
ABSTRACT
OBJECTIVE
To determine the effect of aerobic exercise training on the quality-of-life QoL, morbidity, mortality of patients with Heart Failure (HF)
SEARCH STRATEGY
EBSCO Host, MedLine, Cochrane database, CINHAL, Ovid, AMED were the databases searched, from 1999 to 2010 which was the peak era of implementation of aerobic exercises for HF and other cardiac diseases.
SELECTION CRITERIA
The studies that involved aerobic exercise either in combination or alone were included according to the criteria of New York Heart Association (NYHA) class I-III HF patients. Randomized control trails (RTCs) and systematic reviews were included in the study.
DATA COLLECTION AND ANALYSIS
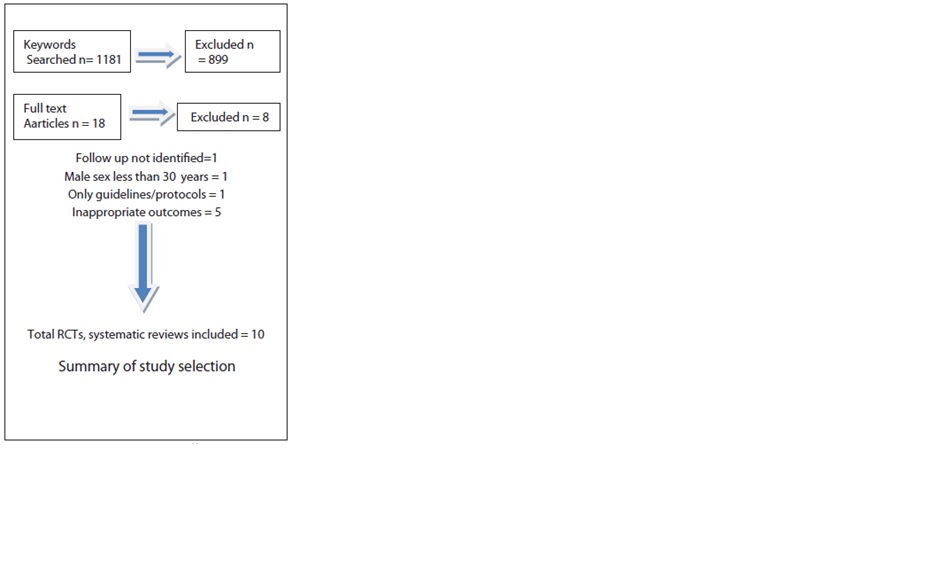
The screening of the papers was done by three review authors. The initial screening was conducted by the first author followed by further selection by the second and third.
MAIN RESULTS
10 articles met the inclusion criteria including 3 systematic reviews. 3647 participants made one trial greater than the rest. The average age observed was from 30-82 years, where males were dominating in almost all studies. The review reveals no statistical differences in the mortality and morbidity. There was no individual effect of aerobic exercise on QoL whereas better results were reviewed when performed in combination.
CONCLUSION
Aerobic exercises have improved the physiological function, aerobic capacity and quality of life among the patients suffering with HF. However, these exercise therapies were given in combination with resistance training but distinct essence for mortality, morbidity and QoL need to be investigated further in the review.
Keywords
Aerobic Exercises, Chronic Heart Failure, Exercise Training, Aerobic Capacity, Cardiac Rehabilitation, Walking, Treadmill, Cycling Ergometer.
