
ABSTRACT
BACKGROUND
Pregnancy is the ideal time for positive lifestyle modifications, including consuming more healthy diet and increasing physical activity. Importance of exercise is supported by the increasing evidence for individual health but unfortunately women are not much aware about the benefits and importance of exercises.
OBJECTIVE
To evaluate how much the pregnant patients coming in gynecological OPD of DOW college clinic, Karachi know about gynecological rehabilitation in their pregnancy period. Moreover, the study will analyze the knowledge level of patients regarding rehab importance during pregnancy.
METHODS AND MATERIALS
A cross-sectional study design will be conducted to carry out the study. 158 participants were selected through convenient sampling technique from DOW university hospital, Karachi and the data will be collected by a self-structured questionnaire.
DATA ANALYSIS
SPSS version 22 will be used for the purpose of statistical analysis. Mean and standard deviation were calculated for all quantitative variables like age. Frequency and percentages were calculated for categorical variables like residence, educational status.
RESULTS
On the basis of gravida, patients of primi-gravida were 38(24.1%) and para-gravida 120(75.9%). 63.3% patients were unaware about physiotherapy services during pregnancy, 90.5% of patients didn’t know about kegal exercises, 56.3% of patients were unaware that weak pelvic floor muscles (PFMs) can cause urinary incontinence.
CONCLUSION
A majority of pregnant patients were participated and demonstrated in inadequate knowledge about gynecological rehabilitation in pregnancy. However, the patients who had awareness of gynecological rehabilitation were in minority. Information about the exercises during pregnancy considerably influences the approach towards exercises in pregnancy.
KEYWORDS
Gynecological Rehabilitation; Pregnancy; Exercises; Pelvic floor; Urinary Incontinence; Primi – Gravida; Pregnancy Rehabilitation
Tooba Hassan
Student of Liaquat National Hospital Karachi
ORCID ID: 0000-0002-6961-9050
Fouzia Arif
Student of Istanbul Aydin University, Turkey
ORCID ID: 0000-0002-5625-1867
Saira Khalid
Student of Mphil in tabba heart institute
ORCID ID: 0000-0002-8398-1988
Muhammad Faisal
Student of Liaquat National Hospital Karachi
ORCID ID: 0000-0003-4618-4821
[Hassan T, Arif F, Khalid S, et al. Awareness Of Gynecological Rehabilitation In Pregnancy, A Survey Among Pregnant Patients In Gynae OPD Dow University Hospital, Karachi
Pak.j.rehabil. 2022; 11(1):88-98]
DOI: 10.36283/pjr.zu.11.1/012
INTRODUCTION
Pregnancy is also well-known as gestation, the moment of development of single or more offspring’s inside the uterus of a woman. A numerous pregnancy is the involvement of more than one offspring, such as with clones. Sexual intercourse and aided sexual technology can cause pregnancy. Labor normally occurs in the order of 40 weeks from the last menstrual period1.
Pregnancy is normally distributed into 3 trimesters. The 1st trimester is from first week through 12 weeks also including conception (at what time the sperm fertilizes the egg). The egg which is fertilized then moves to the fallopian tube and get attached inside the uterus, where the formation of the Embryo and placenta begins. During the first trimester, the miscarriage (natural death of embryo or fetus) possibility is maximum. The second trimester is from week 13 through 28. The movement of the fetus may be felt around the middle of the second trimester. At about 28 weeks, greater than 90% offspring be able to stay alive outside the uterus by means of the provision of high-class medical care. The 3rd trimester is from week 29 to40 in which delivery of baby occurs1.
During pregnancy the organ placenta forms and grows within the baby in the uterus. Umbilical cord connects the baby with the placenta and is the source of transference of important nutrients, blood and oxygen from mother to baby2.
A tube that attaches the fetus to the placenta is known as umbilical cord. The nutrients, blood and oxygen is delivered to the baby from mother through umbilical cord, and it eliminates carbon dioxide and waste products.2
The word uterus is well-known as the womb. The development and growth of fetus occurs within the uterus. It is joined with the fallopian tubes, through which female’s eggs are released and to the cervix through which baby is delivered2.
