ABSTRACT
OBJECTIVE
To Study the effectiveness of Home management versus OPD management in Low back pain patients.
STUDY DESIGN
The study was a quasi-experimental study design.
STUDY SETTINGS & PARTICIPANTS
Participants aged between 30 to 70 years suffering from low back pain for more than 3 months were inducted in the study. They were divided into two groups, one which was provided intervention at home and the other which was given physiotherapy in OPD setting.
INTERVENTIONS
A pre and post assessment was done at 6 months based on Oswestry low back pain disability questionnaire. Analysis was done by application of Independent sample t test. P value less than 0.05 was taken as significant.
RESULTS
A total of 100 participants were equally divided for OPD and home management. Oswestry low back pain disability questionnaire was administered pre and post intervention and Independent T test was applied to find the difference between the mean pretest and posttest scores for OPD and home managed patients which were taken 6 months apart. A significant difference was observed as p value was < 0.00
CONCLUSION
The results of the study concluded that OPD management for chronic low back pain not only reduces pain but also reduces chance of disability. But patient satisfaction was higher in home manage group in comparison to OPD in personal care.
Key Words
Low Back Pain, Lumbago, Home Management, OPD Management, Physiotherapy LBP, Home vs OPD Physiotherapy
Muhammad Sarfraz
Assistant Professor
Ziauddin College of Physical Therapy
Ziauddin University
Erum Naz
Physiotherapist
Physiotherapy Department
National Medical Center
Kulsoom Habib
Physiotherapist
Physiotherapy Department
Al-Mustafa Trust
Syed Hassan Danish
Sr. Lecturer
Department of Community
Health Sciences
Ziauddin University
Farah Ahmed
Assistant Professor
Department of Community
Health Sciences
Ziauddin University
[Sarfraz M, Naz E, Habib K, Danish SH, Ahmad F. Effectiveness of Home Management versus OPD Management in Low Back Pain Patients. Pak. j. rehabil. 2012;1(2): 22-27]
INTRODUCTION
The spine consists of 33 vertebrae and five regions that is cervical (7 vertebrae), thoracic (12 vertebrae), lumber (5 vertebrae), sacral (5 vertebrae), and coccyx (4vertebrae). Each protecting the spinal cord and provide stability to torso 1, 2. The spine has got two types of curves, primary and secondary 3-5. Primary curves are thoracic and sacral where secondary curves are cervical and lumber curves 6,7. Cervical and lumber curves being most mobile and are more prone to develop different problems which can be due to posture, muscle spasm or may be due to the problem in disc, present in between the vertebrae 8-11.
The largest cause of work-related absence and one of the most common medical problems12 affecting 8 out of 10 people at some point during their lives is low back pain. Low back pain means a pain, or ache, anywhere on the backside of body, in between the bottom of the ribs and the top of the legs13, the pain can come on suddenly, slowly or be the direct result of a fall or injury14. In most cases, the pain lasts from a few days to a few weeks and usually clears up after about six weeks5. Area of Lumbar spine encompass the distance from the 1st lumbar vertebra to the 1st sacral vertebra. The most frequent site of low back pain is in the 4th and 5th lumbar segment 12. It is predicted that it will affect up to 90% of the world’s population at some point in their lives, mostly affecting the age group between 35 and 55 years14. Risk factors for LBP include heavy physical work, frequent bending, twisting and lifting; and prolonged static postures. Psychosocial risk factors include anxiety, depression and mental stress at work.
LBP can be arbitrarily divided into acute, sub-acute or chronic, depending on the duration of the complaints. Acute LBP persists for less than six weeks, sub-acute is between six weeks and three months and chronic LBP lasts longer than three months15. It is believed that 80-90% of LBP episodes are acute and resolve within six weeks irrespective of the administration or type of treatment. However, 5-10% of LBP patients will develop chronic problems16.
T M. Damush et al 2003 found that self-management program can improve and maintain functional status, mental functioning, and self-efficacy to manage future symptoms for 1 year among primary care patients with ALBP17. K. Cooper et al 2008 determined the patient-centeredness from the patient’s perspective in the context of physiotherapy for chronic low back pain. There were 25 patients who received physiotherapy for low back pain within 6 months. There was evidence of betterment in chronic low back pain18.
Physiotherapy is one of the effective plans for LBP and can be provided at home as well as in OPD. Exercises and some physiotherapy modalities like hot or cold therapy 19can be given in some cases, pain modulating agents like TENS20 can be used for temporary pain relief. Postural control is taught to the patient to overcome any muscle imbalance.