Amna Aamir Khan
Senior Lecturer
Ziauddin College of Physical Therapy
Ziauddin University
Navaid-us-Saba
Senior Lecturer
Ziauddin College of Physical Therapy
Ziauddin University
Muhammad Usman Khan
Senior Lecturer
Ziauddin College of Physical Therapy
Ziauddin University
Khan AA, Navaid-us-Saba, Khan MU. Aerobic Exercises in Heart Failure – A Review. Pak. j. rehabil. 2012;1(1):3-8]
INTRODUCTION
Heart Failure (HF) has been prevalent throughout the world as the leading cause of morbidity and mortality1 which increases the incidence with the growing age2,3. It has been estimated that more than 550,000 patients suffering with Chronic Heart Failure (CHF) at least once in their lifetime4. Several causes may lead to HF but myocardial dysfunction has been termed as one of the common causes specifically systolic that is; there is a reduced ventricular contraction5. Unfortunately, its prevalence has not been investigated by the researchers in Pakistan. However, the etiology of CHF has been examined in one of the studies6. Initially, patients suffering with HF were advised rest during cardiac phase I and II, resulting in prolong rehabilitation7. With the advent of time, the importance of early mobilization out of bed and physical activity is highlighted and encouraged8. A number of Activities of Daily Living (ADLs) were introduced in the cardiac rehabilitation center but remained a challenge especially in Pakistan.
Inability to perform aerobic exercise was considered as the hallmark for all the patients suffering with HF9. Despite of the pharmacological therapy, the prognosis of the HF patients is poor but exercise training has markedly shown improvement in exercise capacity10, quality of life (QoL) 11,12, mortality and morbidity1. The negative effects on QoL have been increased due to fatigue and dyspnea which may be altered by exercise training13. Aerobic exercise trainings have been well established than non- pharmacological treatment presenting its effectiveness on the exercise capacity to improve the QoL. Moreover, the mortality and morbidity of the patients with HF has also decreased.
The objective of this review is to reveal the importance of aerobic exercises among patients suffering with HF in order to implement the practice among the clinicians in Pakistan.
METHODS
Search & Keywords
EBSCO Host, Medline, Cochrane database, CINHAL, Ovid, AMED were the databases searched, from 1998 to 2010 that was the peak era of implementation of aerobic exercises for HF and other cardiac diseases patients. Some American and a few European journals were inaccessible. The key words such as aerobic exercises, chronic heart failure, exercise training, left ventricular dysfunction, aerobic capacity, cardiac rehabilitation, quality of life, mortality, morbidity, walking, treadmill, cycling ergometer were used.
Study Selection & Data Collection Process
10 studies were included in the review; 3 systematic reviews and one meta-analysis were selected. None of these studies emphasized on aerobic exercise alone but these exercise trainings were performed in almost all the reviewed studies either as a single intervention or combined with resistance exercise program to assess the impact on the outcome measures. The studies selected used oxygen consumption capacity, morbidity, mortality and fatigue as their outcome measures. 4 of 10 studies used aerobic exercise but the rest measured both aerobic and resistance exercises, none of the study selected used resistance training only. The effectiveness of exercise-based rehabilitation in patients with CHF has been demonstrated in the earlier systematic reviews10,14. The data extracted from both the reviews were almost the same yet a few differences in the outcome measures
were noticed. Recently, Davies et al15 selected 19 Randomized Control Trials (RCTs) with almost 3647 patients; to compare exercise training for systolic HF. Health Related Quality of Life (HRQoL), mortality, hospitalization and cost effectiveness was also reviewed. The maximum sample size considered in any of the 19 RCTs was 200 patients where maximum number of male patients was selected. Out of these 19 RCTs, 9 studies considered 100% male members whereas the remaining consists of more than 72% of them. The recruited subjects were without any complications fulfilling the New York Health Association (NYHA) class II and III criteria. The mean age selected for these patients were from 43 to 72 years. A combination of aerobic and resistance training was used and different exercise training programs were selected. Moreover, these studies were mostly