An amniotic sac is the “bag of waters” which soon after conception is formed within the uterus. The fetus is enclosed and is occupied with the amniotic fluid in uterus, this fluid provides cushioning to the fetus and works in the regulation of its temperature2.
The lower portion of the uterus is the cervix. Vaginal opening is lead through the cervix. During labor the process of affectation occurs in cervix, means it becomes dilated2.
At 14th day in normal menstrual cycle ovulation takes place and in less than 24 hours fertilization occurs. Estrogen and progesterone secreted by corpus luteum comes in the control of HCG secreted by the blastocyst in early pregnancy. pregnancy is controlled by progesterone and abortion the result of stoppage of it. Similarly, pregnancy progress with the increase production of estrogen. Another hormone relaxin, cause relieve in the overstretch ligaments. Fetus produce estrogen while placenta is responsible for the secretion of progesterone after 8 weeks of pregnancy. VO2 increase by 4% with the increase of renal, cardiac and respiratory function. In full term pregnancy blood volume increase by 50%, 30-60% plasma volume, total red cells by 20% and cardiac output by 40%. Blood volume is increase due to increase in cardiovascular system capacitance. Left ventricle size increases which cause change in stroke volume. Placenta is 90% supplied by the whole uterine blood flow. Pregnant ladies are over hydrated due to decrease in plasma osmolality3.
Gynecological rehabilitation is a therapy to regain or improve gynecological function that has been lost or diminished following the complications and diseases affecting the reproductive system specific to girls and women4.
Pregnancy is the best and ideal time positive lifestyle modifications, including consuming a more healthy diet and increasing physical activity5.
Physiotherapy plays an important role in pregnancy, both in antenatal and postnatal periods. It is not related with any risk factors to the baby. It can also lead to useful, long-lasting effects for women. Physical exercises are important for pregnant females as they sustain good physical fitness and benefit to overcome pregnancy-related problems. Women who experienced antenatal exercises with supervised training presented quicker deliveries for the period of labour. Furthermore, it is showed that higher physical exercises in multiparous females throughout late pregnancy positively affect the period of the 2nd stage of labor. In addition there is evidence that shows women who experienced antenatal exercises have less chance of backache, caesarean section and urinary incontinence6.
Ideally, exercise prescription for pregnant females should be based on the findings of clinical trials that have determined the special effects of regular exercise on ease or difficulty of labor and delivery, physical fitness on the consequence and progression of pregnancy3.
Importance of exercise is supported by the increasing evidence for individual health. The risk of diseases can be reduced by being active7. Association of habitual exercise throughout pregnancy with several fetal and maternal advantages includes pre-eclampsia, reduced musculoskeletal complaint, decreased risk of gestational diabetes, enhanced mental health and impaired cardiovascular fitness8.
An important index of fetal health is the fetal movements and breathing activity. The fetuses who breathe actively are considered as healthy fetuses. The reason behind this is that the consumption of oxygen is increased by the activity3.
Traditionally, women in pregnancy have been guided to limit exercise due to concern for mother and fetus’s health, including the risk of overheating, compromised nutrients and oxygen delivery to the fetus; and early labor. Along with this women who are aware that exercise is important in promotion of health and physical fitness want to start or continue exercise during pregnancy7.
The self-efficacy thought is getting increase recognition as a predictor of health behavior change and maintenance. Self-efficacy plays a vital role in preparing pregnant women for maintaining their good health and also for exercises that can ease their delivery. The value of self-effectiveness stems from direct correlation with purpose, it is supposed with the greater part of societal mental or emotional theories to be the main proximal determinants of activities8.
