
ABSTRACT
BACKGROUND
Ankle sprain is one of the most frequent musculoskeletal injuries affecting all age groups. Exercises play an important role to improve joint proprioception and coordination after ankle sprain but the efficacy is still unknown. A systematic review in accordance with PRISMA was performed to evaluate the effects of proprioception rehabilitation for ankle sprains.
METHODS
Thirteen articles and one review were searched up to March 2012. Randomized controlled trials of ankle sprain were included while postural sway index and pain were the reported outcomes. An analysis was performed based on intervention type, grade of sprain, and control group. Moreover, a sensitivity analysis was also conducted with respect to risk of bias, sample size, and result reported.
RESULTS
1020 participants included in the review reported marked improvement when compared with other interventions. Risk Ratio (RR) <01, CI 95% was considered low risk of bias. The studies included showed low risk of bias but the benefit of proprioceptive rehabilitation remained significant. Results also revealed proprioception as an add-on treatment also improved global symptoms as compared to primary group alone. It was noticed that no study shown adverse effect.
CONCLUSIONS
Rehabilitation for proprioception is equally effective in improving static and dynamic balance in ankle sprain as a primary intervention and add-on.
Key Words
Ankle Sprain, Proprioception, Static and Dynamic Balance Training, Taping, RCT, Systemic Review.
Erum Naz
Senior Lecturer
Ziauddin College of Physical Therapy
Muhammad Sarfraz
Assistant Professor
Ziauddin College of Physical Therapy
Sana Ambreen
Physiotherapist
Chiniot General Hospital
Navaid-us-Saba
Senior Lecturer
Ziauddin College of
Physical Therapy
[Naz E, Sarfraz M, Ambreen S, Navaid-us-Saba. Effect of Proprioception Rehabilitation in Ankle Sprain: Systemic Review. Pak. j. rehabil. 2012;1(2):3-10]
INTRODUCTION
Ankle sprain is the frequent encountered musculoskeletal injury among people either having sedentary life style or related to sports. The sounds of pop are being heard and feel of give way, difficulty in standing is an active complain in ankle sprain. Among soft tissue injuries ligamentous injury is one of the common problems came across for the treatment purpose to physician and physiotherapist. Beynnon BD et al. Estimated prevalence of first-time ankle sprain as one/10,000 individual affected daily, ten to twenty percent ankle injuries report among all sports injuries and 2 million injuries per year accounted1-3. In Addition, 85% of ankle injury originate from weaker lateral ligament and 3-5 % are medial (deltoid) collateral ligament4,5. According to severity of injury ankle sprain divided into three grades. Grade –l is mild (some damage to fiber of ligament or mild stretching), grade ll is moderate sprain (partial tear and abnormal loosen of ankle joint) and grade lll is severe strain (complete tear of ligament)6.
There are three major type of treatment available to treat ankle sprain according to severity conservative, functional, and surgical, on the other hand, conventional treatment, complementary and alternative therapy (such as physical therapy, electrotherapy, herbal medicine, homeopathy and acupuncture) are available to treat ankle sprain10-12. In conservative management plaster cast immobilization and external support (elastic bandage, tapping, and orthotic support) are in practice 7. Deep heating agent like therapeutic ultrasound and short-wave diathermy are also commonly used, but there is little proof to promote their use in terms of symptom relief 7,8. However, physical therapy have vast scoop to treat ankle sprain grade l,ll.Post surgical rehabilitation to functional training. Patient with grade l or grade ll sprain PRICE is the choice of treatment initially then progress to exercise, mobilization, proprioceptive training, balance training ultimately aim is to restore the pre functional level 7-14.
Clinical experiences and some studies showed that proprioceptive intervention is effective in treating ankle sprain. However, the supportive evidence of proprioceptive rehabilitation as a choice of treatment in ankle sprain to return to pre-injury level is still unclear. We decided to critically evaluate the evidence.