conducted in Europe and United States of America whereas only 1 was conducted in United Kingdom. Most of the judgments of the trials were based on exercises-only interventions. However, the psychological intervention was also provided in one of the studies. The duration of the training programs were 15-20 minutes and the frequency of 2-7 sessions per week. It was mostly an outpatient program whereas one of the study was home based. The interventional group received the cardiac care whereas the control group received no intervention at all; just routine medicines. The HRQoL was mostly measured through disease-specific MLWHF, whereas others used Psychological Wellbeing Index (PGWB), Kansas City Cardiomyopathy Questionnaire (KCCQ), Spritzer’s Quality of Life Index (QLI) and Patients Global Assessment of Quality of Life (PGAQoL). Most of the reviewed studies reported significant improvement with aerobic exercise whereas remaining showed a few limitations. However, while assessing the effects on mortality; no statistically significant results were obtained in the study. These results remain similar with the previous meta-analysis of ExTraMATCH Collaboratives14 between the exercise and the control group. Rees et al10 by performing RCTs select all the adults with CHF to determine the effectiveness of the exercise-based interventions compared with the usual medical care on the mortality, morbidity, exercise capacity and QoL. All the RCTs of the exercise-based intervention were selected. Data was extracted from 29 studies which met the inclusion criteria. 24 studies measured the maximum oxygen capacity (VO2 max), 15 studies measured the exercise duration and 6 studies recorded the work capacity. All the patients showed a left ventricular ejection fraction of less than 40%. The mean ages ranged from 51-77 years. All the studies selected for the review dominated the male patients and may be considered as one of the major limitations16; only 2 studies recruited the female patients. The VO2 max measured in 24 studies with 848 patients randomly allocated. Large improvement effects were seen in VO2 max with the exercise training group by 2.16ml/kg/min. 23 out of 29 trials evaluated an aerobic intervention and 6 has been reported as the resistance training of the peripheral muscle group. It may be considered that aerobic training may have contributed more to increase the exercise capacity. A sensitivity analysis was carried out by excluding the studies that focused completely on the resistance training in order to determine the impact of aerobic exercise. Results showed that it had no significant effects on the pooled analysis for the outcome of VO2 max. The exercise duration and work capacity also showed a remarkable increment. Greater improvements were seen in patients aged less than 55 years since age is reported as an aggregate measure but it is inappropriate to get the individual data. The duration was measured in 15 studies (510 patients randomized) increased by 2.38 minutes and work capacity by 15.1 Watts. It may be assumed that the increasing follow up may have increased the effect of the outcome measures. Exercise capacity was assessed by the maximum oxygen uptake; distance on 6 Minute Walk Test (6MWT) and the physical work capacity. The distance on 6MWT was measured in 282 patients; that increased by 40.9m. It is significant to improve the exercise capacity as decrease in it, restricts the ADLs; influencing an individual’s independence and QoL9.
Rees et al10 also reported the results that were obtained from the 9 trials out of 29 on HRQoL as an outcome measure. Different intervention groups (aerobic & resistance) uses different scales in order to measure the HRQoL. 7 out of 9 studies showed improvements in the intervention group then in the control group. 5 studies used the disease specific Minnesota Living with Health Failure Questionnaire17 where significant improvements were seen in 4 of 5 studies but these improvements shown for a small duration. Out of these 5 studies 2 of them measured the HRQoL for a longer duration and 1 of these showed a sustained improvement which was maintained over an extended period of time. Aerobic exercises improved the QoL by improving the physical activity of the patients with HF, but all aerobic capacity depends on the Frequency, Intensity, Time and Type (FITT) of exercises performed18. It may also depend on modalities used, more commonly treadmill and bicycle ergometer9. No generalized guidelines for all heart failure were recommended precisely but individual modifications were required.