Advantage at home is the level of comfort for patient and especially for those patients who are not able to come in OPD. Advantage at OPD is presence of special modalities. Research is scarce where both the methods were compared both internationally and at the local level. Therefore, we want to compare the effectiveness of HOME management and OPD management in low back patients.
MATERIAL AND METHODS
This was the study of low back pain patients in which 50 participants received physiotherapy sessions at National Medical Center Karachi and 50 participants followed only home program. Handouts and written educational material was given to participants showing recommended exercises with proper body mechanics. The questionnaire was filled at beginning of research and after 6 months by the participants for evaluation.
Study Design
This was a quasi experimental trial where comparison was done between home management and opd management for LBP
Duration of Study
The duration of study was 6 months
Sample Size
The size of 100 people received physiotherapy for Low Back Pain. Sample size was calculated on the basis of prevalence 7% 21 a total of 100 patients were selected. n= Z2 P (1-P)/d2 0.05 = (1.96)2 0.07 =3.8416×0.07×0.93/ (0.05)2/0.0025 = 100
Sampling Techniques
Sampling technique was purposive sampling
Inclusion Criteria
Patients were selected having age between 30 to 70 years and having LBP greater than three months of duration.
DATA COLLECTION PROCEDURE
Patients coming to the outpatient department of National Medical Center were included in this study. Those who fulfilled the inclusion criteria were asked to sign the informed consent after being explained the objectives and duration of the study. On the choice of the participants, they were assigned either the OPD management group or home management group. All the participants were interviewed and were asked to fill the questionnaire at the time of induction in the study. The questionnaire consisted of close ended questions, First part recorded the demographic profile of the patients and the second part of Questionnaire was based on reliable standard scale (Oswestry low back pain disability), one of the most commonly used outcome measures for individuals with low back pain. The Oswestry Questionnaire encloses ten questions about patients. On every question the patient can choose out of 6 possible answers, but only one can be marked. When the patient doubt of several possibilities, he should mark the one which fits the best. For every part, score is minimal 0 and maximal 5. The lower the score the less restrictions, patient experiences during his daily activities. The sample of 100 participants was divided into two groups, one coming to OPD continuously for physiotherapy treatment while other group was given home programme only (but they came at regular interval for follow ups). Than after six months patients were re examined at National Medical Center and were asked to fill the same questionnaire. Voluntary consent was taken from the patients and confidentiality assurance was provided to those who agreed to participate in the study.
DATA ANALYSIS PROCEDURE
Data was entered and analyzed on SPSS version 20. Descriptive variables were both numerical and categorical in nature. Mean and standard deviation was taken out for the numerical variables whereas frequencies and percentages were taken out for categorical variables. Pooled and Paired t test was applied for finding the difference in the mean scores of pre and post test of home versus OPD management groups. P value less than 0.05 was taken as significant.
RESULTS
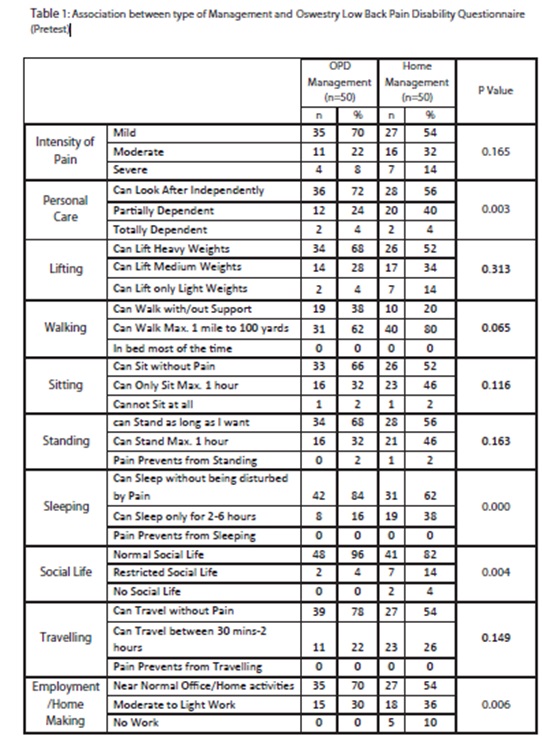
A total of 100 participants were recruited in the study with a male to female ratio of 1:2 (33% males – 67% females).The participants were selected on the basis of chronic low back pain greater than 3 months. They were equally divided into OPD management and home management. At the time of recruitment they were given a pretest based on the Oswestry Low back pain questionnaire which was repeated after an intervention period of 6 months. The questionnaire was based on routine daily activities and was divided into 10 areas which assessed the effect of pain on their day to day activities.