The exercises that stimulates breathing and blood circulation of a person is Aerobic exercises9. An aerobic training regularly for the period of trouble-free pregnancy recover or maintain physical health as well cardio respiratory fitness, increase psychosomatic wellbeing and decreases the risk for inactive standard of living associated co-morbidities. However during pregnancy routines of exercise may have to be altered to accommodate the normal anatomic and physiological variations that occur in pregnant females and to avoid side effects on fetus5.
One of the most general and discomforting problems come across in pregnancy is urinary incontinence10, 11 and is identified to have a severe harmful effect on quality of life with difficult psychological, physical and societal consequences.12 Identification and treatment of this problem is important because pregnancy and birth are most important risk factor meant for urinary incontinence development12, 13.
Urinary incontinence (UI) can be prevented by pelvic floor muscle exercises (kegel exercises) performed during the course of pregnancy. These exercises helps to reduce the short term risk of UI in women without previous incontinence, however a long term advantage has not been proven5.
Those women who previously contain urinary incontinence or for who are dry there is a strong indication with the aim of providing training and instruction for pelvic floor muscle exercises (PFMs) for the duration of the antenatal period is a way of reducing urinary incontinence within the postnatal period14.
Antenatal exercises include abdominal exercises, pelvic floor exercises (Kegel exercises), core stability, and postural education, breathing exercises, aerobic and back care. Pelvic floor exercises (Kegel exercises) are normally used prenatal trainings to strengthen the pelvic floor muscles. It is recognized that an intensive pelvic floor muscle exercise during pregnancy avoids urinary incontinence in the course of pregnancy and after delivery. Additionally, there are facts to indicate that pelvic floor muscle strengthening has been effective at shortening the 1st and 2nd stages of labour6. Pelvic floor muscle exercises can also decrease the risk of early pelvic organ prolapse15.
A Physiotherapist with practice in this branch of exercises can offer the services desired to improve confidence for the duration of pregnancy. The antenatal sessions would be concentrating on the following: nutritional advice, postural education, importance of weight reduction, breathing exercises, pelvic floor exercises, identification of high risk pregnant females and back care15.
Swimming is another safe and ideal form of exercise is pregnancy. It encourages the movement of arms and legs and increases the activity of heart and lungs. Muscle tone, flexibility and posture can be maintained by yoga. It is safe for the joints than more vigorous forms of exercises. Though, stretching helps to keep supple, though don’t overdo it. Gently opening and extending the body helps to relax body and mind16.
Low back ache is mainly the common complains throughout pregnancy that can be resolved by strengthening the abdominal and back muscles. Weight training helps to build stamina which you need during labor and delivery. Weight gain within a healthy range for the baby can be achieved by strength training throughout the pregnancy17.
According to a small number of studies, weight training may help women with gestational diabetes manage their conduction: one study suggested that resistance training can reduce the need for insulin therapy and one more found that it reduced the risk of macrosomia17.
PURPOSE OF THE STUDY
The purpose of this study is to discover awareness of gynecology rehabilitation (positioning, exercises) in pregnant women. Gynecological rehabilitation eases the delivery and postpartum period as well.
Now a day’s pregnant women do not usually induce in exercises because they do not know its benefits. The purpose of this cross-sectional survey was to identify the awareness in pregnant women about gynecological rehabilitation18.
In earlier studies, the urinary stress incontinence reported frequency of 30% of all women and may influence up to 63% of postmenopausal women in prior works. Applying rehabilitation principles to diagnosis and treatment, establish the incidence of stress incontinence to be 20 to 30% of pregnant women, or non-pregnant women, who did no particular pelvic floor exercise. A group of women, not pregnant, who did kegel exercises for pelvic floor strengthening, had only a 6% incidence of stress incontinence19.
In further studies, 50% were pregnant for the first time. While 76% of pregnant women were aware that PFMs can prevent UI, only 27% were aware that they prevented fecal incontinence and 41% considered it was usual to drip urine when pregnant, no more than 11% were working PFMEs. Females who had attended ANE (28%) were significantly more knowledgeable about pelvic floor muscles function comparatively with the ones who had not attended ANE20.