Previously, Lloyds-Williams1 also investigated the effects of exercise training on the patients with CHF, aged between 50-82 years. They were randomly selected to assess the physical performance (e.g. increased peak oxygen uptake, cardiac output, aerobic capacity, mortality and QoL. The studies which have the influence of drugs on the physical performance of the patients and affecting the outcome measure were excluded; along with it those studies consisting of the biomedical changes due to exercise training were also excluded. All the studies reporting the languages other than English were also placed in the exclusion criteria. Wide range of databases from 1996 to 2000 was used and relevant American and European journals were studied but due to unavailability of some electronic journals the data was scrutinized. CINHAL and AMED were not surfed to find the studies. Out of 31 studies 14 were prospective RCTs, 8 were randomized crossover trails, 2 were non randomized control trials and 7 were pre-test and posttest studies. The total number of participants included in the study was 1010. The male participants again dominated the review and only 1 study focused on females exclusively. Out of 31, 10 studies were exclusively focusing on males. Different exercise trainings were included in the review but in most of the studies aerobic trainings were implemented. Although aerobic exercise was not clearly mentioned in the study nor differentiated but the training modalities mentioned in the study made it clear. Mostly a supervised, hospital-based program was included in this review and the patients used a cycle ergometer commonly. Other modalities were also used in combinations such as swimming, jogging, walking and different circuit trainings. Activities such as step exercises, calisthenics, ball games, resistance exercises, and anaerobic training were also focused. Home based programs were included in the review and in 7 studies patients with cycle ergometer and treadmill were given for home use. All these programs were short termed with duration of 4 to 52 weeks. The frequency to perform aerobic exercises was ranged from 1 to 7 times per week; with the session lasting between 10 to 60 minutes. A descriptive synthesis was undertaken but the difference between the studies was not investigated. The amount of oxygen uptake was not ranged but was tabulated and most of the patients were working on mild to moderate intensity; ranged 50% to 70% HR. Mostly the studies that were included were of small sample size less than 50 participants. The patients included were mostly convenient samples and were of younger age whereas the major population age of HF is much higher. The HF patients with comorbidities were excluded so it cannot be generalized to the vast population. There was no classification of the patient mentioned according to the risk stratification or any other classification. A number of discrepancies were present in the number of studies included such as a lack of precision in study designs were found. The training programs were of small duration and mostly lasted for 8 weeks or less whereas only two studies lasted for a year. 16 studies measured the QoL and 11 were found to be beneficial, although small duration decreased the usefulness due to short duration.
Short term exercise training was found to be beneficial in the selected groups of patients and physiological Improvements were notified among these patients. Exercise training has shown positive effects but it may be difficult to evaluate whether the improvements were due to aerobic alone or in combination with resistance exercises.
CHF occurs when heart is unable to pump sufficiently leading to exertion, breathlessness and fatigue5, as one of the major symptoms. Inability to perform the aerobic exercise is the characteristic feature of heart failure9 and the researchers are looking at the effects of exercise training on fatigue and dyspnea in the HF so that the central hemodynamics and the cardiac pumping capacity can be improved. Aerobic training may contribute to decrease the exercise intolerance, fatigue and dyspnea. Pozehl et al 13 conducted a pilot study in order to see the effect of 24-week exercise training on fatigue and heart failure. 19 male and 2 females where recruited by a RCTs. The randomization was done in the ratio of 2:1 that is; twice the intervention group when compared with the control group. The average age among them was 66 years with an ejection fraction of 28.4±7.4%. These patients were classified according to the NYHA in the class II, III and IV. The eligibility criteria also included the patients who were able to read and speak English. The left ventricular ejection fraction recorded was < 40%. A 24-week program was given to these patients. Both aerobic and resistive training at a frequency of 3 times per week was given and each session of 60 minutes was allotted. Aerobic exercises were given for 30 minutes excluding the time of warm-up and cool down (5 minutes each). Four different modalities were used that is; treadmill, stationary bike, rowers and arm ergometers. Piper Fatigue Scale (PFS) and Dyspnea Index (DI) were used to measured fatigability and dyspnea. 20 minutes of resistance training was given and the patients were advised to work at the intensity of 60-80% of VO2 max and the Rate of Perceived Exertion (RPE) should be 12-14 on the BORG Scale. 23 subjects were selected out of which only 21 completed the study but 1 patient from the control group died of Myocardial Infarction. 1 subject was diagnosed with cancer and was unable to continue the exercise. Patients remained on their pharmacological treatment where ACE inhibitors, B Blockers and diuretics were prescribed. Results showed marked improvements in fatigue overtime in exercise trained heart failure (p<0.05) on the PFS scale where as significant decrease in sensory subscale of PFS in the training group was noticed. However, non-significant results were obtained on the DI. The average adherence rate for the exercise group over 24 weeks intervention was 91.8%. Both aerobic and resisted exercises have improved the perceived sensory fatigue of the trained subjects, slight improvements were seen in the control group but only till 12 weeks then these were worsened by 24 weeks. A few limitations were there in the study; a lack of sample size and statistical power was the major obstacle. Therefore, this study may attribute to overcome the symptoms experienced by HF patients but it would be difficult to confirm which intervention might have been significant. It is considered that aerobic training has decreased fatigue whereas resistance training may have improved the strength of the muscle19.
