
ABSTRACT
The age-old understanding that an individual with a hearing loss is incapable of acquiring verbal communication skills was readily accepted in the past, which led to the inadvertent but unfortunate coining of phrases “deaf and dumb” or “deaf and mute, ” and the development of non-verbal or manual communication methodolgies of Sign language. Further, this caused the segregation and isolation of otherwise physically and intellectually competent individuals from mainstream society, unjustifiably denying them opportunities of education and vocation. Studies have proved that in the absence of any organic or inorganic complication, a child with a hearing loss may not only score a high Intelligence Quotient but can also acquire more than one language fluently.
Early Intervention with appropriate amplification of residual hearing is underscored as the fundamental prerequisite for children with bilateral congenital profound sensorineural hearing loss, for subsequent acquisition of good listening and normal speech-language skills and plausible bilingualism; that further equips them with scholastic achievements comparable to their hearing peers. The past half century has witnessed stupendous technological enhancements in amplification devices manufactured for children having hearing loss, complemented by steady success in fostering their Inclusive Education. This paper highlights the urgent need in Pakistan to address this issue as well as the importance of early detection, diagnosis, and (re)habilitation along with parent training initiated within the first year of life.
An otherwise anticipated disabling condition may be overcome completely if neonatal screening, which is not only inexpensive but also easy to perform; is made mandatory at all hospitals and maternity homes, as practiced in the developed world. This shall ease the challenges faced by the families of children having hearing loss; and enable the professionals working with them to successfully alleviate their communicative, social, educational and vocational difficulties, and ensure that they become successfully contributing members of our verbal society.
Key Words
Bilingualism, Children, Congenital, Bilateral Sensorineural, Hearing Loss, Pakistan
Amina Asif Siddiqui
Principal
Ziauddin College of Speech
Language And Hearing sciences (ZCLHS)
Ziauddin University
[Siddiqui AA. Bilingualism in children having Congenital Bilateral Profound Sensorineural Hearing Loss
– Case Review. Pak. j. rehabil. 2012; 1(2):11-16]
INTRODUCTION
The World Health Organization figures in 2002 stated that about 250 million people in the world have disabling hearing impairment (moderate or worse hearing impairment in the better ear)1. A number of children present with mild to moderate degree (25db to 55dB) of conductive of hearing impairment caused by a pathology in the outer or middle ear; which although treatable and most often a reversible condition often goes unnoticed2. When hearing loss involves the inner and outer hair cells or the auditory nerve it is known as sensorineural hearing impairment and is irreversible3. Moderate to severe hearing loss markedly affects the normal acquisition and development of speech and language skills and consequently restricts the individual’s social, educational and vocational progress4.
Pakistan, a predominantly bilingual society, has over 180 million people (Pakistan Bureau of Statistics 2011) with more than half of them in the small towns and villages5. Most people in rural Pakistan are exposed only to their native language and Urdu sometimes, whilst those in the cities are exposed to English additionally. Researchers studying Language and Language Acquisition in human babies, have spoken more than often about the role of parents and family or caregivers in fostering the development of verbal communication skills in little children6. Research has proved that the language used at home, referred to as mother tongue, is acquired best by the human baby, in the first 3 years of life when the brain is most plastic and malleable (Hoff 2005)5. However, can we apply this rule indiscriminately when talking about children with congenital hearing impairment? In the absence of multiple disabilities these children have a speech mechanism that is completely normal in structure and function, they are intelligent and have normal neurological functioning necessary for speech and language development, but are deprived of the main input for language growth through the channel of hearing (Arnold 1982)7.
This case review is aimed at defining the development of verbal communication skills of children with hearing impairment, in a predominantly bilingual society, and the necessary measures that ensure optimal social integration and a successful academic career for them.
Hearing Impairment in Pakistan
Pakistan is a third world country struggling to establish immunization programs and reduce maternal death. Prevalence of repeated consanguineous marriages over the generations in families is a prominent cause of congenital hearing impairment (also known as pre-lingual hearing loss) and other congenital problems8. Malnutrition and lack of education lead to poor prenatal, natal and post-natal care9. Rampant infections due to unhygienic conditions as well as impoverished medical intervention are often the cause of complicated pregnancies and premature deliveries10.
There is no law enforced in Pakistan for mandatory hearing screening of new born babies at medical facilities, whilst only a handful of the medical institutions in the public or private sector have initiated this, as a result of which congenital hearing impairment of the sensorineural type is most often not detected till the family begins to worry about the child not communicating verbally. Conductive hearing impairment, which may be a fluctuating hearing loss, is often not detected either, with the child being labeled as inattentive, naughty, or weak in studies, and worse still may be misdiagnosed as developmentally or intellectually challenged 8,11,12.
