
ABSTRACT
OBJECTIVE
To find the association of over-weight and obesity with high frequency of co-morbid conditions
STUDY DESIGN
Cross-Sectional Study
SAMPLE SIZE
This study is conducted at Ziauddin Hospital Out Patient Department. A sample of 200 over weight and obese clients were included by simple random sampling to find out the relation of co-morbidities with overweight and obesity.
OUTCOME MEASURES:
Patients were categorized as overweight and obese by calculating their Body Mass Index (BMI).
RESULTS
Out of 200 patients it is was found that there is an increase in secondary complications such as depression, hypertension, stroke, cardiac diseases, knee pain, and kidney disease. The statistics also showed that generally overweight and obese clients had a higher of smoking and alcohol consumption. There is a marked association of co-morbidities conditions within clients with higher BMI than normal.
CONCLUSION
This study provides a comprehensive estimate of the strong association of co-morbidities attributable to overweight and obesity using standardized and consistent definitions and methodologies. Our findings confirm that high BMI will carry a profound health burden and will have a significant impact on health expenditures.
Key Words
Obesity, Body Mass Index (BMI), Co Morbids, Depression, Stroke, Hypertension,
Diabetes Mellitus
Sunny Kumar
Physiotherapist
Physiotherapy Department
Ziauddin Hospital
Nabiha Mujahid Faruq
Senior Physiotherapist
Physiotherapy Department
Ziauddin Hospital
Amna Aamir Khan
Assistant Professor
Ziauddin College of Physical Therapy
Ziauddin University
Kailash Kumar
Clinical Physical Therapist
Maesa Jaffer
Physical Therapist
Physiotherapy Department
Ziauddin Hospital
[Kumar S, Faruq NM, Khan AA, Kumar K, Jaffer M. Is Over-Weight and Obesity associated with High Frequency of Co-Morbid Conditions? Pak. j. rehabil. 2012;1(2):47-50]
INTRODUCTION
Overweight and obesity are simply defined as conditions of abnormal or excessive fat accumulation in adipose tissue, to the extent that health may be impaired1. It is a resultant of excess body fat. A standard marker for body content is the body mass index (BMI). There are other parameters to calculate over weight or Obesity such as waist circumference, waist-hip ratio, skinfold, and percent body fat measurements2 BMI: body mass index (BMI) is calculated as: weight (Kg)/Height (m2). In clinical terms, a person with a BMI between 25.0 and 29.9 Kg/m^2 is called over weight and One with a BMI greater than 30 Kg/m^2 is called Obese 3,4.
The excess intake of food results in increase in fat stores which causes increase in body weight. The causes of obesity are complex and poorly understood. Genes also play an important role in determining food intake or energy metabolism along with low activity caused by a sedentary life style. It is evident through previous studies that there is a rapid increase in the prevalence of overweight and obesity during the past 2 to 3 decades 5-12.
Obesity is an epidemic of the 21st century, and is a major causal issue for various other metabolic disorders. According to a worldwide estimation by the World Health Organization (WHO), in 2005 there were about 1.6 billion overweight persons aged 15 years and above and among them at least 400 million adults were obese6. In most of the Asian countries the prevalence of overweight and obesity has increased many folds in the past few decades and the magnitude varies between countries 9-18 South East Asia and Western Pacific region are currently facing an epidemic of diseases associated with obesity such as diabetes and CVD 8.9.
Overweight and obesity represent a rapidly growing threat to the health of populations in an increasing number of countries. Indeed, they are nowadays so frequent that they are replacing more traditional problems such as under nutrition and infectious diseases as the most significant causes of ill-health.
Obesity co-morbidities include coronary heart disease, hypertension and stroke, certain type of cancer, non-insulin-dependent diabetes mellitus, gallbladder disease, dyslipidaemia, osteoarthritis, gout, pulmonary diseases and sleep apnea. In addition, the obese put up with common bias, discrimination, on the part not only of the general public but also of health professionals, and this may make them unenthusiastic to seek out medical assistance. World Health Organization therefore convenes a discussion on obesity to review current epidemiological information, causative factors and related consequences, and this report presents its conclusions and recommendation. In particular, the Consultation measured the system for classifying overweight and obesity based on the BMI, and concluded that a coherent system is now available and should be adopted globally. The discussion also concluded that the fundamental causes of the obesity epidemic are sedentary lifestyles and high-fat energy-dense diet, both resultant from the intense changes taking place in society and the behavioral patterns of communities as a consequence of increased urbanization and industrialization and the disappearance of traditional lifestyles7.