Similar research was conducted by Witham et al20 but the duration of study was reduced to only 12 weeks. A sample of convenience of 26 patients aged more than 70 years was recruited, out of which the follow-up of only 15 was received. All the patients either fell in class II or III; according to NYHA. Patients suffering from aortic stenosis, sustained ventricular arrhythmia, uncontrolled atrial fibrillation, and unstable angina were excluded from the study. Hospital Anxiety and Depression Score (HADS), Functional Limitation Profile (FLP), and Guyatt Chronic Heart Failure Quality of Life Questionnaire were also measured. The two-week program consisted of both aerobic and resisted training, of both the upper and lower limbs performed in both standing and sitting positions. The classes lasted for 60 minutes of exercises and its effectiveness was tested for the 6MWT at baseline and after the program. A proper warm up and cool down phases were considered. These aerobic exercises prepared the body for the work load on the heart18. Although timings of warm-up and cool down were not mentioned in the methodology neither a separate recommendation were given especially for the heart failure patients but in general a warm up for 15 minutes for cardiac patients with HF are recommended21. The exercises were easily completed by the patients where no monitoring was undertaken although it was a group of older aged people. Although it was a pilot study so the conclusion of efficacy of interventions cannot be drawn out of it still the patients showed good toleration for the training program. Only one adverse event was recorded involving a fall from the step so the interventions may be considered safe. The results showed an increase in exercise capacity in HF patients but it might be difficult to state whether this increment on the 6MWT was due to aerobic or resisted exercises. Furthermore, the attendance was 80% for the program emphasizing that the patients may have increased the physical activity but the provision of taxi transport may have induced an element of bias in it. Overall, the two weekly groups focusing on aerobic endurance and everyday functional task was accepted and tolerated.
Several small studies have shown that aerobic exercises increase the exercise capacity of patients suffering with CHF. Four different studies were conducted using aerobic exercises as their intervention protocol (Yamomto et al22, Cao et al23, Hambrecht et al24, and Sturm et al25). All these selected RCTs concentrated on improving the exercise capacity of patients suffering with HF, a sample size of 125 patients (8, 26, 73, 18) was recruited from all these studies. Only one study had a larger sample size25 the rest had a sample size less than 30. Moreover, only one of these studies measured the effects of exercise (aerobic training) on the central sleep apnea in CHF. All of these patients fall in the category of NHYA class II and III. Males remained dominant as being in the other studies. The study conducted by Hambrecht recruited 73 males only. Step aerobics, cycle, treadmill, bike, arm weight, arm ergometer walking, calisthenics, ball games, bicycle ergometers were used as intervention modes. One study measured the effects of both aerobic and resistance training (Cao et al23) showing marked improvement in the muscle strength and endurance. However, when a comparison was made between the upper and lower extremities; improvement in the muscle strength was more pronounced in the lower extremity. Moreover, resistance exercised groups improved in the muscle endurance of all 5 muscle groups (triceps, lattismus dorsi, biceps, quads and hamstrings). Aerobic training improved more of cardiopulmonary capacity. The combination of aerobic and resistance exercises improved the pulmonary fitness, muscle strength and reduced the fatigue. These results were similar with other studies13.