METHODOLOGY
- Eligibility Criteria
a) Types of study
Randomized controlled trials (RCTs) evaluating effect of proprioceptive rehabilitation in ankle sprain were considered.
b) Types of participant
Following are Inclusion criteria of this systemic review,
- Mixed population studies including adults and children were included
- Patients who reported an ankle sprain regardless of duration also included
- The diagnosis could be based on any method, including physical examination for edema drawer test ligament stress test and ancillary procedure like radiograph of the injured ankle.
c) Types of intervention
i.Types of control
For control groups, we considered non placebo, cryotherapy, taping, acupuncture, exercises, functional rehabilitation, normal daily activities, orthosis, static balance training, and no intervention. Proprioceptive rehabilitation was given with other treatment; we considered only those trials where identical comparative treatment was administered to the proprioceptive and control groups.
ii. Types of outcome measure
The primary outcome of this systematic review was proprioception improvement at the end of treatment. Postural sway data were included in the review if data of postural were not available. Secondary outcomes included pain intensity or time to achieve pre-injury level of work or sports, subjective (e.g., giving way) and objective (e.g., inversion stress test, talar tilt, anterior drawer test, postural sway analysis) evaluations of ankle sprain/ instability, dichotomous (e.g., yes or no) and continuous data regarding swelling, recurrence of ankle sprain, subsequent surgery, or long-term treatment and adverse events related to proprioceptive treatment.
- Literature Search
We searched the following databases from their initiation 10 march 2012. Controlled Trials, Pub Med, article journal of Orthopedic and Sport Therapy, Sports Med, Knee Surgery, Sports Traumatology, Arthroscopy , article from group bmj.com, article from Journal of Athletic Training, BMC Musculoskeletal Disorders, Med. Sci. Sports Exerc, Archives of Emergency Medicine, Journal of American physical therapy association, journal of bone and joint surgery, J Chiropr Med, Journal of Manipulative and Physiological Therapeutics, Journal of Physiotherapy, Clinical Journal of Sport Medicine. Trail publish in English were sought6.
- Study Selection and Data Extraction
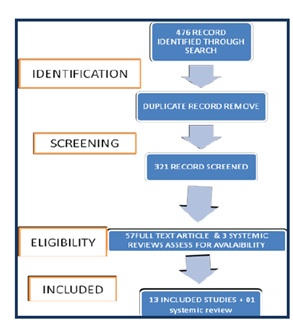
Our electronic search resulted in 57 article and three systemic reviews potentially relevant articles. Reviewers independently searched articles to evaluate for the suitability of the inclusion criteria. If there was a disagreement, it was resolved by discussion between the reviewers; after reviewing titles and abstracts 57 potentially relevant articles were selected. However, 16 full text articles fulfill our inclusion criteria. A further three relevant articles were rejected after checking the reference lists of included studies. Hence a total of 13 articles were included in this review.
- Risk of Bias Assessment
a) Assessment Tool?
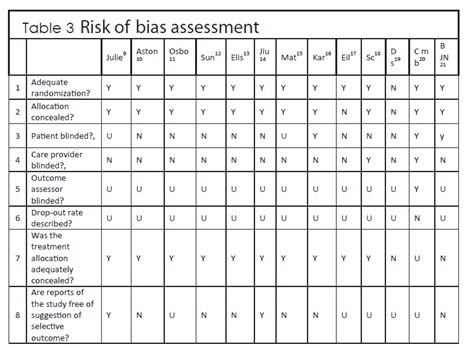
Reviewer individually analyzes the risk of bias. Eight domains were the objective and assess by the reviewer, table 3.
1.Adequate randomization?
2.Allocation concealed?
3.Patient blinded?
4.Care provider blinded?
5.Outcome assessor blinded?
6.Drop-out rate described?
7.Was the treatment allocation adequately concealed?25
8.Are reports of the study free of suggestion of selective
outcome reporting?
Yes(Y), No (N) and unclear (U) were used to give rating.
- Statistical Analysis
Studies were classified in the main analysis according to whether Proprioception intervention was a primary or an alternative or an add-on treatment. The impact of proprioception on dichotomous data was expressed as the risk ratio (RR) with the proprioception intervention compared with the control, with 95% confidence intervals (CIs)(the RR of non-response). To define non-response, symptoms in ordinal assessments were divided into two groups (e.g., ‘poor’ or ‘good’ as non-response vs. ‘very good’ or ‘excellent’ as response). RR value of less than 1 indicated a lower risk of symptoms getting worse/ persisting with proprioception compared with the control. For continuous outcomes, the mean difference (MD) with a 95% CI was calculated. Visual inspection were used to assess homogeneity among the included studies Subgroup analyses were conducted in terms of proprioception intervention, grades, and control type.