Economic improvement over the last 50 years in most of the countries has resulted in greater affluence and to diets that are higher in fats especially saturated fat, cholesterol, and cultured carbohydrates and low in polyunsaturated fatty acids and dietary fiber. This nutrition trend has also been accompanied with a sedentary lifestyle and increased level of stress. Therefore, the prevalence of obesity and other non-communicable diseases has raised steeply 19, 20.
The nutrition transition can be noticed in all high-income countries in the region (Arab Gulf Countries), and most middle wages countries, especially in urban areas, and in a few high or socioeconomic sectors of poor countries 21-23. Several studies have reported the association of dietary patterns with obesity and central adiposity; most of these came from Western countries. A reduction in fat intake to around 20-25% may be helpful in weight reduction and minimize the risk of energy imbalance and weight gain in sedentary individuals. Although there is strong evidence that certain genes have an influence on body mass and body fat, mostly do not qualify as necessary genes, i.e., genes that to cause obesity when two copies of the defective allele are present; it is likely to be many years before the results of genetic research can be applied to the problem23. Different methods for the treatment of increases BMI are described including dietary management, physical exercises and activities, and anti-obesity drugs, with gastrointestinal surgery being reserved for extreme cases. Overweight and obesity are major cause of co-morbidities which can lead to further morbidity and mortality.
The objective of this study is to assess the relation of co morbidities with overweight and obesity which can be done by survey. The articles obtained from the literature search prospective cohort study of the general population of a Western country (countries in Europe or North America, Australia or New Zealand), significant outcomes, a sample size of at least 200 subjects, and risk estimation based on the incidence of disease instead of the mortality rate of disease 13,15. For large cohorts with several articles meeting the defined criteria, the mostly recent article.
The aim of the study was to determine relation between co-morbidities in clients who are overweight or obese clients coming for physiotherapy in a tertiary care hospital.
METHODOLOGY
Study Design
It is a Cross sectional study.
Settings
The study will be conducted at the Physiotherapy Department of Ziauddin Hospital North Nazimabad and Clifton campus.
Sample Size
200 patients of both genders are included in this study with a global prevalence of 15% to 18% calculated on EPI calculator11.
Sampling Techniques
Simple random sampling is used for this study.
Sample Selection
Inclusion Criteria
On the basis of BMI all over weight and obese patient coming for physiotherapy treatment were included.
Exclusion Criteria
Patients less than 18 years or more than 65 years were not included in this study.
Data Collection Tool
Body Mass Index calculation. Self-Administered Questionnaire.
RESULTS
Our research was conducted on a sample size of 200 patients with mean age of 49.4 ± 11.9 and mean BMI of 29.3 ± 3.3. It was seen that 131 (65.5%) were females while male was only 69 (34.5%).
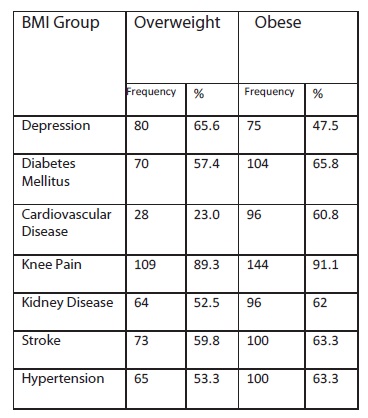
This study focused on different co morbid associated with overweight and obesity. It was seen that 65.6% patients of depression were overweight and 47.5% were obese. In the same way it was observed that hypertension and stroke was more prevalent in obese patients. 63.3% of obese patients had hypertension and stroke while 53.3% of the overweight patients had hypertension and 59.8% had stroke.