A home-based program was used by Hambrecht et al24 in the study where patients were randomly assigned to 2 weeks in the hospital performing the ergometer exercise for 10 minutes and 4 – 6 times per day, followed by a home-based program of ergometer exercise training for 20 minutes per day at 70% peak oxygen uptake to a no intervention in the control group. The central hemodynamics was measured by thermodilution at rest and even during the exercise. Echocardiography was conducted to determine the left ventricular diameters and volume; and baseline follow up of 6 months was given for the exercising and control groups. It revealed that exercise trained group had statistically significant improvements when compared with the control group. Maximum ventilation, exercise capacity, and exercise time also showed marked progress. A decrease in heart rate and stroke volume at rest was also documented. A reduction in the peripheral resistance occurred with small but significant improvement in cardiomegaly. Similar results were obtained for the remaining two studies (Hambrecht et al24 Sturm et al25).
These studies conducted mostly focused on laboratory based or out-patient programs where patient exercise under the controlled conditions but these exercises was not applicable for all the patients due to inaccessibility of the formal program. Many home-based programs have been established for these patients. Dracup et al26 randomized 173 with systolic heart failure. Out of which 87 were placed in the control group and 86 were allocated a home-based exercise program. The patients aged between 18 – 80 years were all English-speaking people. The NYHA ll classification criteria were followed whereas the patients with myocardial infarction were all excluded from the study. The exercise groups were assigned to perform a graduated, low level exercise protocol consisting low level aerobic exercise and resistance training. Aerobic exercise was initially given for 10 minutes at a maximal heart rate of 40% and progressively an increment up to 45 minutes at 60% of HR for the remainder program. The patients were given a prescription for their 4 weekly sessions until a progression was made up to 45 minutes of walking. After 6 weeks, the aerobic training was optimized and resisted training was added. Upper and lower body strengthening exercises for 3 days per week was given, pedometers were used which has found to be reliable27. Patients recorded the distance traveled and minutes walked on weekly and then on monthly visits. Composite end points were selected over a single outcome to increase the number of events over 1 year period of follow-up. All-cause mortality and all-cause hospitalizations were selected over HF. The results indicate patients in the exercise group had a significantly higher probability of having coronary heart disease. Neither deaths nor exercise related injuries were reported in the study. The results from the study indicated that there was a significant difference between the multiple hospital readmissions for both the exercise group and control group.
SUMMARY OF EVIDENCE
Aerobic training, as part of comprehensive program has shown highly significant improvements in functional capacity, muscle strength, QoL and reducing the mortality in the individuals with HF but the effects were short termed. It has also shown central adaptation to the exercising patients with CHF although initially it was thought that it is due to peripheral adaptations27. The studies suggest that moderate intensity exercise training is safe and progression of exercise should be followed according to the FITT principal. Continuation of exercise training must be till the results are beneficial. Mostly the trials are hospital based and home programs are not kept under consideration. Walking and cycling are mostly advised among these patients. It has been prescribed that 30 minutes of activity daily or in 3 different bouts is sufficient for a patient18. Various studies have been conducted to determine the optimum frequency for cardiac rehabilitation programs but the debate is still ongoing.
