
ABSTRACT
OBJECTIVE
To compare the effectiveness of low and high frequency ultrasound (US) technique for treatment of osteoarthritis (OA) of knee joint.
STUDY DESIGN
It is a pre-post design was used with multiple treatment therapies (A and B).
STUDY SETTINGS & PARTICIPANTS
The study was conducted on the 310 patients. The patients were diagnosed knee OA by the orthopedic doctor and recommended to the Physiotherapy department of North and Clifton Campus of Ziauddin Hospital. In this study 310 patients were divided into two groups. Group A of 155 patients received low frequency US treatment of 0.01MHz frequency for 10 min and at the same time Group B of 155 patients received high frequency US treatment of 1MHz for about 3 min. Both the groups had 6 sessions in 3 weeks.
RESULT
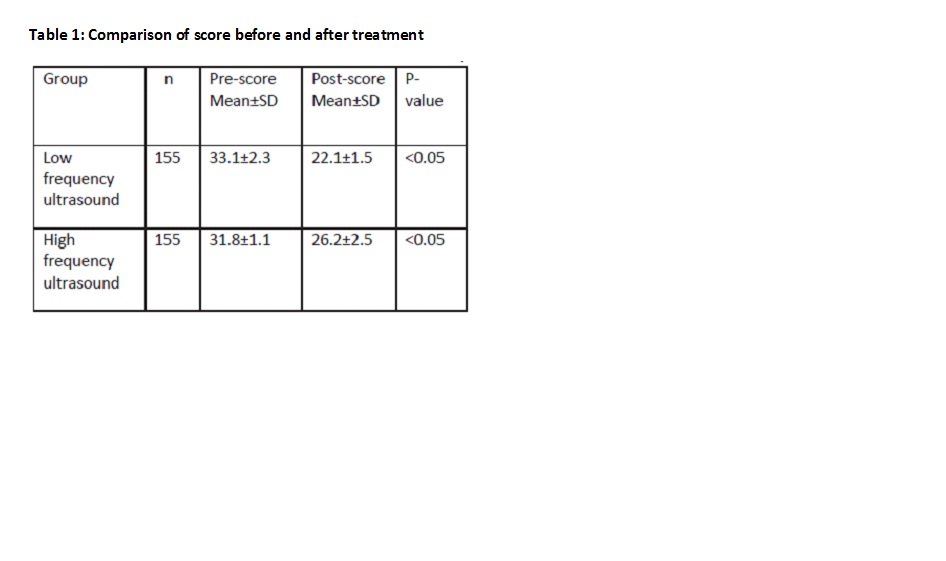
There was a mean reduction in the pain and disability with difference of low frequency US and high frequency US pre score and post score treatments of both the groups is 1.2± 0.3 and 4.1± 1.0, there was statistically significant difference between the effects of low frequency US and high frequency US in pain management of knee O.A (P < 0.05).
CONCLUSION
There was difference between the effectiveness of low frequency US and high frequency US in the pain management of knee OA
Key Words
Low Frequency US, High Frequency US, Ultrasound, Osteoarthritis, Pain, Knee.
Syeda Amool Sakeena Rizvi
Lecturer
Ziauddin College of Physical Therapy
Syed Abid Mehdi Kazmi
Manager
Department of Physical Therapy
Ziauddin Hospital
Sumaira Imran Farooqi
Principal
Ziauddin College of Physical Therapy
Jharna Devi
Senior Physiotherapist
Ziauddin Hospital
Samreen Iqbal
Senior Physiotherapist
Ziauddin Hospital
[Rizvi SAS, Kazmi SAM, Farooqi SI, Devi J, Iqbal S. Effects of Low Frequency Ultrasound compare with High Frequency Ultrasound in Knee Osteoarthritis. Pak. j. rehabil. 2012;1(1):9-12]
INTRODUCTION
Osteoarthritis is by far most common form of arthritis. It is strongly associated with aging and is the major cause of pain and disability in people. Osteoarthritis is an age-related condition, occurring more frequently in males as compare to females1. Pathologically it is defined as condition of synovial joint characterized by focal loss of hyaline cartilage with proliferation of new bone and remolding of joint contour2. The knees, hands, hips, spine, and feet include the joints most often affected by OA3,4. OA prevalence, effect on health and economics consequences are expected to increase dramatically during the next few decades as the population ages5. The prevalence of OA with age is about 40-65 years of people 80% of people have radiographic evidence of OA, through only 25-30% are symptomatic. The main clinical symptoms related by patients with knee OA include pain, stiffness, edema, deformities, instability, decrease in range of motion (ROM), physical activity limitations and muscle weakness4,6. Osteoarthritis treatment aim is to improve physical function, prevent disability, reduce or minimize pain and enhance quality of life7. In Singapore the Burden of Disease Study 2004 found that the osteoarthritis was the fifth leading cause of disability8.