HYPOTHESIS
- H1: There is lack of awareness of gynecological rehabilitation among pregnant women.
- H2: Para-gravida females are more aware about postnatal exercises as compare to primi-gravida.
- H3: Urban population is more familiar to gynecological rehabilitation protocols.
- H4: Educated women are well informed about physical activity during pregnancy.
RESEARCH STRATEGY
This research project was based on the descriptive cross-sectional study design. The study was executed after taking permission from institutional & hospital ethical committee. Data was obtained through a pre-structured questionnaire. Approval for participating in the study was acquired through an informed consent form. Subsequently, after data entry, data was analyzed through SPSS 22.0.24
TARGETED POPULATION
The target group was pregnant women attending Dow University Hospital, Karachi
SAMPLING
158 pregnant patients were selected from gynecological OPD of Dow University Hospital, Karachi. Epi info sample size calculator was used for the estimation of sample size. Taking confidence interval 95%, margin of error 7%, reported frequency of awareness regarding physiotherapy services among pregnant women 72%.18 The final sample size came out to be 158.
INCLUSION CRITERIA
- Pregnant Women
- Irrespective of the age and gravida
EXCLUSION CRITERIA
- Pregnant women who fails to provide informed consent
RESEARCH INSTRUMENT
A pre-structured questionnaire will be used to determine the awareness level of the pregnant women regarding gynecological rehabilitation. Awareness level will be measured as per the criteria in terms of appropriate and inappropriate. There are 10 questions related to awareness of pregnant women regarding gynecological rehabilitation. Each correct answer carries 1 mark. Those pregnant women who gives the correct answer of 6 questions or more (≥60%) will be labeled as appropriate whereas those who gives correct answer of less than 6 questions (<60%) will be labeled as inappropriate. Information regarding pelvic floor muscles exercise (PFME), kegel’s, aerobics, urinary incontinence and maternal and fetal health will be noted along with the demographics characteristics like age, residence, educational status, gravida.
RESULTS
158 pregnant patients came to Gynecology OPD of Dow University Hospital, Karachi participated in the study.
Table 1 shows the qualitative data which includes all demographic factors like age, residence, education level, employment and gravida. The mean ± SD of age of patients who participated is 30.46 ± 7.144. Results of the studies showed that out of 158, 24(15.2%) patients from rural areas out of which 22(91.7%) results were inappropriate and 2(8.3%) were appropriate. On the other side 134(84.8%) patients were from urban area, 91(67.9%) results were inappropriate while 43(32.1%) were appropriate (p-value 0.018). education level was divided into primary, secondary, matriculation and more than or equal to intermediate. From which 15(9.5%) patients were qualifies till primary and out of which 15(100%) results were inappropriate. Those patients with education level till secondary were 8(5.1%) and 100% results were inappropriate. While the patient with the education level matric were 14(8.9%) and 10(71.4%) were inappropriate and 4(28.6%) were appropriate. Patients with the education level more than or equal to intermediate were 121(76.6%) out of which 80(66.1%) results were inappropriate in 41(33.9%) were appropriate (p-value 0.012).Division on the basis of employment were done as 137(86.7%) patients were unemployed out of which 102(74.5%) results were inappropriate and 35(25.5%) were appropriate. The participated patients who were employed were 21(13.3%) out of which 11(52.4%) results were inappropriate and 10(47.6%) were appropriate (p-value 0.037).