It is estimated that two out of three of the words hearing-impaired are in developing countries (Rai 2004)13. Recessively inherited deafness in the Pakistani population is higher 1.6 per 1000 individuals due to high consanguinity13, whilst the world average is 1 per 1000 individuals (Hussain and Bittles, 1998)14. Approximately 2% of children in Pakistan present with prelingual severe to profound hearing impairment of the sensorineural type.
Language Acquisition and Critical Period Hypothesis
The Speech Chain (Varley 1991) describes the sense of hearing as the primary source of receiving verbal information15. Listening is when the person pays attention to information received auditorily; and whence the brain decodes that information it is known as auditory processing 12,16. The human foetus is receptive to sounds from the 24th week of gestation, hence it is no surprise that the baby is soothed by his/her mothers voice soon after birth17. The development of listening skills progresses from a mere awareness of sounds to their recognition and understanding of speech and language. The first year is critical for the completion of auditory maturation (Northern and Downs 2003)18. Birth through puberty is known as the Critical Period in the child’s life, as it is the period of maximal neurological growth both anatomically and physiologically (Myelination continues till puberty – Crystal 1998)16, this along with environmental stimulation contributes to intense intellectual, cognitive, speech and language development. Furthermore, the first three years of life are the most crucial period as we see the human baby achieve his major motor milestones, accomplish auditory maturation and speak the first meaningful word around the first birthday, which rapidly evolves to phrases and sentences by the age of three years19. Noam Chomsky hypothesizes the ‘Language Acquisition Device’ in the baby’s brain that generates the rules of grammar of any language, and is actively engaged in doing so till puberty, thus establishing our innate ability to acquire language skills.
Consequence of Bilingualism / Multilingualism in the world on deaf population today
Most societies in the world today are bilingual; stretching from China in the far-east across Central Asia and Africa to Canada and Portugal in the west. It is estimated that two third of the children in the world’s population grow up in bilingual environments (Crystal)14. The natives of most countries communicate in the dominant language, whilst English is either the second language or the additional language spoken by them. The migration of inhabitants from third world countries to the developed world, seeking better education and a brighter future has vigorously led to this phenomenon20. Research has proved that not only do bilingual individuals super cede monolinguals over metalinguistic skills, but also have better cognitive skills as a result of which they have more vocational opportunities. Ironically, we need to question strategies and methodologies in aural re/habilitation, as it is a rule to be using just one language with children having hearing impairment, which must be their native language! How then, can we educate them in a country like Pakistan where schools for mainstreaming these children have English as their medium of instruction predominantly?
Mammoth technological advances in amplification devices that have greatly contributed to improved listening skills in children with hearing impairment, now warrant a complementary change in communication methodologies as well21. Early Intervention is underscored as the fundamental prerequisite for the acquisition of good listening skills leading to normal speech and language skills in children with bilateral congenital profound sensorineural hearing loss22,23. Schools in local languages are seldom found, and ‘Urdu medium’ schools are few and far between, ‘English medium’ schools are the best option for most Pakistani families; it becomes crucially important to determine the factors conducive to acquiring or learning two languages i.e. ‘bilingualism’ in children with hearing impairment; for them to successfully enroll into ‘Inclusive education programs’.
Educating Children with Hearing Impairment in Pakistan
Statistics show 58% (2009) literacy in Pakistan (Federal Ministry of Education, provisional Education Ministries)24. The government spends a negligible 2.2% (2007) of its annual budget in this realm, causing the obvious neglect of primary and secondary education in mainstream schools. The idea of ‘special education’ is entrenched in Pakistani society that unjustly discriminates and segregates all individuals that are in any way different from the so called ‘normal’ population, cruelly labeling them as ‘disabled’ or abnormal’.
On the other hand, madrasahs are located near around mosques and impart religious education fused with worldly knowledge at a nominal cost or for free, while the government schools where the medium of instruction is invariably Urdu, are run on a nominal tuition fee, but are severely impoverished in terms of qualified teachers and basic infrastructure. Educational institutions where the medium of instruction is English, are considered superior to those schools where the medium of instruction is Urdu, whilst schools having a regional language of instruction fall in the lowest rungs of hierarchy.
The private sector has invested heavily in this area, and undeniably shoulders the responsibility of educating the 63% of youth in Pakistan from pre-primary to post graduate levels, running English medium schools and making education an expensive yet buyable commodity for the middle, upper middle and upper strata of society, but the lower socioeconomic stratum remains deprived; relying on madrasahs or the government schools. It is the Private sector that has introduced Inclusive Education, wherein most schools are mainstreaming children that are differently-abled with their peers. This is an expensive affair, as the schools also make the parents bear the cost of an individualized teacher’s aide who works on a one-to-one basis with their child, within the classroom. Since most teachers are untrained and ignorant about hearing impairment and its management in mainstream schools, the speech language therapists at the Ziauddin College of Speech Language Therapy have undertaken the task of a Teacher Training Program on management of hearing impairment and other speech language disorders in mainstream schools of Karachi.
