
ABSTRACT
BACKGROUND
Shisha and cigarette are the two most common type of tobacco smoking. Cigarette and shisha smoking have grown fast in different ages globally. Shisha and cigarette both contain chemicals that affect health badly and can cause common diseases such as cough and some life threatening diseases like cancer, emphysema and bronchitis also affect bones causing osteoporosis and decrease functional capacities of lung. There are no proper guidelines for the awareness of the public about the hazards of shisha smoking as they are present for cigarette smoking but it’s a fact that shisha smoking is as harmful as cigarette smoking
OBJECTIVES
To compare the effect of Inspiratory Reserve Volume (IRV) on shisha and cigarette smokers by using spirometer.
STUDY DESIGN AND SAMPLING TECHNIQUE
Cross-sectional survey was steered, convenient sampling was used.
STUDY SETTINGS & PARTICIPANTS
The study was conducted on 50 participants of Ziauddin College of Nursing and Ziauddin College of Physical Therapy
RESULTS
IRV is more compromised in shisha smokers than in cigarette smokers. As far as deciding between health concerning effects of shisha and cigarette smokers, the shisha smoking effects are same as cigarette smoking.
CONCLUSION
Shisha smokers have more exposure to tobacco than cigarette smokers. IRV is disturbed by both means of smoking but shisha smoking has more potential risks.
Keywords
Inspiratory Reserve Volume, Spirometer, Cigarette, Smokers, Shisha, Emphysema, Bronchitis.
Muhamamd Usman Khan
Assistant Professor
Ziauddin College of Physical Therapy
Ziauddin University
Alisha Noreen
DPT Student
Ziauddin College of Physical Therapy
Ziauddin University
Ramsha Kafeel
DPT Student
Ziauddin College of Physical Therapy
Ziauddin University
Yusra Sabahat
DPT Student
Ziauddin College of Physical Therapy
Ziauddin University
[Khan MU, Arif Z, Noreen A, Kafeel R, Sabahat Y. Comparing the effects of Inspiratory Reserve Volume in Cigarette and Shisha smokers by using Spirometer. Pak.rehabil. 2015;4(2):38-44]
INTRODUCTION
Smoking has global health risk and cigarette smoking has been recognized to boost the morbidity and fatality rate in both genders. It is a common thinking that tobacco associated hazards can be diminished by altering the way tobacco is used including the use of cigar, pipes or using other classic modes. Younger representative of our society even women boost up to adopt smoking methods1.
Shisha is a traditional way of tobacco use in developing countries about 400 years ago. Shisha is alsoknown as Hookah, Ghoza, Narghile, And Waterpipe and Hubble Bubble Smoking2 is used by the people of Middle Eastern or Asian countries3. Tobacco implanted in pot at the top of apparatus which is linked to the water filled base by a duct. The pot is then closed by a porous material. Flaming charcoal is then situated on the top; the smoke from the charcoal is dragged through the tobacco descending into the duct towards the water. After bubbling over the water the chilled smoke surfaces and is stained through the hose and inhaled. Mostly water pipe has a choke to restrict the quantity of smoke puff in. Electrical jet is also feasible nowadays, which offers abrupt smoke than the initial charcoal4.
In recent years the hookah has been modernized and become socially acceptable3. It is more common in U.K nowadays. In Middle East in young adult the prevalence rate is 19% -54%, in males ratio is about31% to 63% and in females it is 23% to 69%5-7.
In Pakistan 75% to 80% adolescents smoke shisha8-9. Male’s ratio is higher in cigarette smoking that is 60% but in shisha smoking female ratio is more than males that is 62%10.
Use of tobacco with sweetened fruits and molasses sugar makes the shisha smoke more aromatic and attractive3. Shisha smoke contains toxins because shisha has same contents as cigarette, such as nicotine, tar, carbon monoxide and heavy metals like arsenic and lead3.