Sensitivity analyses were also planned by including only those studies with low risk of bias or studies with sample size ≥40 per division, and by varying the grouping of outcome measures. We analyzed studies with a low risk of bias for randomization and/or allocation concealment only and investigated whether the intervention was affected. For outcome measure report based on an ordinal assessment (e.g., poor, good, very good, excellent), we also performed a sensitivity analysis by reanalyzing the dichotomous outcomes; we compared the ‘excellent, very good vs. good, poor’ scenario from our original analysis with an ‘excellent, (very) good vs. poor’ scenario to differentiate any inconsistence.
RESULTS
- Description of Studies
475 articles and 3 systemic reviews were searched on electronic media, out of which 321 were withdrawn on the basis of study topics and after reading abstracts. 21 articles were not focusing on the topic and rest of the 42 articles was not randomized control trial or clinical trial. On the basis of not fulfilling our inclusion criteria 44 more articles were also excluded. Our search terms give in 13 records of article and one systemic review. Four in the journal of orthopedic and sport therapy, five in sports Med, four in Rehabilitation and Sports Medicine. Twelve in Pub Med, five in American physical therapy association, one in journal of bone and joint surgery, one J Chiropr Med, one in Journal of Manipulative and Physiological Therapeutics, one in journal of physiotherapy, Four in clinical journal of sport medicine. After removal of duplicate studies 42 records were excluded, however, studies that compare the effect of proprioception on ankle rehabilitation as a control group(n=1) or as a co-intervention(n=3) or trails compare proprioception with other rehabilitation procedure(n=09) were studied. One systemic review related to topic was also included. Figure -1 shows a flow chart of literature search according to guideline of PRISMA23.
- Characteristics of the Included Studies
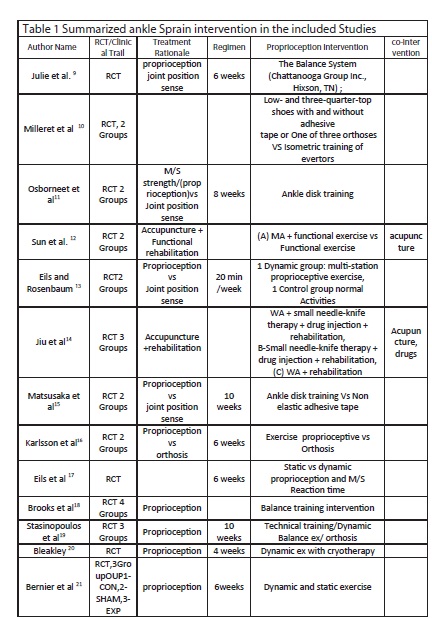
All details regarding including studies are summarized in table-1 and 2
a) Participants 1020 ankle sprain participant enrolled in this review.
Studies is taken from different countries. According to grade three studies clearly mention grades of ankle sprain18 and on the basis of acute and chronic sprain one12,16,20 study involves acute cases while nine remaining studies involve mixed participant. Chronic participant were not considered in any study. Adverse effect was not observed in any study.
b) Proprioceptive intervention
Varity of treatment available like Disk training, static and dynamic exercise, taping, orthosis, muscle training to improve proprioception in ankle sprain.
c) Control intervention
A verity of treatment were used in included studies taping, icing, acupuncture, orthosis, balance board exercises, static and dynamic exercises, multistation, proprioceptive exercises and technical training. Only one study adapt proprioception as control group10, two studies applied proprioception as an add on12,14. Nine trails evaluated the effect of proprioception 9,11,13,15-19,21. Furthermore, two groups were considered in four trails14,18,19,21.
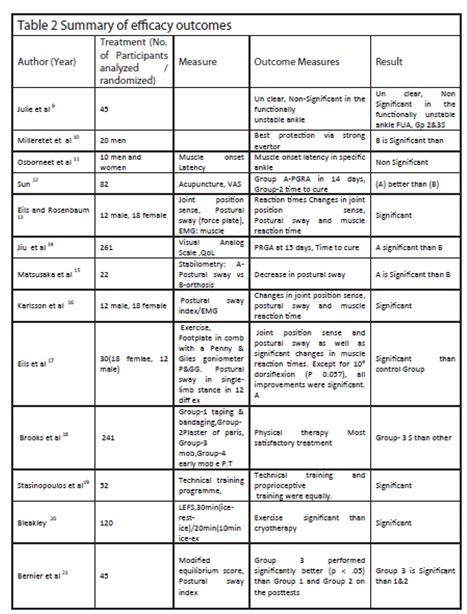
d) Outcome measure
Outcome measures described in the included studies were Postural sway, Pain scale and Pre injury level. Ten trails shown improvement in postural sway index, two trails reveal improvement in pain (PGRA) and time to return to pre-injury level of work or while one shown unclear results9. One trail showed muscle strength is better than balance exercise only one trail reported about the reoccurrence. Diversified outcomes were used to assess efficacy but significant and non-significant results were used in this review to accomplish the key analysis. See table 1 and 2.