One Iranian study concluded that prolonged squatting and cycling may be risk factors for development of knee OA, with housewives being at greater risk of developing knee OA than women whose main occupation was outside the home9. Disability is more rapidly reported in the cases of knee OA10. In the Netherlands, patients with hip and knee pain, of 55 to 74 years of age, are diagnosed with arthritis11. Globally OA causes moderate to severe disability in 43.4 million people as of 200411. The rate of reduced employment and lost work contribute to the indirect costs of musculoskeletal conditions12. Kellgren and Lawrence also defined a widely utilized grading system for knee OA13.
Grade 1: doubtful narrowing of joint space and possible osteophyte lipping
Grade 2: definite osteophyte, definite narrowing of joint space
Grade 3: moderate multiple osteophytes, definite narrowing of joint space, some sclerosis and possible deformity of bone contour
Grade 4: large osteophyte marked narrowing of joint space, severe sclerosis and definite deformity of bone contour. Ultrasound (US) is described as micro- massage.
These are essentially the same as sound waves but of higher frequency, such waves that are beyond the human audible range14. US is used to treat many musculoskeletal diseases and is also reputed to reduce edema, relive pain increase range of motion and accelerate tissue healing15. Ultrasonic energy is described as any vibration at a frequency above the sound range but it is frequency of a few megahertz that are typically used in physiotherapy several frequencies range from 0.5 to 5MHz. There are two frequency modes of ultrasound High frequency US and Low frequency US. They produce two types of effects, thermal and non-thermal. Thermal effects are due to the absorption of the sound waves. Non thermal effects are from cavitations, micro streaming and acoustic streaming16. Therapeutically we use this modality to generate heat within a body part3. The result of survey carried out in Britain in 1985 (ter-Haar, Dyson and Oakley, 1985) showed that 20% of all physiotherapy treatments in NHS department and 54% of all private treatments involved therapeutic US17. In 1985 survey, physiotherapists were asked to complete questionnaire covering a range of topics including technical details of their US machine, intensities, caliberation procedure and observed contraindications.
Low frequency US has good effects since the early 1990s there has been an interest in the use of low frequency US for the treatment of variety of tissue injures (Bradnock, Law and Roscoe, 1996). Typically, this modality operates at a frequency of around 44-48 kHz, which is significantly lower than the usual therapy ranges 1-3MHz.
HYPOTHESIS
The research hypotheses are as follows;
Ho: low and high frequency ultrasound provides same effects in the management of knee OA. Ha: low and high frequency ultrasound both have different effects in the management of OA.
METHODOLOGY
It is a pre-post design study conducted on 310 patients in the time period of nine months (January 2012-November 2012). The study includes male and female, with age range of 40-65 years. All participants were suffering from confirmed diagnosed osteoarthritis of knee joint accordance to the American College of Rheumatology criteria18. The consent was sought from the subject before participating into the study, thereafter; the subjects were randomly divided into two groups, Group A and Group B each consisting 155 patients. Both groups received same protocol of treatment, including ice pack {Preheating the treated area with a hot pack does not affect the deep-heating capacity of ultrasound (Lehman et al, 1978)}19 and stretching exercises except. Group A received low frequency US treatment of 0.01MHz frequency for 10 min and at the same side Group B received high frequency US treatment of 1MHz about 3 min. Both groups had six sessions in 3 weeks. Before and after the treatment of both groups we examined pain and disability of patient by different method. Pain intensity was examined by a visual analogue scale (VAS) both pre-treatment and post-treatment and disability was examined by a questionnaire in which pre-treatment and post-treatment scores are calculated by adding the numbers of answered options. Data was analyzed on SPSS. Patients fulfilling following criteria were included in the study: patient within age of 40-65years, patient with diagnosed knee osteoarthritis, patient with pain in knee and Grade1,2,3 OA of knee13. While patients fulfilling following criteria were excluded: patients with inflammatory arthritis, patient having fracture earlier around the knee, any neurological involvement, diabetic patient or patient with any cardiac disorder, tumor, malignancy, bone tissue infection, cardiac pace maker and over plastic implants20. Patients with grade 4 OA of knee were also excluded from this study13.