CASE REVIEW
Case Review of baby MA having bilateral profound
sensorineural hearing loss, who received early intervention.
Introduction
Baby MA was fitted with binaural hearing aids at 8 months of age and was given a cochlear implant in one ear at 18 months of age. Now 2; 10 years of age he has well established verbal communication skills, with a Mean Length of Utterance (MLU) of 1.5 – 2.0.
Baby MA is the first baby of non-consanguineous parents. His mother had an uneventful pregnancy and a normal full-term delivery. The baby had an immediate birth cry, a birth weight of 2.5 kilograms and an Apgar score of 10. MA was nursed by his mother, and was discharged from hospital on the third day after birth. He was usually very manageable, and appeared to be achieving his milestones age appropriately, he was weaned at 4 months of age. At 5 months of age the grandfather voiced his concern that the baby had not responded to a loud environmental sound. MA’s behavior was thence scrutinized for his responses to all sounds around him. The family observed that he was not startling to loud sounds such as banging the door or to loud clapping. He was not turning or looking towards sounds around him such as the door bell, the ringing of the mobile phone. He was definitely not aware of his name.
MA was promptly taken to an Otorhinolaryngologist who examined him, and advised a complete audiological evaluation to rule out a suspected hearing loss. The Visual Response Audiometry in sound field revealed a ‘no response’ to all frequencies at 110db.The Brainstem Evoked Response Audiogram showed no responses to the click stimulus at 110dB in both ears. MA was diagnosed as having a bilateral congenital profound sensorineural hearing loss.
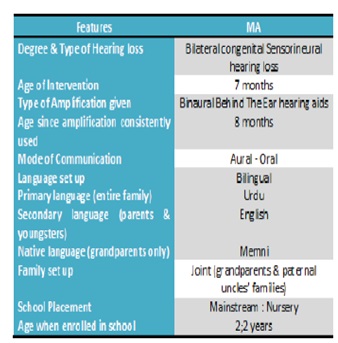
Table 1: Features of Lingual status and Aural Habilitation of MA
Development of MA’s Listening & Speech-Language Skills
MA has been wearing his hearing aids since the age of 8 months regularly and consistently. He was exposed to English by his parents and grandfather; whilst the rest of the family spoke Urdu around him. He developed awareness to environmental sounds and speech within a month and would startle and cry on loud sounds. By the age of 10 months, he was producing reduplicated babbling. Soon after his first birthday he had well established variegated babbling, he was responding to his name when called and recognized the voice of his grandfather, was imitating motor speech play behaviors such as ‘peek a boo’, and the sound of the aero plane. MA spoke his first meaning full word at the age of 18 months by calling out to his mother by the word “mama.” Present Status of Listening & Speech-Language skills: MA uses stereotyped utterances in Urdu and English as well as generates his own spontaneous utterances in both languages spontaneously. He follows single stage routine and non-routine instructions with ease. His receptive and expressive language skills have developed very well for verbal language. He has about 200-250 words in his receptive-expressive repertoire. He has a rapidly developing lexicon for nominals, action words, describing words, and position words. He understands and uses concepts of possession, quantity and negation (refusal and absence) correctly.
Parental involvement
MA has tremendous support from his family. His parents and grandparents and maternal and paternal aunts and uncles are all very supportive in providing language stimulation. His mother is the most active in transfer and carryover of all tasks taught in therapy.
CONCLUSION
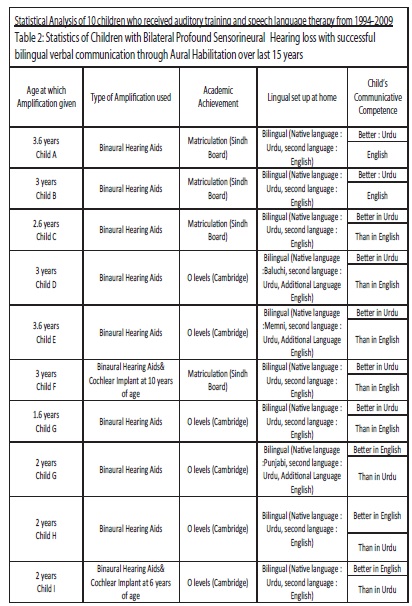
In table 2, it is evident that all the children with hearing impairment came from bilingual homes, where English and Urdu were spoken simultaneously. The children were enrolled in two different systems of school education the Cambridge system of ‘O’ levels, which places more demand on the student as it involves more analytical thinking than rote learning, as seen in Matriculation. 6 of the children were given amplification between 2.6 and 3.6 years whilst 4 of them received amplification between 1.8 years – 2 years.