e) Risk of bias in the included studies
The studies were evaluated on the basis of high or low risk of bias. To ensure low risk of bias the blindedness regarding physical therapist and participant were also considered in the study. There were single blinded studies, however only one study was found to be double blinded. Ten trails having low risk of bias except one study studies was not reported an adequate method of sequence of randomized control trail20. Regarding choosy outcome reporting, we could not find and compare the protocols of any of the included studies; hence, describe method is judged for risk of bias in this review. Two studies had a high risk of bias regarding free of suggestion of selective outcome (Table 3).
- a) Effects of Rehabilitation measure on Primary
Outcome
The key outcomes from the included studies are provided in Table 1. We evaluated primary outcomes according to postural sway index. Pain (VAS) was considered if postural sway was not available. Most of trials reported improvement in symptoms. Approximately three sessions/ week were given over 6 weeks to 10 weeks. Only one trail used session once/ week13. Dynamic balance training / had a statistically significant effect in reducing the postural sway /instability of ankle sprain (low risk of bias). See table1 & 2.
b) Effects of Rehabilitation Measure as an Add-on
Treatment
Two trials reported the add-on effect of proprioception12,14 and rehabilitation exercises/functional exercises. When added to other treatment, proprioception compared with the other treatment. There was no significant heterogeneity among the studies. Only one study reported recurrence of ankle sprain after treatment. 4-Effects of Rehabilitation on Secondary Outcomes
a) Time to achieve pre-injury level
One study reported that acupuncture in addition to functional exercise shortened the time to coming back to normal activity by 3-4 days compared with a functional exercise only group (5.2 ± 0.7 vs. 8.6 ± 1.4, MD –3.40, 95% CI –3.88 to –2.92.
b) Ankle instability and swelling
Most of the studies reported a composite measure of postural sway. No included study reported on ankle instability and/or edema as a separate outcome measure.
c) Recurrence of ankle sprain
One study reported that one participant in the primary intervention of proprioceptive rehabilitation had ankle instability16 and unclear risk of bias in the control group had suffered recurrent injury.
d) Adverse events
None of the study reported adverse events such as worsening of the symptoms, frost bite, allergic reaction both in primary treatment and add on treatment.
- Subgroup Analyses
Subgroup analyses conducted on the base of the following Predefined characteristics: type of proprioception intervention, grade of ankle sprain, and control type.
- Type of Intervention of Proprioception
Proprioception had an additional effect on symptoms improvement compared with add on group. Proprioception as a sole treatment had significant benefit compared with other treatment like adhesive taping, cryotherapy, orthosis, functional exercise, static balance training and acupuncture. The effect of proprioception was statistically significantly better than other groups.
a) Dynamic rehabilitation vs other rehabilitation measure
Dynamic balance and coordination training vs rehabilitation measure (functional exercises, disk training, static balance. six trials tested the effect of improvement in dynamic balance and coordination training against rehabilitation measur9,11,13,15,18,21. There was no statistically significant difference between the groups11.
b) Dynamic and static rehabilitation plus taping vs taping Proprioceptive rehab with taping had additional effect on postural sway index improvement compared with tapping only15.
c) Acupuncture plus functional exercise and rehabilitation vs. acupuncture alone Symptoms persisted in significantly fewer participants when was added to acupuncture compared with the acupuncture alone.
6. Sensitivity Analyses
Sensitivity analyses were performed by excluding studies with predefined less desirable characteristics, as follows.
a) Risk of bias
When the analysis was limited to 13 studies with a low risk of bias for random sequence generation and/or allocation concealment, the add-on effect of intervention on remain postural sway index or VAS significant and risk factor is too low. See table-3
b) Sample size
when four studies with > 50 participants per group were analyzed; there was no significant difference in the risk of symptoms persisting or worsening between the ankle proprioception improvement and control groups14,18,19,20.
c) Outcome measures
For 13 studies reporting a dichotomous outcome based on an assessment, we compared the ‘excellent, very good’ vs. ‘good, poor’ scenario the difference remained significant without variability.