Study Setting
The study is taken in Physiotherapy department of North Nazimabad and Clifton Campus of Ziauddin Hospital, Karachi, Pakistan.
Variable of the Study
In the study following variables are being tested:
i . Knee pain
ii. Disability
Sampling Method
Sample size was calculated as 309.7 taking prevalence of knee OA 22-28% 21, at 95% confidence level and margin of error is 0.05. To avoid data wastage 310 Individual were included in the study.
Group A: 155 patients were selected with age range of 40 to 65 years. Group A received low frequency ultrasound.
Group B: 155 patients were selected with age range of 40- 65 years. Group B received high frequency ultrasound
Ethical Consideration
According to ethical consideration patient privacy is most important, patient hygiene factor, Patient therapist relationship and Environment of the place where we treat the patient.
Finding and Analysis
The finding and analysis is based on the three major parts:
1) It includes the basic statistical information of pre and post scores of the treatments
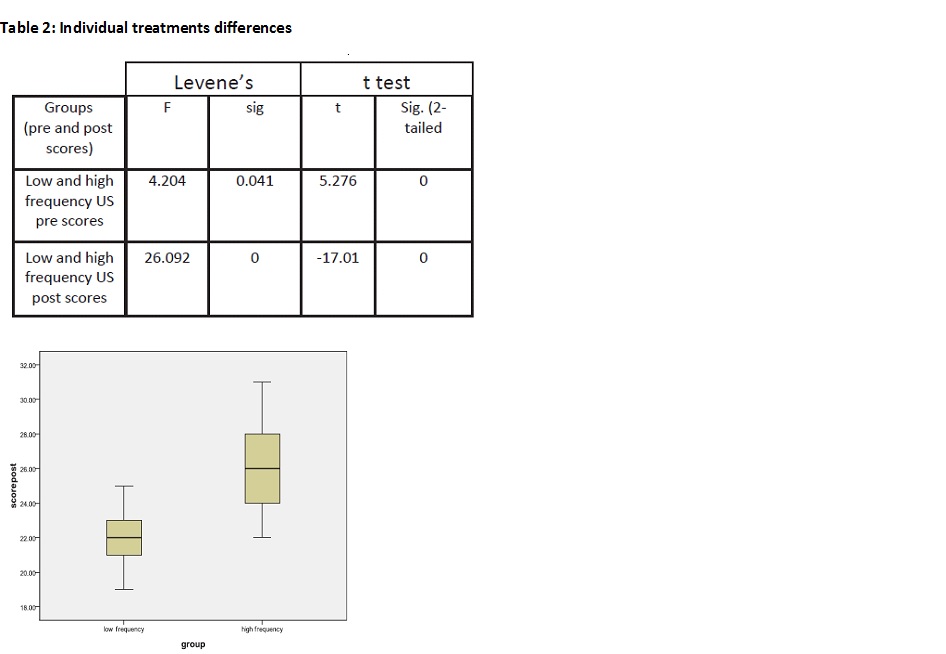
2) The box plot shows the normality of data and its variation which is been further discussed.
3) The third and final part of the Finding and analysis is based on the independent t-test which shows the efficient treatment among both groups.
RESULTS
The descriptive statistics (table 1) provides useful statistics for both groups A and B. The tables show the pre and post treatment efficiency. The sample which we have chosen is 310 (group A=155 and group B=155) ranges from the age of 40 to 65 which are further divided on the bases of gender (Male 35.8% and Female 64.2%). The significance of both the treatment is less than 0.05 which means both the treatments are effective.
The box plot shows that the high frequency ultrasound treatment has less efficiency in pain management of osteoarthritis of knee joint as compare to low frequency ultrasound treatment.
