval was taken from research and ethics committee of Riphah college of Rehabilitation and Allied Health Sciences with Ref.No. REC/RCR & AHS/21/0420. Data was collected after obtaining informed consent from participants. Patients were divided into 2 groups i.e. Mobilization with Movement (MWM) group and Soft Tissue Mobilization (STM) group randomly by lottery method. In MWM group the participants received intervention 3 session per week for 4 weeks hence total 12 sessions. In soft tissue mobilization (STM) group the participants also received intervention 3 session per week for 4 weeks hence total 12 sessions. Each session lasted 20-30minutes. The session was repeated three times a week for 4 weeks.
Pain, Muscle power and function activity were 3 outcome measure in both groups .Pain assessment was done by 11 Point NPRS, where the end points are extremes of no pain and worst pain. The NPRS is a Reliable and valid pain assessment scale in tennis elbow patients11. Patient-related tennis elbow evaluation (PRTEE) index was used to assess functional status of tennis elbow patients on initial visit and after 4th week. The PRTEE is a valid and reliable instrument for tennis elbow patients12.Manual muscle testing is a reliable tool for assessing muscle strength in tennis elbowpatients13. The data analysis was done by using SPSS version 21.
RESULTS
Out of 30 patients, there were 15 (50%) in each group. Mean age of the participants was 24.30 ± SD 3.01 years, 80% were male and Only 2 out of 30 participants was having left side involved and 26 i.e. 86% was having right side affected with tennis elbow.Normality of data was checked by Shapiro wilk test that showed that data was normally distributed with p value > 0.05. Parametric tests were used to compare both groups at pre-treatment and post treatment level. Independent sample t-test was applied to measure difference between two groups. Paired sample t test was applied to measure difference within each group
Figure 1: Age of the participant’s histogram
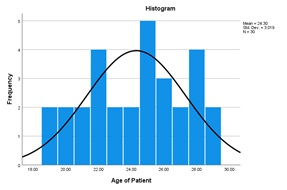
Figure 1 shows that in both groups the mean age of the participants was 24.30 ± SD 3.01 Years.
Figure 2: Gender Of participant pie chart
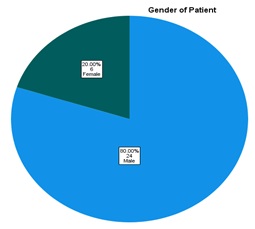
Figure shows that 20 % female and 80% were male.
Figure 3: Side of Injury Pie chart
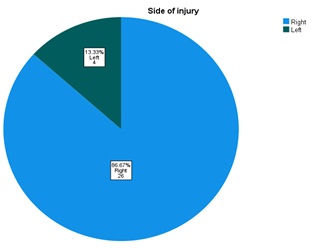
Only 2 out of 30 participants was having left side involved and 26 i.e. 86% was having right side affected with tennis elbow
Table: 1 Pain at baseline and post treatment within group and in between group
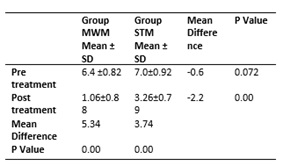
A paired sample t test and an independent samples t-test was conducted to compare the effects of MWM and Soft Tissue Mobilization in in between and within group. There was a significant Mean difference in the pain scores for MWM (5.34) and Soft Tissue Mobilization (3.74) after treatment. P value is significant for both group but there was greater difference with group MWM than group STM.
Table: 2 Grip Strength at baseline and post treatment within group and in between group
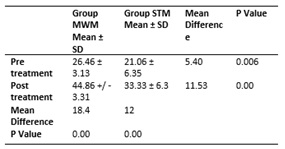
Group MWM pre-treatment values were 26.46 ± 3.13 while Post treatment values were 44.86 +/ – 3.31. Mean Difference was 18.4 and p value < 0.05. While in Group STM pre-treatment values were 21.06 ± 6.35while Post treatment values were 33.33 ± 6.3. Mean Difference was 12and p value < 0.05.There was significant difference after both techniques but there was greater difference with group MWM than group STM.
Table: 3 Specific activities at baseline and post treatment within group and in between group
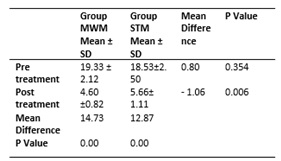
Specific activities are carry a grocery bag, turn a doorknob and key ,lift a full coffee cup to your mouth ,pen a jar ,pull up pants Table show that p value is significant for both groups and within group at pretreatment and post treatment level.
In between 2 groups p value is also significant i.e. p <0.05 and mean difference is greater after treatment session.
Table: 4 usual activities at baseline and post treatment within group and in between group
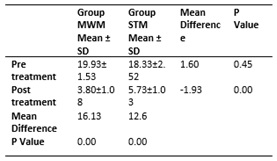
Usual activities included are personal activity(dressing, washing),house hold work (cleaning and maintenance) ,work(your job or everyday work recreational and sporting activities .Group MWM has mean difference of 16.13 as its pre-treatment mean ±SD was 19.93± 1.53 and post treatment mean ±SD was 3.80±1.08. Group Soft Tissue Mobilization has mean difference of 12.6as its pre-treatment mean ±SD was 18.33±2.52 and post treatment mean ±SD was 5.73±1.03 while P value is significant for both groups.