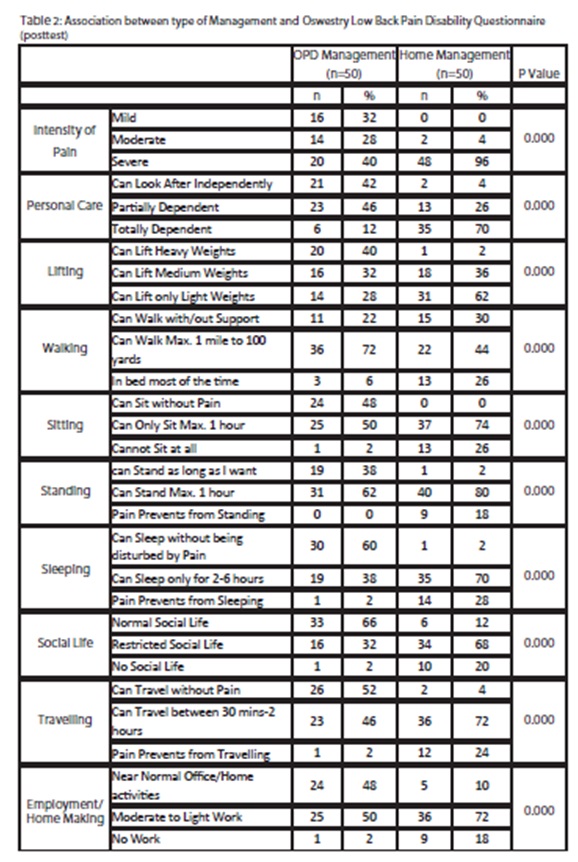
Independent T test was applied to find the difference between the mean pretest and posttest scores for OPD and home managed patients which were taken 6 months apart. A significant difference was observed as p value was 0.000. When paired t test was applied to find the difference in the pre and post home scores of home managed group mean score for pretest was 36.42±6.9 and for the posttest was 16.38±6.3 with a highly significant p value of 0.000. When paired t test was applied to find the difference in the pre and post home scores of OPD managed group mean score for pretest was 19.42±9.8 and for the posttest was 10±8.9 with a highly significant p value of 0.000.
When intensity of pain was compared between the pretest and posttest and type of pain management there was a reduction of severity of pain from 40%(n=20) to 8%(n=4) in OPD treated patients as compared to home treated patients where reduction was seen from 96%(n=48) to 14%(n=7). Significant reduction in the number of people suffering from pain was observed. Initially in the pretest, n=34(68%) of the people in the OPD management group had moderate to severe pain, number decreased to n=15(30%) after 6 months. As compared to home management group where initially all the participants had moderate to severe pain after 6 months their number decreased to n=23(46%) Table 1 and Table 2.
Regarding personal care, number of participants who were able to take care of themselves independently in the OPD managed group improved significantly from n=21(42%) to n=36(72%) after six months of intervention. Significant difference was also observed in the home managed group as the numbers increased from n=2(4%) to n=28(56%) Table 1 and Table 2
Regarding the impact of chronic pain on social life in the OPD managed group n=33(66%) people had a normal social life and remaining had restricted. Their number improved to n=48(96%) after 6 months of intervention. Whereas in the home managed group initially there were only n=6(12%) people who had normal social life and after 6 months their number rose to n=41(82%).
When asked about the effect of chronic pain on either employment or home making it was observed that initially there were n=24(48%) in OPD managed group who were able to perform near normal duties. After 6 months their number augmented to n=35(70%). In home managed group only n=5(10%) were able to perform their duties as compared to n=27(54%) after 6 months of intervention.
The effect of chronic pain on travelling when assessed revealed that n=26(52%) were able to travel without any pain but after 6 months of intervention the number escalated to n=39(78%) in OPD managed group. Significant difference was observed in the home managed group where 50% of participants showed improvement after 6 months.
Regarding the other variables that were assessed in their daily activities lifting of weights showed that initially n=20(40%) were able to lift heavy weights and after intervention their number ascended to n=34(68%) in the OPD managed group. As compared to OPD managed group marked improvement was seen in home managed group where 50% of participants showed improvement after 6 months.