The association of obesity was seen with some other diseases and it was found to be closely related. It was found that Kidney diseases, heart diseases, diabetes mellitus and knee pain are also very common in obese patients. Among overweight patients 23% were suffering from cardiovascular disease and 52.5% kidney diseases while in obese patients 60.8% had cardiovascular disease and 62% kidney disease. Similar pattern is observed in cases of diabetes mellitus. Obese patients were more prone to have diabetes mellitus (65.8%) and overweight (65.6%).
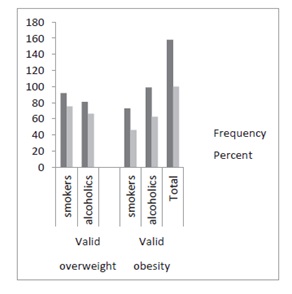
In this study we came across the fact that the consumption of alcohol and smoking was more commonly seen in overweight patients compared to the obese. 62% alcoholics and 75% smokers among the overweight patients and 60% alcoholics and 42% smokers in obese patients.
Alcohol Consumption and Smoking
DISCUSSION
It has been observed in our study that overweight and obesity are strongly associated with many other of co-morbids including diabetes mellitus, hypertension, stroke, cardiovascular disease, kidney disease, knee pain and depression. It was also seen that depression and knee pain were most common among overweight and obese individuals. Other researchers have also shown high prevalence of both depression and obesity in their studies and the fact that they both carry an increased risk for cardiovascular disease as well 24,25. A potential association between depression and obesity has been presumed and repeatedly been examined and confirmed in different studies by de wit L et al, Faith MS et al and Scott KM et al 26-28. In another study by de wit L et al there is a significantly positive association between depression and obesity in the general population, which appeared to be more marked among women 29. This study also supports the association of overweight and obesity with depression.
Foy CJ. et al in his study has discussed the association of obesity with a number of comorbid conditions such as type 2 diabetes and knee pain. According to him, the etiology of knee pain is multifactorial, and can range from chronic diseases such as osteoarthritis (OA) to acute trauma but at the same time he mentioned that it is a modifiable risk factor for the development and treatment of knee pain30. Similarly in our study it has been evidently seen that knee pain is a common complaint in obese and overweight individuals. It is a major problem faced by them. Other researches also support this association.
Alcohol and Smoking both are risk factors for many diseases such as hypertension, stroke, heart disease, etc. In this study we came across the fact that the consumption of alcohol and smoking was not commonly seen in normal individual’s compared to the overweight and obese patients. Other diseases like cardiovascular disease, Kidney disease and diabetes mellitus have also been seen in abundance in these patients.
CONCLUSION
In conclusion, this study provides a comprehensive estimate of the incidence of co-morbidities attributable to overweight and obesity using standardized and consistent definitions and methodologies. Our findings confirm that overweight and obesity carry a profound health burden and will have a significant impact on health expenditures.
REFERENCE
- World Health Organization WHO. Obesity and managing the global epidemic: WHO Technical Report Series 894. Geneva, Switzerland; 2000. http://whqlibdoc.who.int/trs/WHO_TRS_894.pdf
- World Health Organization (WHO), Physical status: the use and interpretation of anthropometry, WHO Technical Report Series 854, WHO, Geneva, Switzerland;1995.http://whqlibdoc.who.int/trs/WHO _TRS_854.pdf
- Pi-Sunyer FX. Co-morbidities of overweight and obesity: current evidence and research issues. Med Sci Sports Exerc 1999;31(11):602 -8.
- BMI classification Global Database on Body Mass Index [internet]. World Health Organization; 2006.cited July 27, 2012. Available from:http:// apps.who.int/bmi/index.jsp?introPage=intro_3.html
- Parag V, Woo J, Larn TH, Woodward M, Bennett DA.Central obesity and risk of cardiovascular disease in the Asia Pacific Region. Asia Pac J Clin Nutr 2006;15(3):287-292.
- Hall JE. Guyton and Hall textbook of medical physiology. 11thEdition. New Delhi India:Elsevier Publisher 2006;547-8.