It is a very false approach that herbal shisha is safer than any other kind of smoking. This is because containing fruit or herbal aromas does not make the shisha healthy. Even if the shisha is tobacco free, it still contains carbon monoxide or charcoal that is used to burn shisha3.
Meanwhile some people think that shisha smoking is not addictive because water which is used in pipe can absorb nicotine. However, not whole nicotine is absorbed by water, only a small amount of nicotine is absorbed but the amount which is not absorbed is enough to cause addiction of shisha3. Nicotine reaches the brain just after being inhaled and this is the reason due to which shisha becomes addictive even after its few sessions. Another reason of addiction is the unpleasant withdrawal feelings such as headache, fatigue or depression11.
Shisha smokers are prone to health hazards as compared to cigarette smoking. One session of shisha inhaled is same as the person who inhales 100 cigarettes per day. One puff of shisha smoke is equal to the whole cigarette. Shisha smoking causes many diseases such as respiratory diseases, heart diseases and cancer3.It is proved by research that people who are shisha smokers have high percentage of chronic Bronchitis than cigarette smokers. The heavy volume of smoke can cause chemical irritation leading to the irritation or inflammation in the lining of nasal passages and may cause asthma11. Shisha smoking in pregnant female can cause problems to fetus12. Shisha is harmful for active smokers as well as for passive smokers. Both are at high risk of health problems.
A study conducted by Al-Fayez et al in Saudi Arabia on both shisha and cigarette smokers, showed in both genders, significant decrease in the mean value of FVC when FEV1 compared with controls, regardless of gender, and support our results, the risk was in both genders higher for shisha smokers. That could be justified by the reality that the exact measurement of the increased amount smoked in our study was due to more subgroups. The Saudi study divided shisha smokers into mild if they smoked 2 sessions/day and heavy if they smoked more. They were unsuccessful to examine those who smoke shisha only a few times per week13.
The shisha smoking in women causes greatly extra CBH than cigarettes for the same amount or period (p value < 0.001). At most progressive the phlegm and cough during comparatively three months is defined as chronic bronchitis. The CBH is only critical definition. FEV1 and FEV1/FVC could be normal and their variation means the incident of COPD13.
Shisha smoking conveys respiratory infections, particularly tuberculosis, by passing the tube from person to person, however it has a less carcinogenic effect.
Shisha is now commonly a new tobacco universally and severely damaging the indoor air quality and includes severe health risks10. Shisha smoking hold equivalent similar health risks as smoking cigarettes because it generates large amount of toxic ultrafine particles7. In the advance study, we resolved the outcome of Shisha smoking on lung functions and Fractional Exhaled Nitric Oxide (FeNO). In the advance study between Saudi young adults, we constitute a notable decline in lung function parameters FEV1, FEV1/FVC%, FEF-25%, FEF-50%, FEF-75%, FEF-75-85% in Shisha smokers comparable to their similar control group. In Shisha smokers compared to control group there was also a notable decline in the Fractional Exhaled Nitric Oxide (FeNO)14.
Shisha smoking causes natural alteration in place causing obvious health problems. Likewise, Hawari et al. performed a study on shisha tobacco smokers, they originate that forced expiratory flow above the middle half of the forced vital capacity (FEF50%) decreased between shisha tobacco smokers with mean age 20.4 years in shisha smokers comparable to their matched group, we create a notable decline in lung function parameters FEV1, FEF-25%, FEF-50%, FEF-75% and FEF-75-85% as similarly shown in the present study15.
The decline of FEV1 coupled with shisha smoking is critically proportional. A notable decline in FEV1 offers its indication as a risk factor for obstructive disease relevant with shisha smoking. This is invariable with the conclusion of a direction toward decline in FVC and FEV1/FVC between shisha smokers. These conclusions indicate possible role of shisha smoking in the progress of COPD15.