LIMITATION OF THE STUDY
A large amount of literature is available concerning training for the patients with HF although methodological problems are associated with many studies. 40% of the review consist of meta-analysis and systematic review due to which most of the trials where covered. Trials often involved consist of small number of patients and are of short duration that does not make it a representative of the large population of CHF. There are some marked limitations in the review. Firstly, both homes based and hospital-based studies are considered. Although, the hospital-based programs are safe, yet the impact on the outcomes remain different in both the environment that has been recently explained by Piepoli et al 20118. There are some evidences that exercise training improves exercise tolerance and QoL but no single randomized trials have looked at the mortality over a sustained period9. All these studies have considered different regimes and varied outcome measures but generalization regarding exercise training is difficult. Although aerobic exercise has been recommended as a vital part of cardiac rehabilitation and is suggested as a non-pharmacological approach in the management of CHF yet the significance of these trainings among sleep related abnormalities has not been studies well. However, some significant results are obtained for the patients suffering with sleep apnea 22. It is recommended that further studies particularly among the elderly patients and those with more severe CHF should be conducted with a larger sample size. Also, the follow-up of the patients is not uniform in the study and gender is also limited to only men, which needs to be further investigated.
CONCLUSION
Exercise training is recommended for all the patient suffering with HF if they fulfill the New York Heart Association (NYHA) class I-III8. Therefore, aerobic exercises should be conducted 2 to 3 times per week for the minimum of 8 weeks to achieve physiological adaptation5 for the patients with heart failures. Beneficial outcome results may be achieved when optimal physiological and psychosocial requirements are fulfilled18. The duration of aerobic exercise varies from 15 – 60 minutes. A proper warm up and cool down phases should always be advised by physical therapist. It is advised initially that the patients with CHF should avoid physical activity and rest is recommended but for the past few decades promising results are obtained when exercise training is introduced among the patients. Recently, a moderate supervised exercise program for the patients who are in class NYHA class-II & III are advised in order to improve the exercise tolerance and QoL is been recommended28, 29. Debate is still going on to clarify the type of exercises advised to the patients with CHF and the effects of it.
REFERENCE
- Lloyd-Williams F, Mair FS, Leitner, M. Exercise training and heart failure: a systematic review of current evidence. The Br J Gen Pract 2002;52(474):47-55
- Collins SP, Hinckley WR, Storrow AB. Critical review and recommendations for nesiritide use in the emergency department. J Emerg Med 2005;29:317-29.
- Kannel WB, Belanger AJ. Epidemiology of heart failure. Am Heart J 1991;121:951–7.
- American Heart Association. Heart Disease and Stroke Statistics: 2005 Update. Dallas, Tex: AHA;2005.
- Scottish Intercollegiate Guideline Network SIGN. Management of chronic heart failure: A national clinical guidelines. 2007 [Online]. Available from: www.sign.ac.uk/pdf/sign95.pdf [Accessed 1st March, 2011]
- Khan Z, Khan B, Haider I, Khan I, ud- Din J, Khan H et al. Etiology of congestive heart failure at a tertiary care hospital. RMJ 2010;35(2):141-144
- Ishaq M, Jamal Q. Treatment of Heart failure under current guideline. Pak Heart J 2001;34(1-4):29-37
- Piepoli MF, Conraads V, Corrà U, Dickstein K, Francis DP, Jaarsma T et al. Exercise training in heart failure: from theory to practice. A consensus document of the Heart Failure Association and the European Association for Cardiovascular Prevention and Rehabilitation. Eur J Heart Fail 2011 Apr;13(4):347-57.
- Pina IL, Apstein CS, Balady GJ, Bekardinelli R, Chaitman BR, Duscha, BD et al. Exercise and heart failure: A statement from the American Heart Association committee on exercise, rehabilitation and prevention. Circulation 2003;107(8):1210-25
- Rees K, Taylor RS, Singh S, Coats, A, Ebrahim S. Exercise based Rehabilitation for Heart Failure. Cochrane Database of Syst Rev 2004;(3)
- Mandic S, Riess K, Haykowsky MJ. Exercise training for individuals with Coronary Artery Disease or Heart Failure. Physiother Can 2005;58:21-29
- Flynn KE, Piña IL, Whellan DJ, Lin L, Blumenthal JA, Ellis SJ e tal. Effects of exercise training on health status in patients with chronic heart failure: HF-ACTION randomized controlled trial. JAMA 2009 Apr 8;301(14):1451-9
- Pozel B, Duncan K, Hertzog M. The effects of exercise training on fatigue and dyspnea in heart failure, Eur J Cardiovas Nurs 2008 Jun;7(2):127-32
- ExTraMATCH Collaborative. Exercise training meta-analysis of trials in patients with chronic heart failure (Cover story). BMJ 2004;328(7433):189-192.