- Haslam DW, James WP. Obesity. Lancet 2005;366(9492):1197-209
- International Diabetes Federation, Diabetes Atlas, 4th edition, 2009. Available online: http://www.idf.org/diabetesatlas
- Yoon KH, Lee JH, Kim JW, Cho JH, Choi YH, Ko SH, et al. Epidemic obesity and type 2 diabetes in Asia. The Lancet 2006;(368)9548:1681–88
- Flegal KM, Carroll MD, Ogden CL, Curtin LR. Prevalence and trends in obesity among US adults, 1999- 2008 JAMA 2010;303(3):235–41
- Griffiths PL, Bentley ME. The nutrition transition is underway in India. Journal of Nutrition 2001;131(10):2692–2700
- Sidik SM, Rampal L. The prevalence and factors associated with obesity among adult women in Selangor, Malaysia. Asia Pacific Family Medicine. 2009;8(1):1–6
- Prentice AM. The emerging epidemic of obesity in developing countries. International Journal of Epidemiology 2006;35(1):93–99
- Lin YC, Yen LL, Chen SY. Prevalence of overweight and obesity and its associated factors: findings from National Nutrition and Health Survey in Taiwan, 1993-1996. Preventive Medicine 2003;37(3):233–41
- Deurenberg-Yap M, Chew SK, Lin VFP, Tan BY, van Staveren WA, Deurenberg P. Relationships between indices of obesity and its comorbidities in multiethnic Singapore. International Journal of Obesity 2001;25(10):1554–6
- Ko GTC, Wu MMF, Tang J, Wai HPS, ChanCHS,Chen R. Body mass index profile in Hong Kong Chinese xadults. Annals of the Academy of MedicineSingapore 2001;30(4): 393–96
- Kim DM, Ahn CW, Nam SY. National prevalence of obesity: prevalence of obesity in Korea. Obesity Reviews 2005;6(2):117–21
- Aekplakorn W, Chaiyapong Y, Neal B. Chariyalertsak S, Kunanusont C,Phoolcharoen W, Suriyawongpaisal P. Prevalence and determinants of overweight and obesity in Thai adults: results of the Second National Health Examination Survey. Journal of the Medical Association of Thailand 2004;87(6):685–93
- World Health Organization, Obesity and Overweight, Fact Sheet No. 311, WHO Media centre; 2006. Available online: http://www.who.int/ mediacentre/factsheets/fs311/en/print.html
- Galal O. Nutrition-related health patterns in the Middle East, Asia Pacific Journal of Clinical Nutrition 2003;12(3):337–43
- Ng SW, Zaghloul S, Ali HI, Harrison G, Popkin BM.The prevalence and trends of overweight, obesity and nutrition-related non-communicable diseases in the Arabian Gulf States. Obesity Rev 2011;12(1):1–13
- Benjelloun S. Nutrition transition in Morocco. Public Health Nutrition 2001;5(1A):135–40
- Musaiger AO. Overweight and Obesity in Eastern Mediterranean Region: Prevalence and Possible Causes. Journal of Obesity 2011; 17
- Global Health Observatory (GHO). Obesity and overweight. World Health Organization . http://www.who.int/dietphysicalactivity/publicatio ns/facts/obesity/en/. Accessed February 9, 2009
- Penninx BW, Beekman AT, Honig A, Deeg DJ, Schoevers RA, van Eijk JT, van Tilburg W. Depression and cardiac mortality: results from a communitybased longitudinal study. Arch Gen Psychiatry 2001; 58(3):221-7
- de Wit LM, van Straten A, van Herten M, Penninx BWJH. Cuijpers P. Depression and body mass index, a u-shaped association. BMC Public Health 2009;9:14
- Faith MS. Matz PE. Jorge MA. Obesity-depression associations in the population. J Psychosom Res 2002;53(4):935-42
- Scott KM. McGee MA. Wells JE. Oakley Browne MA. Obesity and mental disorders in the adult general population J Psychosom Res 2008;64(1):97-105
- de Wit L, Luppino F, Annemieke, van Straten A, Penninx B, Zitman F, Cuijpers P. Depression and obesity: A meta-analysis of community-based studies. Psychiatry Research 2010;178(2):230-35
- Foy CJ, Lewis E, Hairston KG,Miller GD, Lang W, Jakicic JM, Rejeski WJ, Ribis PM, Walkup MP, Wagenknecht LE. Intensive Lifestyle Intervention Improves Physical Function Among Obese Adults With Knee Pain: Findings From the Look AHEAD Trial. Obesity 2011;19(1):83–93.