On the basis of gravida, primi-gravida patients were 38(24.1%) out of which 30(78.9%) results were inappropriate and 8(21.1%) were appropriate. Regarding para-gravida patients were 120(75.9%) out of which 83(69.2%) were inappropriate. While 37(30.8%) were appropriate (p-value 0.244)
Table 1: Qualitative data is represented by frequency; while quantitative data is represented by Mean ± SD.Chi-square test applied, p-value <0.05 taken as significant. (* denoted as significant)
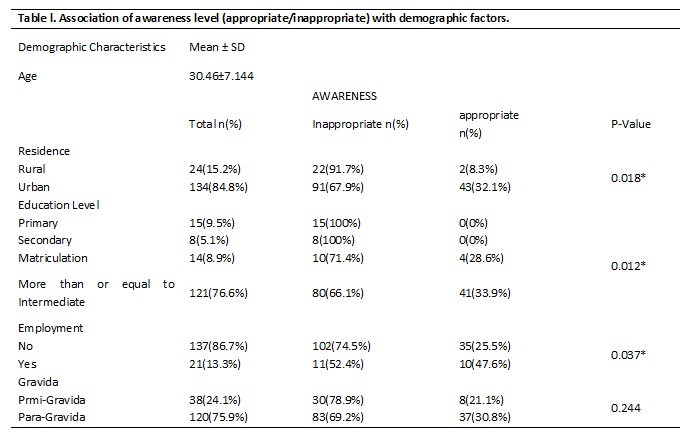
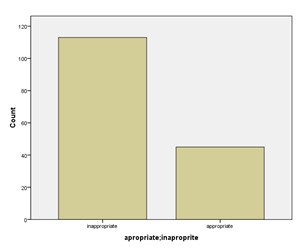
Figure1: Bar Chart; Awareness of Gynecological rehabilitation in pregnant patients (appropriate/inappropriate)
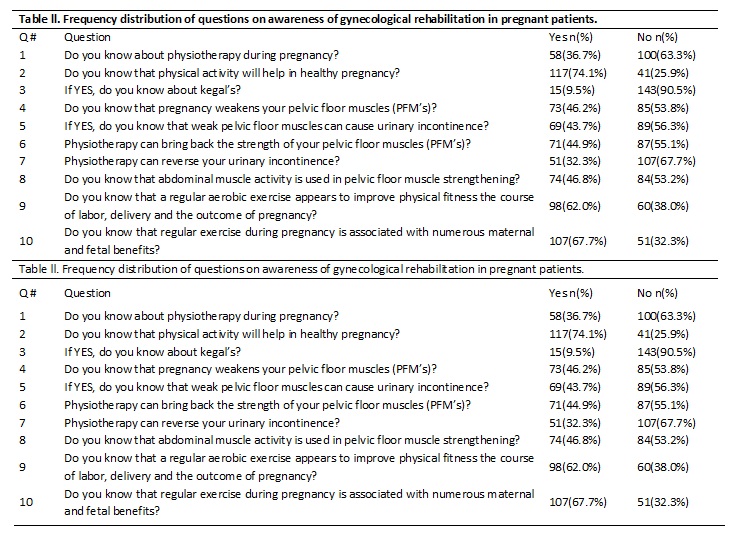
Table no 2 is based on frequency distribution of questions on awareness of gynecological rehabilitation in pregnant patients. The frequency of patients those were aware about physiotherapy during pregnancy were 58(36.7%) while 100(63.3%) patients were unaware. 15(9.5%) of patients were aware about kegal’s exercises while 143(90.5%) were unaware about it. Only 69(43.7%) patients were aware that weak pelvic floor muscles (PFMs) can cause urinary incontinence and 89(56.3%) were unaware. 51(32.3%) patients were aware that physiotherapy can reverse urinary incontinence while 107(67.7%) were unaware.
DISCUSSION
This study demonstrated the awareness of gynecological rehabilitation in pregnant patients of gynecological OPD of Dow University Hospital, Karachi. The patient participated in this study were all pregnant. Majority of patients were unemployed. From earlier published study it has been formed that qualitative features such as age, level of education and gravida (primi or para) considerably effect knowledge, perception, interest and attitude of pregnant females towards exercises.23 Likewise most of the patients participated in this study were unaware about the physiotherapy in pregnancy (benefits and outcomes). Most of them were even unaware about kegal exercises and their results, pelvic floor muscles (PFMs), importance of PFMs in urinary incontinence, generalized aerobic exercises and its effects for healthy pregnancy.