DISCUSSION
The present study was conducted to see the effects of, MWM with STM in patients with lateral epicondylitis . The main results of present study were pain relief, improved grip strength and specific and usual activities. In this study the author include the Age group between 15-30 years. According to literature a study was conducted in which, mean age at which tennis elbow occur is in between 40 to 50 years 14.
In UK 2017, A research was done on orthopedic surgeons and physiotherapists to investigate which techniques are best for tennis elbow results were that approximately 81% recommended that therapeutic exercises as a first-line treatment option .(15)Stasinopoulos D et al. stated that Deep friction massage along with Mill’s manipulation technique is very effective method for treatment of pain associated with tennis elbow.(16) But in current study Mobilization with movement has greater effect than the Soft Tissue Mobilization in relieving pain and improving grip strength and fictional status in patients with tennis elbow.
Brosseau et al. said that DTF massage therapy for the managing the patients of tendinitis and author concluded that massage therapy is one of the main choice for treating patients of tendinitis.(17) Trishna Kakati et al said that that both Mulligan’s technique MWM and elbow orthosis are very effective in pain management and improving the grip strength in patients of tennis elbow directly after treatment. (18, 19) But in current study Mobilization with movement showed best results in relieving pain and improving grip strength and in patients with tennis elbow.
In Current study MWM was very effective to improve functional status in tennis elbow patients while a study done by Karthika Prasad et al in india in 2019, the Myofascial Release was more effective in improving grip strength and functional status in contrast to MWM 20,21.In 2020, JH Lee et al a research findings revealed that taping techniques along with Deep Friction Massage are also an effective approach in tennis elbow for pain reduction , improvement of functions, and grip strength along with muscle activation in lateral epicondylitis22.
In a previous reseach done by , Shamsoddini et al taping techniques was very effective to reduce pain in tennis elbow (23) and same results showed by Vicenzino et al.that diamond shape taping techniques was best pattern than other taping techniques. (24) Previous study done by Nagrale et al. Showed that steroid injections and deep friction massage reduce pain in patients of tennis elbow25.Peterson et al. conducted randomized trial to see the effects of eccentric exercises along with concentric exercises and he found that eccentric exercises showed more improvement of pain and muscle strength. (26)In current study Mobilization with movement has greater effect than the Soft Tissue Mobilization in relieving pain and improving grip strength and fictional status in patients with tennis elbow
CONCLUSION
The present study concluded that Mobilization with movement has more effect than the Soft Tissue Mobilization in relieving pain and improving grip strength and fictional status in patients with tennis elbow.
RECOMMENDATIONS
- Immediate and long term effect must be evaluated
- Sample size should be enhanced
- Study should be done other age group as well
- More studies should be conducted in treating different postural syndrome and musculoskeletal condition independently.
REFERENCES
- Bagade VK, Verma C. Effect of Mulligan Mobilization with Movement (MWM) in the Treatment of Chronic Lateral Epicondylitis: 24 Weeks Follow-up Study. Website: www ijpot com. 2015;9(4):199.
- Abbas S, Riaz R, Khan A, Javed A, Raza s. effects of mulligan and cyriax approach in patients with subacute lateral epicondylitis: soi: 21-2017/re-trjvol03iss02p107. The Rehabilitation Journal. 2019;3(02):107-15.
- Basak T, Pal TK, Saha MB, Agarwal S, Das T. Comparative Efficacy of Wrist Manipulation, Progressive Exercises and Both Treatments in Patients with Tennis Elbow. International Journal of Health Sciences and Research. 2018;8(4):87-94.
- Barrington J, Hage WD. Lateral epicondylitis (tennis elbow): nonoperative, open, or arthroscopic treatment? Current Opinion in Orthopaedics. 2003;14(4):291-5.
- Cutts S, Gangoo S, Modi N, Pasapula C. Tennis elbow: A clinical review article. Journal of orthopaedics. 2020;17:203-7.
- Bisset L, Paungmali A, Vicenzino B, Beller E. A systematic review and meta-analysis of clinical trials on physical interventions for lateral epicondylalgia. British journal of sports medicine. 2005;39(7):411-22.
- Castillo-Lozano R, Casuso-Holgado MJ. Incidence of musculoskeletal sport injuries in a sample of male and female recreational paddle-tennis players. The Journal of sports medicine and physical fitness. 2016;57(6):816-21.
- Yan C, Xiong Y, Chen L, Endo Y, Hu L, Liu M, et al. A comparative study of the efficacy of ultrasonics and extracorporeal shock wave in the treatment of tennis elbow: a meta-analysis of randomized controlled trials. Journal of orthopaedic surgery and research. 2019;14(1):1-12.