Tobacco has been used for smoking for centuries. Tobacco plant was first grown in America in 17th century and from that day tobacco has been used in various forms. One form of tobacco used in cigarette. In 1885 Washington Duke from North Carolina invented cigarette. Cigarette is a form of tobacco leaves rolled in fine paper. In 1883 James Bonsack invented a cigarette manufacturing machine and started his own business naming “The American Tobacco Company”. This company was first to produce cigarette mechanically16.
In U.S, prevalence of cigarette smoking is 20.5% in men and in women it is 15.6%among which 18- 24 years adult age person the rate is 17.3%. In 25-44 years old people, the prevalence rate is 21.6%. In age 45-64 rate is 19.5% and 65 years above is 8.9%17.
According to WHO prevalence of cigarette smoking in Pakistan is greater in males than females. It was 17.2% in male and 1.5% in female. Among youth it is 9.9% in male and 1.0% in female18.
Cigarette and other mode of tobacco- counting cigar, pipe tobacco and chewing tobacco all these consist of obsessive drug nicotine. A classic smoker will take 10 puff on a cigarette over a cycle of about 5 minutes that a cigarette is lit. Therefore, a person who smokes about 1 packet that is 25 cigarettes regularly receives 250 “hits” of nicotine1.
Smoking tobacco contains more than 60 known cancer causing chemicals. The components used in tobacco smoking are Tar, Carbon monoxide, hydrogen cyanide and other free radicals. These components are the most health damaging components. Tar is brown colored sticky substance that is deposited on teeth, nails or lung that can further result in cancer. Tobacco cigarette also contain metals that are very hazardous to health e.g.
Arsenic, Cadmium and zinc. Smoking can cause damage to any organ of body as well as system of body. It affects musculoskeletal system of the body by reducing bone density and tightening of muscles. It affects sexual organs of both male and female. In females there are menstrual irregularities and the risk of cancer in cervix is increased whereas in males it causes damage and this damage results in low sperm production, impotence or damage to vessels of penis. In pregnant females smoking causes low body weight of fetus which can further effect the growth of the baby18.
Smoking also damages the cardiovascular system of the body by causing stroke and coronary heart diseases, narrowing of vessels. Smoking also affects the respiratory system of the body by causing lung cancer and COPD. 80% to 90% of people dying with COPD are those having COPD due to smoking. If a person is already suffering from asthma, smoking can trigger effects of attack or make a worse attack18. Smoking can cause cancer all over the body. Prolong use of smoking can cause fractures, osteoporosis, gangrene which may result in amputation18.
Cigarette smoking causes a number of chemicals enter in the lungs. Smoking influences the lungs and airways significantly. Cigarette smokers have several breathing problems. These problems may be disturbing as cough or may be life threatening as emphysema and cancer19. Damage to the lung by smoking doesn’t depend on age. Cigarette smoking destroys the lung of people of every age. Function of lungs gets worse as long as person smokes. The major health problem caused by smoking affects the nicotine delivery system, airways, blood vessels and lungs in the human respiratory system. Cigarette smoking upsets this balanced process due to damage of the respiratory system20.
Expecting women who smoke cigarette have an elevated risk of miscarriage, stillborn and immature infants or a child with low birth weight. Maternal smoking also affects child’s learning and behavior problem. Study shows that if the pregnant women smoke more than 1 packet of cigarettes doubles the danger that the concerned child will become obsessed to tobacco if he starts smoking1.
In 19th century first Spirometer was invented by a London surgeon, John Hutchinson. Spirometer is used for evaluating exhaled and inhaled lung volumes, and shows how effectively lungs can work21. It is adopted for airflow hurdle for patients having respiratory manifestations but cannot be used for any respiratory problems. On the other hand another purpose for Spirometer is monitoring disease furtherance as well as readjustment and treatment progression. Despite of the fact that Spirometer explains nature, pattern along with hardness of lung disease. It fails to give any long term prognosis or life quality21. Spirometer test is commonly protective for all subjects but at times the subject may struggle with a sense of lightheadedness or fainting22.