However in 2012, a study was conducted on awareness of pregnant woman about physiotherapy services at selected maternity hospital, 50 women participated in the study out of which 76% of participants were not aware about the physiotherapy services during pregnancy.18 While in our study 63.3% of patients were not aware about the physiotherapy in pregnancy. In 2014, a cross sectional study was conducted in Nigeria to check the knowledge and attitude towards exercise during pregnancy, most of them had less knowledge but they showed good response towards antenatal exercises.
Furthermore, our study showed that 53.8% participants were unaware that pregnancy can weaken our pelvic floor muscles (PFMs) and 56.3% patients were unaware that weak PFMs can cause urinary incontinence. However in March 2017 a cross sectional study was conducted on awareness, beliefs and knowledge about pelvic floor muscles (PFMs) and pelvic floor muscle exercises (PFMEs) and their results showed that 76% of participants were aware that strong PFMs can prevent urinary incontinence.18
Another research was conducted in January 2010 on effects of aerobic exercises in pregnancy and the effects of recommending healthy pregnant women to engage in regular exercises. The aspect of our study was to know that regular aerobic exercises appears to improve physical fitness, the course of labor, delivery and the outcome of pregnancy and our results showed that 62% of the participants had the awareness.
Although similar studies have been done in other countries, this study is the first of its kind in assessing the awareness of gynecological rehabilitation in Dow University Hospital, Karachi Pakistan. The need of the rehabilitation and physiotherapy is increasing day by day but people need to get aware about its benefits and effects to practice it.22 On the other hand, the study does however have some limitations. Some of the participants we faced had language barrier and those whom education level was till primary were not able to understand the questionnaire easily.21 Another study conducted in previous years concluded that more noteworthy neuromotor advancement in one-month old newborn children of practicing ladies add to the developing assemblage of proof recommending that activity during pregnancy decidedly impacts different body frameworks in the creating newborn child 24.
CONCLUSION
A majority of pregnant patients were participated and demonstrated in inadequate knowledge about gynecological rehabilitation in pregnancy. However, the patients who had awareness of gynecological rehabilitation were in minority. Information about the exercises during pregnancy considerably influences the approach towards exercises in pregnancy.
REFERENCES
- Hellwig K, Geissbuehler Y, Sabidó M, Popescu C, Adamo A, Klinger J, Ornoy A, Huppke P. Pregnancy outcomes in interferon-beta-exposed patients with multiple sclerosis: results from the European Interferon-beta Pregnancy Registry. Journal of neurology. 2020 Jun;267(6):1715-23.
- Humphries A, Thompson JM, Stone P, Mirjalili SA. The effect of positioning on maternal anatomy and hemodynamics during late pregnancy. Clinical Anatomy. 2020 Sep;33(6):943-9.
- Okafor UB, Ter Goon D. Physical activity and exercise during pregnancy in Africa: a review of the literature. BMC Pregnancy and Childbirth. 2020 Dec;20(1):1-7.
- Phillips, C., Hillard, T., Salvatore, S., Toozs-Hobson, P. and Cardozo, L., 2020. Lasers in gynaecology. European Journal of Obstetrics & Gynecology and Reproductive Biology, 251, pp.146-155.
- Saarikko J, Niela-Vilén H, Rahmani AM, Axelin A. Identifying target behaviors for weight management interventions for women who are overweight during pregnancy and the postpartum period: a qualitative study informed by the Behaviour Change Wheel. BMC pregnancy and childbirth. 2021 Dec;21(1):1-2.
- Dilaxshan V, Nasmy MN, Sandamali AA, Sugandika RK, Waththage CN, Welgama WR, Senarath MK, Bandaranayake DW. Awareness and Effectiveness of Physiotherapy Interventions among Pregnant Women Attending Antenatal Care in Gangawatakoralle.
- Duncombe D, Wertheim EH, Skouteris H, Paxton SJ, Kelly L. Factors related to exercise over the course of pregnancy including women’s beliefs about the safety of exercise during pregnancy. Midwifery. 2009 Aug 1;25(4):430-8.