- Davies EJ, Moxham T, Rees K, Singh S, Coats AJS, Ebrahim S et al. Exercise training for systolic heart failure: Cochrane systematic review and metaanalysis. Eur J Heart Fail 2010;12:706- 715
- Haykowsky MJ, Liang Y, Pechter D, Jones LW, Mc.Alister FA, Clark AM. A meta-analysis of the effect of exercise training on left ventricular remodeling in heart failure patients: the benefit depends on the type of training performed. J Am Coll of Cardiol 2007;49(24):2329-2336.
- Riegel B, Moser DK, Rayens MK, Carlson B, Pressler SJ, Shively M et al. Ethnic Differences in Quality of Life in persons with heart failure. J Card Fail 2008;14(1):41-7
- Thow, MK (Ed). Exercise Leadership in Cardiac Rehabilitation-Evidence based Approach. 2006.
- Wiley and Sons, West Sussex.
- Magnusson G, Rong LK, Isberg B, Sylven C, Saltin B. Exercise capacity in heart failure patients: relative mportance of heart and skeletal muscle. Clinical Physiology 1996;16(2):183-195
- Witham MD, Argo IS, Johnston DW, Struthers AD, McMurdo ME. Predictors of exercise capacity and every day activities in older heart failure. Eur J Heart Fail 2006:8(2);203-207
- Myers JN, Brubaker PH. Chronic Heart Failure. In: Durstine JL, Moore GE (Eds.) ACSM’s Exercise Management for Persons with chronic disease and disabilities 2nd Edition. USA: ACSM Group; 2003. p. 64-69
- Yamamoto U, Mohri M, Shimada K, Orguchi H, Miyata K, Ito, K, et al Six- month aerobic exercises training ameliorates Central sleep apnea in patients with chronic heart failure. J 2007:13(10);825-829
- Cao W, Shieh J Rana MI, Haberl E, Jones JD, Naughton Patients With Congestive Heart Failure Arch Phys Med Rehabil 2005;8(9):e14
- Hambrecht R, Gielen E, Linke A, Fiehn E, Yu J, Walther C, Schuler N, Schuler G. Effects of exercise training on left ventricular function and peripheral resistance in patients with chronic heart failure: A randomized trial. JAMA 2000;283(23):3095-3101
- Sturm B, Quittan M, Wiesinger GF, Stanek B, Frey B. Pacher R. Moderate- Intensity exercise training with elements of step aerobics in patients with severe chronic heart failure. Arch Phys Med Rehabil 1999;80(7):746-750
- Dracup K, Evangelista LS, Hamiltion MA, Erickson V, Hage A, Moriguchi J, et al. Effects of a home-based Program on the Clinical outcomes in the heart failure. Am Heart J 2007;154(5):877- 883
- Mezzani A, Corra U, Giannuzzi P. Central adaptations to exercise training in patients with chronic heart failure. Heart Fail Rev 2008;13(10): 13- 20.
- Cowie A, Thow MK, Granat MH, Mitchell SL. A comparison of home and hospital-based exercise training in heart failure: immediate and long- term effects upon physical activity level. Eur J Prev Cardiol 2011;18(2)158-166
- Swank AM, Funk DC, Manire JT, Allard AL, Denny DM. Effect of resistance training and aerobic conditioning on muscular strength and submaximal fitness for individuals with chronic heart failure: influence of age and gender. J Strength Cond Res 2010;24(5):1298-1305