DISCUSSION
Summary of Evidence
This systematic review directed to assess the evidence in support of effect of proprioceptive rehabilitation intervention for ankle sprains. One Systemic Review and thirteen RCTs were included that investigated the effect on postural sway index of proprioception intervention as an primary, an add-on to other treatment and control group. In the evaluation of proprioception interventions compared with other treatments, proprioception had a therapeutic benefit in improving postural sway in ankle sprain (RR of symptoms persisting with proprioception = 0.56, 95% CI 0.42–0.77). However, this is Probably an over emphasize due to the heterogeneity between large (> 50) and small (<40) sample size and could be high risk of bias of the included studies.
Compared with other treatments alone, proprioception significantly low risk of bias. A sensitivity analysis of the studies with a low risk for selection bias suggested that the valuable effect of proprioceptive rehabilitation was maintained. The effect of proprioceptive intervention was more significant when the analysis was not limited to studies sample size. Proprioception was equally effective as primary intervention; co intervention and control group in improving stability by retrained the participant balance and coordination. In addition, participant returns to their daily activities, but these analyses were based on only a small number of studies. Any ad versed effect was not reported by any participant.
Risk of Bias
Most of the selected studies had a low risk of bias for adequate randomization and allocation concealment. One study had a high risk of bias for adequate randomization and allocation concealment. It is clear that inadequate allocation concealment/random sequence generation leads to overestimation of treatment effects. Although the included studies uniformly reported no difference in baseline characteristics between groups, we cannot exclude the possibility that selection bias may have played a role. However, when we limited our main analysis to those studies rated as having a low risk of bias for randomization/allocation concealment, the benefit of intervention remained significant.
Selected studies may have been more likely with positive outcomes measure, but the sample size of the study in this review may have been adequate effect on methodology design and conduct. Because it is well known that high-quality studies tend to inflate the effect of an intervention.
Limitations of this Review
All relevant trails and systemic review assessable on electronic media were searched only in English. The included trials were mostly of good quality; thus, the reported data are not be overestimated. In addition, the sample size of the studies may have resulted in heterogeneity of the effect size22. Reported in a model study that at least 40 participants per division are required to obtain clinically relevant results in trials relating to pain. Our sensitivity analysis based on samples size (i.e., trials with 40 ≥ per group only found significant benefit from proprioception intervention.
Finally, most of the studies in our review used various subjective outcomes. Study result may have influenced by failure of blind outcome assessment. Implications for Practice This systematic review suggests that there is insufficient high-quality evidence supporting the use of rehabilitation intervention for proprioception improvement as an alternative and co-intervention. Rehabilitation to recover proprioception provided a significant benefit as a primary intervention and a sensitivity analysis of high quality. In this review proprioception as an add on treatment improve symptom markedly, another outcome measure reveal that data was sufficient on the maximally have clinical importance relating to ankle sprain. In summary, evidence supporting the use of intervention either dynamic or static, supporting aids in patients with ankle sprain is currently conclusive.
Implications for Research
To obtain a more definitive result to the question of the efficacy of proprioception intervention for ankle sprain, a careful conducted trial was designed to evaluate the recurrence of ankle sprain after proprioception rehabilitation. Researchers should use proprioception training verses orthosis. Regarding the blindness of the trails, most of the trails were not mention either the trail is blinded, single blinded or double blinded. Only one study showed double blinded adequately. There was no study with sham control in this review, so performance bias may have present in this study, so Sham-controlled trial is needed to avoid performance bias in future. To maintain outcome assessor Blinding, validated assessment tools are required to judge the outcome assessor. Recent studies has not tested the validity and responsiveness of the ankle functional score (AFS) based on fundamental functional outcomes such as pain, edema, and gait. In addition, AFS is easy to evaluate recovery after acute ankle sprain and should be use as a outcome measure in future. Available evidence is sufficient to recommend dynamic proprioception exercise as an evidence-based treatment option for ankle sprain. Furthermore, Proprioception exercises as an add on measure should be practice. Further well-designed and conducted trials are needed to draw a definitive conclusion.
REFERENCE
- Beynnon BD, Renstrom PA, Haugh L, Uh BS, Barker H. A prospective, randomized clinical investigation of the treatment of first-time ankle sprains. Amn J Sports Med 2006;34(9):1401–1412.