- Gaston A, Cramp A, Prapavessis H. Enhancing self-efficacy and exercise readiness in pregnant women. Psychology of Sport and Exercise. 2012 Sep 1;13(5):550-7.
- McDonald SM, Isler C, Haven K, Newton E, Kuehn D, Kelley G, Chasan‐Taber L, May LE. Moderate intensity aerobic exercise during pregnancy and 1‐month infant Morphometry. Birth Defects Research. 2021 Feb 1;113(3):238-47.
- Schei B, Johannessen HH, Rydning A, Sultan A, Mørkved S. Anal incontinence after vaginal delivery or cesarean section. Acta obstetricia et gynecologica Scandinavica. 2019 Jan;98(1):51-60.
- Whitford HM, Alder B, Jones M. A cross-sectional study of knowledge and practice of pelvic floor exercises during pregnancy and associated symptoms of stress urinary incontinence in North-East Scotland. Midwifery. 2007;23(2):204-17.
- Lasserre A, Pelat C, Gueroult V, Hanslik T, Chartier-Kastler E, Blanchon T, Ciofu C, Montefiore ED, Alvarez FP, Bloch J. Urinary incontinence in French women: prevalence, risk factors, and impact on quality of life. European urology. 2009 Jul 1;56(1):177-83.
- Memon H, Handa VL. Pelvic floor disorders following vaginal or cesarean delivery. Current opinion in obstetrics & gynecology. 2012 Oct;24(5):349.
- Hill A-M, McPhail SM, Wilson JM, Berlach RG. Pregnant women’s awareness, knowledge and beliefs about pelvic floor muscles: a cross-sectional survey. International urogynecology journal. 2017;28(10):1557-65.
- Sajan M. Awareness of physiotherapy interventions among pregnant females in antenatal clinics, Buffalo city municipality, Eastern Cape, South Africa. 2013.
- McMillan AG, May LE, Gaines GG, Isler C, Kuehn D. Effects of Aerobic Exercise during Pregnancy on One-Month Infant Neuromotor Skills. Medicine and science in sports and exercise. 2019 Jun 13;51(8):1671-6..
- Barakat R. An exercise program throughout pregnancy: Barakat model. Birth Defects Research. 2021 Feb 1;113(3):218-26..
- Afroz F. Pregnant women’s awareness about physiotherapy services at selected maternity hospital: Bangladesh Health Professions Institute, Faculty of Medicine, the University of Dhaka, Bangladesh); 2015.
- Maly B. Rehabilitation principles in the care of gynecologic and obstetric patients. Archives of physical medicine and rehabilitation. 1980;61(2):78-81.
- Bayat, M., Eshraghi, N., Naeiji, Z. and Fathi, M., 2021. Evaluation of Awareness, Adherence, and Barriers of Pelvic Floor Muscle Training in Pregnant Women: A Cross-sectional Study. Female pelvic medicine & reconstructive surgery, 27(1), pp.e122-e126.
- Ali, S.H., Rizvi, S.A.S. and Naqvi, M., 2013. Physical activity level in medical students of the Ziauddin University, Karachi. Pakistan Journal of Rehabilitation, 2(1), pp.31-34.
- Watson ED, Oddie B, Constantinou D. Exercise during pregnancy: knowledge and beliefs of medical practitioners in South Africa: a survey study. BMC pregnancy and childbirth. 2015;15(1):245
- Sultan F, Hasan Z. PARENTAL PERCEPTION ABOUT WESTERN CARTOON ON CHILD’S MENTAL HEALTH IN PAKISTAN. Pakistan Journal of Rehabilitation. 2020;9(2):48-53.
- McMillan AG, May LE, Gaines GG, Isler C, Kuehn D. Effects of Aerobic Exercise during Pregnancy on One-Month Infant Neuromotor Skills. Medicine and science in sports and exercise. 2019 Jun 13;51(8):1671-6.