Initially n=11(22%) participants were able to walk regardless of miles travelled and with or without support in the OPD managed group. Their number was increased by n=19(38%) after 6 months of intervention. In home managed group there were 13(26%) people who were bed ridden. After the intervention period they were able to walk a few miles without pain hindering their walking. After the intervention period the number of people in whom chronic pain restricted them to bed became negligible in both groups.
Initially n=24(48%) participants were able to sit without pain for longer duration of time in OPD managed group. After 6 months intervention another 9 participants showed improvement. Marked improvement was observed in home management group. Initially there was no one in this group who could sit without pain but after intervention n=26(52%) people were able to sit without pain for longer duration.
For how long participants who were assigned in the OPD managed group can stand without being affected with pain initially it was n=19(38%) but after 6 months intervention the number levitated to n=34(68%). In the home managed group there was only 1 participant in this category but after 6 months n=28(56%) participants showed improvement and they were able to sit without pain.
When inquired about sleeping n=30(60%) of the participants in OPD managed group could sleep without being disturbed by pain and their number was significantly increased to n=42(84%) after 6 months. Marked improvement was observed in the home managed group where initially there was only one participant who was able to get a proper night sleep but later on the number increased to n=31(62%) after intervention of 6 months.
DISCUSSION
The effectiveness of home management versus OPD management in low back pain patients was assessed using a self administered questionnaire. The two groups were followed over a period of six months and pre and post test were carried out on all the 100 participants.
The pain intensity was shown to improve from 40% to 8% in OPD managed group in our research where a similar research conducted by K. Cooper stated betterment in chronic low back pain18. He inducted 25 patients receiving physiotherapy for low back pain for 6 month. French S, Cameron stated that heat therapy cold compression therapy can reduce symptoms of acute and sub acute low back pain19 similarly our study revealed that use of the same modalities with manual therapy improved pain by 38%. Parallel study conducted by Hollinghurst S, sharp D, Ballard K, et al stated that Massage (manual) therapy can provide relief in pain22. Regarding home management, T.M. Damush et al17 affirmed that self-management program can improve LBP. He conducted a research on Long-term Effects of a Self-management Program for Patients with Acute Low Back Pain. Similarly we noticed that the group following home programme in our study revealed 82% betterment in Pain.
Sarno, John revealed Education and attitude, cognitive therapy and progressive relaxation therapy can reduce chronic pain23, and our study confirmed the same results when respondents took sessions in OPD and showed improvement up to 33% in social life.
When comes to personal care Damush TM17 stated marked improvement in functional status, mental functioning, and self-efficacy when managed at home, the same results were reflected by our study which revealed 52% improvement in personal care.
Ebadi S et all conducted a research and concluded that the therapeutic ultrasound and exercise treatment for chronic non specific low back pain is beneficial and found Both function (17%) and pain (24%) improved post treatment14 similarly our research showed 48% to 70% improvement in OPD managed group and 10% to 54% improvement in home managed group.
DA Hurley conducted a research to see sleep disturbance in chronic low back pain. He took three intervention groups, one supervised exercise group, second walking programme group and third usual physiotherapy group and concluded the major improvement was seen in walking and supervised exercise group25 like our study revealed improvement in sleep pattern after having supervised OPD sessions.
The major limitation was that confounders like taking pain killers were not taken into account leading to information bias. Occupational history was not asked which could have led to selection bias. Compliance of home managed group for treatment could not be assessed that.
CONCLUSION
The results of the study concluded that OPD management for chronic low back pain not only reduces pain but also reduces chance of disability. But patient satisfaction was higher in home manage group in comparison to OPD in personal care.
REFERENCE
- O’Rahilly R, Müller F, Carpenter S, Swenson R. Basic Human Anatomy [Internet]. W B Saunders Co; 1982, Revised 2008. Available from: http://www.dartmouth.edu/~humananatomy/part _7/chapter_39.html.
- Letts RM, Jawadi AH. Types of congenital spinal deformities [Internet]. [updated 2012 Feb 7] Available from: http://emedicine.medscape.com/article/1260442- overview
- Mark F. Seifert.The Complete Idiot’s Guide to Anatomy Illustrated[Internet]. ALPHA; 2008 Jul 01. Available from: . http://idiotsguides.com/static/quickguides/scienc enature/anatomy-101-the-spine.html.
- Aebi M.The adult scoliosis. Eur Spine J. 2005;14(10):925-948.