- Mascaro TB, Swanson LE. Rehabilitation of the foot and ankle. Orthop Clin North Am 1994;25:147–60
- Beynnon BD, Renstrom PA, Alosa DM, Baumhauer JF, Vacek PM. Ankle ligament injury risk factors: a prospective study of college athletes. J Orthop Res 2001;19(2):213–220.
- Nyanzi CS, Langridge J, Heyworth JRC, et al. Randomized controlled study of ultrasound therapy in the management of acute lateral ligament sprains of the ankle joint. Clin Rehabil 1999;13:16–22.
- Lofvenberg R, Karrholm J. The influence of an ankle orthosis on the talar and calcaneal motions in chronic lateral instability of the ankle. Am J Sports Med 1993;2:224–30.
- Egger M, Jüni P, Bartlett C, Holenstein F, Sterne J. How important are comprehensive literature searches and the assessment of trial quality in systematic reviews? Empirical study. Health Technol Assess 2003;7(1):1–76.
- Ogilvie-Harris DJ, Gilbart M: Treatment modalities for soft tissue injuries of the ankle: a critical review. Clin J Sport Med 1995;5(3):175–186.
- Bekerom MP, Windt DA, Ter G, Heijden GJ, Bouter LM: Therapeutic ultrasound for acute ankle sprains. Cochrane Database Syst Rev 2011; 6:CD001250.
- Bernier JN, Perrin DH. Effect of coordination training on proprioception of the functionally unstable ankle. J Orthop Sports Phys Ther. 1998;27(4):264-75.
- Ashton-Miller JA, Ottaviani RA, Hutchinson Ch, et al. What best protects the inverted weightbearing ankle against further inversion. Am J Sports Med 1996;24:800–9.
- Osborne MD, Chou LS, Laskowski ER, et al. The effect of ankle disk training on muscle reaction time in subjects with a history of ankle sprain. Am J Sports Med 2001;29:627-32.
- Sun C, Ju YY: Evaluation on the effect of acupuncture in the acute ankle sprain induced by football [in Chinese]. Mod Prev Med 2011; 38(10):1890–1891
- Eils E, Rosenbaum D. A multi-station proprioceptive exercise program in patients with ankle instability. Med Sci Sports Exerc 2001;33:1991–8.
- Jiu ZZ. Observation on therapeutic effect of acupuncture at Yanglingquan (GB 34) on sprain of external ankle joint [in Chinese].Zhongguo Zhen Jiu 2006; 26(8):569–57
- Matsusaka N, Yokoyama S, Tsurusaki T, et al. Effect of ankle disk training combined with tactile stimulation to the leg and foot on functional instability of the ankle. Am J Sports Med 2001;29:25–30.
- Karlsson J, Andreasson GO. The effect of external ankle support in chronic lateral ankle joint instability. Am J Sports Med 1992;20:257–61.
- Eils E and Rosenbaum E. A multi-station proprioceptive exercise program in patients with ankle. Sci. Sports Exerc 2001;33(12):1991–98.
- Brooks SC, Potter PT, Rainey JB. Treatment for partial tears of the lateral ligament of the ankle: a prospective trial Bmj 1981;282(6264):606-07.
- Stasinopoulos D. Comparison of three preventive methods in order to reduce the incidence of ankle inversion sprains among female volleyball players. fbjsm.bmj2013.
- Bleaklay CM. The PRICE study (Protection Rest Ice Compression Elevation): design of a randomised controlled trial comparing standard versus cryokinetic ice applications in the management of acute ankle sprain . BMC Musculoskeletal Disorders 2007; 8:125
- Bernier JN & Perrin, D.H. Effect of coordination training on proprioception of the functionally unstable ankle. JOSPT 1998;27:264-
- Moore RA, Gavaghan D, Tramèr MR, Collins SL, McQuay HJ: Size is everything–large amounts of information are needed to overcome random effects in estimating direction and magnitude of treatment effects. Pain 1998;78(3):209–216.
- Moher D, Liberati A, Tetzlaff J, Altman DG: Preferred reporting items for systematic reviews and metaanalyses: the PRISMA statement. Ann Intern Med 2009;151(4):264–269. W264
- Zöch C, Fialka-Moser V, Quittan M.Rehabilitation of ligamentous ankle injuries: a review of recent studies, Br J Sports Med 2003;37:291–295.
- Pildal J, Hróbjartsson A, Jørgensen KJ, Hilden J, Altman DG, Gøtzsche PC:Impact of allocation concealment on conclusions drawn from metaanalyses of randomized trials. Int J Epidemiol 2007;36(4):847–857.