The data is normally distributed (table 2) and there are no outliers but the range of low frequency ultrasound is set to be less than as compare to the range of high frequency ultrasound treatment.
The Levene’s test for equality of variances in the independent sample t-test show that the variances of variable are statistically significant (if the significance is less than 0.05we assumed equal variances amongst the group) The t statistics shows that there is a difference between the effectiveness of both treatments. The significance level oft-statistics also shows the same result so we reject H0 that is low and high frequency ultrasound provides same effects in the management of knee osteoarthritis. At 95% confidenence interval we can say that Low and high frequency ultrasound both have different effects in the management of knee osteoarthritis the descriptive statistics also supported our result that there is a difference between the effectiveness of both the treatments.
We know that the low frequency ultrasound is more effective in the treatment of knee osteoarthritis. On the basis of descriptive analysis we can say that the low frequency ultrasound treatment is more effective as compare to high frequency ultrasound treatment in pain management of knee osteoarthritis. Low frequency ultrasound shows greater depth of penetration but lower spatial resolution it is mostly used for deeper structures and it often penetrates 4-5cm or more below the skin.
DISCUSSION
Several authors researched the effectiveness of therapeutic US and there controversial results in US efficiency20,22,23. The effectiveness of US is still inconclusive so, in this study we investigate the effectiveness of US in knee OA. In this study 310 patients were divided into two groups consist of Group A (155 patients) and Group B (155 patients) respectively, including male and female, with age range of 40-65 years Both groups received same protocol of treatment, including ice pack and stretching exercises except. Group A of 155 patients received low frequency ultrasound treatment of 0.01MHz frequency for 10 min and at the same side Group B of 155 patients received high frequency ultrasound treatment of 1MHz about 3 min. Both groups had six sessions in 3 weeks. Before and after the treatment of both groups we examined pain and disability of patient by different method. Pain intensity was examined by a visual analogue scale (VAS) both pre-treatment and post-treatment and disability was examined by a questionnaire in which pre-treatment and post-treatment scores are calculated. The descriptive statistics compares pre and post treatment scores which show the significance level of both the treatment is less than 0.05 which means both the treatments are effective. The box plot shows the data is normally distributed which indicates that the research which we conducted have no outliers. We have conducted independent sample t-test in which on bases of F statistics and its significance level the groups have equal variances. The further analysis is based on this assumption and it’s suggested that and high frequency ultrasound both have different effects in the management of osteoarthritis. Other studies show that ultrasound therapy is reported in relieving pain and improving in functions of knee osteoarthritis9,20,24,25, there is no evidence that US therapy is unsafe. In three trials no side-effects were reported both in the control group and in the US20,22,24.
CONCLUSION
We conclude that low and high frequency ultrasound both have different effects in the management of OA (on bases of 95% confidence interval). In accordance to these results, we conclude that in comparison of both treatments high frequency ultrasound and low frequency ultrasound, the low frequency ultrasound is found to be more effective to the patients.
ACKNOWLEDGEMENTS
We are really thankful to Almighty Allah for granting me wisdom and understanding to value through learning process. We also thankful to administrative and supporting staffs of Ziauddin Medical University for relevant information and supporting me throughout the course of my research. Special thanks: To Ms. Syeda Nida Imran and Mr. Syed Ahmed Raza Kazmi for all their help
REFERENCE
- Solomon DH, Bates DW, Panush RS, Katz Jn. Costs, Outcomes, and Patient Satisfaction by Provider Type for Patients with Rheumatic and Musculoskeletal Conditions: A Critical Review of the Literature and Proposed Methodologic Standards. Ann Inter Med 1997;127(1):52-60
- College NR, Walker BR & Ralston SH Davidson’s Principles and Practice of Medicine. 21st edition. China: Elsevier Science Limited; 2010. 1083-5
- Osiri M, Welch V, Brosseau L, Shea B, mcgowan J, tugwell P, wells G. Transcutaneous Electrical Nerve Stimulation for Knee Osteoarthritis. Cochrane Database of Systematic Reviews 2000;(4):CD002823.
- Leslie M. Knee Osteoarthritis Management Therapies. Main Manag Nurs 2000;1(2):51-57.