- Akbarnia BA, Marks DS, Boachie-Adjei O, Thompson AG, Asher MA. Dual growing rod technique for the treatment of progressive early-onset scoliosis: a multicenter study. Spine. 2005;30(17):46-57.
- Bridwell K. Spinal curves [Internet]. [updated 2013 Oct 01] Available from: http://www.spineuniverse. com/anatomy/ spinal-curves.
- Anderson SM. Spinal Curves and Scoliosis. Radiologic technology. 2007; 79(1) Available from: http://www.mccc.edu/~petroskw/outlines/rd_128/ Spinal_Curves_Scoliosis.pdf.
- R C. Schafer. Symptomatology and Differential Diagnosis. In: The lumbar and sacral areas. available from: http://www.chiro.org/ ACAPress/ Lumbar_and_Sacral_Areas.html
- Nordqvist, Christian. What Is Back Pain? What Causes Back Pain?. [Internet] Medical News Today; 2009 Dec 03. [cited 2013 July 08]. Available from: URL: http://www.medicalnewstoday.com/ articles/172943.php.
- Petersen T, Larsen K, Nordsteen J, Olsen S, Fournier G, Jacobsen S. The McKenzie method compared with manipulation when used adjunctive to information and advice in low back pain patients presenting with centralisation or peripheralisation. A randomised controlled trial. Spine 2011;36:1999- 2010.
- Carolyn Kisner; Lynn Allen Colby. Therapeutic Exercise: Foundations and Techniques; 6th Edition. F. A. Davis Company
- Waddell G. A New Clinical Model for the Treatment of Low Back Pain. Spine 1987;12(7): 632-644.
- Moffett J. Richardson G, Sheldon, T. Maynard, A. Back Pain its Management and Cost to Society [Internet]. Discussion paper 129. University of York. February 1995. Available from: http://www.york.ac. uk/media/che/documents/papers/discussion papers/CHE%20Discussion%20Paper%20129.pdf
- Mierzejewski M, Kumar S. Prevalence of low back pain among physical therapists in Edmonton, Canada. Disabil Rehabil. 1997 Aug;19(8):309-17.
- Leijten A.O.J. Reasons for patients discontinuing chiropractic care and subsequent recurrences of low back pain. Anglo-European College of Chiropractic, Academic Year 2008/2009, MChiro. Available from: http://www. chiropractieoosterhout. nl/images/upload/Project.pdf
- Patel A.T., Ogle A.A. Diagnosis and management of Acute Low Back Pain. Am Fam Physician. 2000 Mar 15;61(6):1779-1786.
- Teresa M. Damush.T.D. The Long-term Effects of a Self-management Program for Inner-city Primary Care Patients With Acute Low Back Pain. Arch Intern Med. 2003;163:2632-38.
- Molumphy M, Unger B, Jensen GM, Lopopolo RB. Incidence of work-related low back pain in physical therapists. Physical therapy. 1985;65(4):482-6. Epub 1985/04/01.
- French S, Cameron M, Walker B, Reggars J, Esreman A. A Cochrane review of superficial heat or cold for low back pain.Spine2006;31(9):998-06.
- Khadilkar A, Odebiyi DO, Brosseau L, Wells GA. Trancutaneous electrical nerve stimulation versus placebo for chronic low-back pain. Cochrane Database Syst Rev 2008;4
- Thomas E, Silman AJ, Croft PR, Papageorgiou AC, Jayson MI, Macfarlane GJ. Predicting who develops chronic low back pain in primary care: a prospective study. BMJ 1999; 318:1662–7.
- Hollinghurst S,sharpD,BallardK,et alRandomized controlled trial of Alexander technique lessons, exercise,and massage(ATEAM)for chronic and recurrent back pain: economic evaluation http://www.bmj.com/cgi/content/full/337/dec11_2/a2656).BMJ 2008;337:a2656.doi:10.1136/bmj. a2656.PMID 19074232.
- Sarno, John E. Healing Back Pain: The Mind-Body Connection. Grand Central Publishing: Warner- Books; 1991.
- Ebadi S, Ansari NN, Henschke N, Naghdi S, Tulder MW. The effect of continuous ultrasound on chronic low back pain: protocol of a randomized controlled trial. BMC Musculoskeletal Disorders 2011; 12:59.
- DA Hurley1 Physiotherapy for sleep disturbance in chronic low back pain:preliminary results of a feasibility randomised controlled trial.J Bone Joint Surg Br, 2012;94:1.