The children who received amplification after 2.6 years not only had difficulty mastering communicative competence in English, but were also slightly more challenged scholastically as 4 out of them progressed to obtain their matriculation, whilst only 2 of them did the O – levels. On the other hand, the remaining 4 children achieved better communicative competence in English than in Urdu and progressed to complete their O levels.
We can thus conclude that languages are best acquired if the child receives amplification before the age of 3 years, as 0-3 years is the critical age for language acquisition, after which the child’s capacity to acquire a language naturally because of his innate biological predisposition is maximum in this period. The role of nurture in teaching the language gives best results complementing nature during the first 3 years of life, however language can be nurtured till puberty, after which the capacity to acquire it is known to diminish (critical age hypothesis, Lenneberg 1967)25.
RECOMMENDATION
It is recommended that all new born babies and high-risk babies be screened mandatorily for hearing impairment within the first few days. Those suspected of hearing loss must be further tested so that appropriate amplification is provided within the first year of life, facilitating the age-appropriate maturation of auditory skills, and speech language skills. These children shall then be able to acquire more than a single language and reap the benefits of bilingualism, cognitive skills, better concept formation and more creativity skills (Rod Ellis). Dr. Ziauddin Hospital is to commence hearing screening of new born babies through Otoacoustic Emission test in December 2012. Hearing aids and cochlear implants cost exorbitantly and must be made available through banks and leasing companies on easy installments. Amplification devices may not be afforde d by most families in Pakistan, because of the high cost. Donor agencies and philanthropists must together ensure that amplification devices are funded for the children.
REFERENCE
- The World Health Report 2002: Reducing Risks, Promoting Healthy Life. World Health Organization (accessed online): www.who.int/entity/whr/2002/ Overview_E.pdf by Life – 2002
- Musani MA, Khan FA, Rauf A, Ahsan M. Frequency and causes of hearing impairment in tertiary care centre. JPMA 2011;61:141.
- Bernstein DK, Tiegerman E. Language and communication disorders in children: Macmillan Publishing company;1993
- Elahi MM, Elahi F, Elahi A, Elahi SB. Paediatric hearing loss in rural Pakistan, Journal of Otolaryngology 1998 dec;27(6):348-53
- Gleason JB, Ratner NB. Psycholinguistics 2nd Edition: Singapore Wadsworth, Thomson Learning;1998
- Hoff E, Language Development. 3rd edition.Belmont: Wadsworth, Thomson learning; 2005
- Riaz A, Iqbal M. Non-syndromic autosomal recessive deafness in Pakistani population: Epidemiology and genetics. Pakistan J Zool 2012;44(6):1431-1438
- Gleason JB, Ratner NB. The development of language. Allyn and Bacon;2009
- How-To Guide: Inclusive Education for Children with Disabilities. Vietnam:Catholic Relief Services;2007
- http://www.crsprogramquality.org/storage/pubs/e ducation/edhowto_vietnam.pdf Rai S, Puliyel JM. Screening for auditory impairment in resource-poor countries, Journal of postgraduate medicine 2004;50(3);178-179
- Katz J, handbook of clinical audiology: Williams and Wilkins;1994
- A dictionary of linguistics and phoenix 3rdEdnOxford: Blackwell;1991
- Dyson A, Farrell P, Polat F,Hutcheson G.Inclusion and pupil achievement. Califoria State University Northridgehttp://www.csun.edu/ncod/programs/n codbooks.html
- Crystal Varley.Introduction to language development: Whurr publishers, London, jersey;1991
- Foreman P. Integration and inclusion in action: Thomson;2001,
- Fetal development: what does baby really hear in utero? : http://www.pregnancyandbaby.com/ pregnancy/articles/945349/fetal-developmentwhat- does-baby-really-hear-in utero.
- Northern JI,Down’s MP.Hearing in children. William and Wilkins; 1978,
- List of languages by number of native speakers http://www.babylon.com/definition/List%20of%20la nguages%20by%20number%20of%20native%20spe akers/:
- Clavert DR, Silverman SR, Speech and deafness, Alexander Graham Bell Association of the deaf;1983.
- Early intervention and language development in children who are deaf and hard of hearing; pediatrics 2000;106(3):43.
- Ross M. Hearing impaired children in the mainstream, York Press. 1990
- June M,Lee J, Scott.Enhancing communication skills of deaf and heard of hearing children in the mainstream; Wadsworth Thomson learning:2006.
- Economic survey of Pakistan 2007-08 http://www.khyberpakhtunkhwa.gov.pk/departm ents/bos/nwfpdev-statis-stat-abs-population.php
- Silverman FH.Speech language pathology and audiology- an introduction: Charles e Merrill publishing; 1984
- Lenneberg E. Biological foundations of language, New York:Wiley;1967