- Oliveria SA, Felson DT, Reed JI, et al. Incidence of symptomatic hand, hip and knee osteoarthritis among patients in a health maintenance organization. Arthritis Rheum 1995; 38(8):1134-41.
- Bennell KL, Hinman RS, Metcalf BR, Buchbinder R, mcconnell J, Mccoll G. et al. Efficacy of Physiotherapy Management of knee joint Osteoarthritis: A Randomised, Double Blind, Placebo Controlled Trial. Ann Rheum Dis 2005;64(6):906-12.
- Felson DT, Zhang Y, Hannan MT, et al. The Incidence and Natural History of knee Osteoarthritis in the Elderly. The Framingham Osteoarthritis Study. Arthritis Rheum 1995;38(10):1500-5.
- Phua HP, Singapore’s burden of disease and injury, Singapore Med J 2009;50(5):468-478.
- Dahaghin S, Tehrani-banihashemi SA, Gaezi ST, Jamshidi AR, Davatchi F. Squatting, sitting on the floor or cycling: are life-long daily activities risk factors for clinical knee osteoarthritis. Arthritis Rheum 2009;61:1337–42.
- Huang MH, Lin YS, Lee CL, et al. Use of Ultrasound to Increase Effectiveness of Isokinetic Exercise for knee Osteoarthritis. Arch Phys Med Rehab 2005;86(8):1545-51.
- Hopman-Rock M, de Bock GH, Bijlsma JW et al. The pattern of health care utilization of elderly people with arthritic pain in the hip or knee. Int J Qual Health Care. 1997;9:129 –137.
- Yelin E. Cost of musculoskeletal diseases: impact of work disability and functional decline. J Rheumatol Suppl. 2003;68:8–11.
- Kellgren JH, Lawrence JS, J, et al. Radiological assessment of osteo- arthrosis. Ann Rheum Dis 1957; 16(4):195-25
- Low J. Electrotherapy explained principle and practice. 3rd ed. Bostan: Butterworth heinemann; 2000.172-7
- Vander DA, Vander GJ, Vanden SG. Ultrasound Therapy for Musculoskeletal Disorder: a systemic review. 1999;81:277-71.
- Steven, MO, Constantin CC, Len S, Robert Carlisle. Ultrasound-Enhanced Drug Delivery for Cancer. Expert Opinion on Drug Delivery 2012; 9(12):1525.
- Kitchen S, Young S Electrotherapy. 11th ed. Elsevier Science Limited; 2002.211-4
- Hochbery MC, Atlam RD, Brandth KD, et al. Guide Lines for the Medical Management of Osteoarthritis Part2. Osteoarthritis of knee American College of Rheumatology. Arthritis Rheum 1995;38(11):1541-6.
- Belanger AY, & Therapeutic Electrophysical Agents. 2nd ed. China: Lippincott Williams and Wilkins; 2009.405-6
- Tascioglu F, Kuzgun S, Armagan O, Ogutlerget Al. Short Term Effectivness of Ultrasound Therapy in Knee Osteoarthritis. J Int Med Res 2010;38(4):1233-42.
- Anita YN, Doherty M. What of Guide Lines for Osteoarthritis. Int Journal Rhem Dis 2011;14(2):136-44.
- Falconer J, Hayes KY, Change RW. Effects of Ultrasound on Mobility in Osteoarthritis of the Knee. Arthritis care Res 1992;5(1):29-35.
- Cetin N, Aytar A, Atalay A, Akmanmn. Comparing Hotpack, Shortwave Diathermy, Ultrasound and TENS on Isokinetic Strength, Pain and Functional status of Women with Osteoarthritic Knees: A Single Blind, Randomized, Controlled Trial. Am J Phys Med Rehabil 2008;87:443-51.
- Ozgonenel L, Aytekin E, Durmusoglu G. A Double Blind Trial of Clinical Effects of Therapeutic Ultrasound in knee Osteoarthritis. Ultrasound Med Bio 2009;35(1):44-9.
- Kozanoglu E, Basaran S, Guzel R, Guleruysalf. Short Term Efficancy of ibuprofen Phonophoresis versus Continuous Ultrasound Therapy in Knee Osteoarthritis. Swiss Med Wkly 2003;133:333-8.