- Ahn S-w, Yoo T-g. The effect of soft tissue mobilization using prop on the pain, grip strength, functional activity and proprioception in patients with lateral epicondylitis. The Journal of Korean Academy of Orthopedic Manual Physical Therapy. 2017;23(1):15-22.
- Coombes BK, Connelly L, Bisset L, Vicenzino B. Economic evaluation favours physiotherapy but not corticosteroid injection as a first-line intervention for chronic lateral epicondylalgia: evidence from a randomised clinical trial. British journal of sports medicine. 2016;50(22):1400-5.
- Abhimanyu V, Ritika P, Osama N, Srishti N, Gita H. Lateral epicondylitis: Are we missing out on radial nerve involvement? A cross-sectional study. Journal of Bodywork and Movement Therapies. 2021;27:352-7.
- Shafiee E, MacDermid JC, Walton D, Vincent JI, Grewal R. Psychometric properties and cross-cultural adaptation of the Patient-Rated Tennis Elbow Evaluation (PRTEE); a systematic review and meta-analysis. Disability and Rehabilitation. 2021:1-16.
- Baschung Pfister P, de Bruin ED, Sterkele I, Maurer B, de Bie RA, Knols RH. Manual muscle testing and hand-held dynamometry in people with inflammatory myopathy: An intra-and interrater reliability and validity study. PloS one. 2018;13(3):e0194531.
- Rabago D, Lee KS, Ryan M, Chourasia AO, Sesto ME, Zgierska A, et al. Hypertonic dextrose and morrhuate sodium injections (prolotherapy) for lateral epicondylosis (tennis elbow): Results of a single-blind, pilot-level randomized controlled trial. American journal of physical medicine & rehabilitation/Association of Academic Physiatrists. 2013;92(7):587.
- Fry A, Littlejohns TJ, Sudlow C, Doherty N, Adamska L, Sprosen T, et al. Comparison of sociodemographic and health-related characteristics of UK Biobank participants with those of the general population. American journal of epidemiology. 2017;186(9):1026-34.
- Stasinopoulos D, Papageorgiou SN, Kirsch F, Daratsianos N, Jäger A, Bourauel C. Failure patterns of different bracket systems and their influence on treatment duration: a retrospective cohort study. The Angle Orthodontist. 2018;88(3):338-47.
- Pitsillides A, Stasinopoulos D. The beliefs and attitudes of cypriot physical therapists regarding the use of deep friction massage. Medicina. 2019;55(8):472.
- Lyngdoh AW, Khatonier P, Das J, Lyngdoh S. Bengal Slow Loris, Nycticebus bengalensis.
- Selvan KM, Krishnakumar BM, Ramasamy P, Thinesh T. Diel activity pattern of meso-carnivores in the suburban tropical dry evergreen forest of the Coromandel Coast, India. Journal of Threatened Taxa. 2019;11(8):13960-6.
- Rezkallah SS, Abdullah GA. Comparison between sustained natural apophyseal glides (SNAG’s) and myofascial release techniques combined with exercises in non specific neck pain. Physiotherapy Practice and Research. 2018;39(2):135-45.
- Kaya Mutlu E, Ercin E, Razak Ozdıncler A, Ones N. A comparison of two manual physical therapy approaches and electrotherapy modalities for patients with knee osteoarthritis: A randomized three arm clinical trial. Physiotherapy theory and practice. 2018;34(8):600-12.
- Lee J-H, Oh J-S, Kim M-H. Effect of Deep Friction Massage with Taping Technique on Strength, Pain, Function and Wrist Extensor Muscle Activity in Patient with Tennis Elbow. Journal of Musculoskeletal Science and Technology. 2020;4(2):76-83.
- Sobhani V, Shamsoddini A, Khatibi-Aghda A, Mazloum V, Kia HH, Meybodi ME. Effectiveness of Dry Needling, Manual Therapy, and Kinesio Taping (R) for Patients with Chronic Myofascial Neck Pain: A Single-Blind Clinical Trial. Trauma Monthly. 2017;22(6):8.
- Collins NJ, Barton CJ, Van Middelkoop M, Callaghan MJ, Rathleff MS, Vicenzino BT, et al. 2018 Consensus statement on exercise therapy and physical interventions (orthoses, taping and manual therapy) to treat patellofemoral pain: recommendations from the 5th International Patellofemoral Pain Research Retreat, Gold Coast, Australia, 2017. British journal of sports medicine. 2018;52(18):1170-8.
- Joseph MF, Taft K, Moskwa M, Denegar CR. Deep friction massage to treat tendinopathy: a systematic review of a classic treatment in the face of a new paradigm of understanding. Journal of sport rehabilitation. 2012;21(4):343-53.
- Amsterdam EA, Wenger NK, Brindis RG, Casey DE, Ganiats TG, Holmes DR, et al. 2014 AHA/ACC guideline for the management of patients with non–ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Journal of the American College of Cardiology. 2014;64(24):e139-e228.