There are two types of Spirometer: 1) those that record the amount of air exhaled or inhaled within a certain time (volume) 2) Those that measure how fast the air flows in or out as the volume of air inhaled or exhaled increases (flow) 22.
In this study we aim to use incentive Spirometer to calculate inspiratory reserve volume which is defined as” the amount of that you inhale and exhale during normal breath”. Tri-balls incentive Spirometer is a flow-oriented device, provided with a ball that indicates patient’s inspired volume. It is used to help strengthen respiratory musculature and to help restore and maintain lung capacity by encouraging a slow, deep breathing.
Three color-coded balls in each chamber provide a visual incentive for the patient. Air flows into single channel, when it passes through the chamber; it raises each of the three balls depending on the flow inhaled per second23.
It was said that hazards of shisha is less than cigarette smoking but it was the misleading concept. Dr. Ahmed Al Mullah, Consultant physician and Head of smoking cessation clinic claimed that smoking shisha can be harmful more than ten times than cigarette smoking, according to a report in Peninsula23.
Eventually the shisha smokers are at more risk than cigarette smokers. As shisha contains approx. 36 times more tar than cigarette13. So, it resulted as lung volume specifically inspiratory reserve vol. is more decreased in shisha smokers than in cigarette smoker.
METHODOLOGY
Study Settings
The study will be organized in Ziauddin College of Physical Therapy, Ziauddin College of Nursing, Ziauddin Hospital (North Nazaimabad) Karachi, Pakistan.
Study Design
Cross sectional study design. Sampling Technique Probability sampling (stratified)
Inclusion Criteria
- People who precisely smoke cigarette.
- People who specifically smoke shisha (water pipe).
- Both genders are counted (male and female).
Exclusion Criteria
- Subjects with the history of anemia, bronchial asthma, diabetes mellitus, chronic obstructive pulmonary diseases, drug addiction, and malignancy.
- People who perform vibrant exercises frequently.
Procedure
50 participants were included in this study they were given an assessment form to be filled after taking an informed consent.
After that, one by one all subjects performed Spirometer test (Pulmonary function test) in which researcher asked the participants achieve sitting position which is more comfortable for patient than lying down on bed or standing position. Do not bend your head forward or backward. Firstly, place Spirometer pipe into the mouth. Then the patient is advised to take wide breath as much as they can through their mouth, while their nose is closed by nose clip and when the person is not able to hold further more than ask him to remove mouthpiece and then exhale. We noted the Inspiratory volume by the level of ball raised (600, 900, 1200cc) and as well as no. of second’s patient hold the ball or balls. Test was immediately stopped if person felt any kind of dizziness, headache, shortness of breath, chest pain. When the test was completed, researcher calculated tidal vol. through the formula that is “inspiratory reserve vol. = levels of ball raised X no of seconds hold”.
Data Collection
Data is collected through questionnaire which includes 8 questions based on effects of shisha and cigarette smoking on lung capacities specifically inspiratory reserve volume by using spirometer. After collecting the data through questionnaire lung capacity was measured by the help of spirometer.
Data Analysis Strategies
The Data was analyzed through SPSS.16, in a cross tabulation and value of p was obtained by t table.
Ethical Consideration
The Research is approved by the ethical committee of Ziauddin University. Participant’s demographic information was kept confidential and is only accessed by the authorized person. In consonance with ethical consideration all information related to attendant was also kept confidential.
RESULTS
The total no of respondents was 50 in which 25 were shisha smokers and 25 were cigarette smokers. Result was obtained by the help of SPSS 16 through “independent variable T- test”.
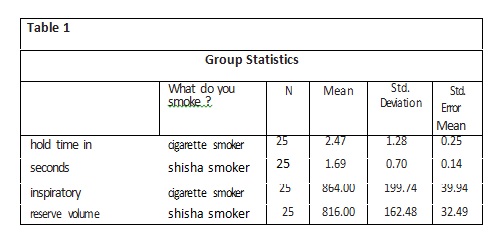
The mean holding time of cigarette smokers was 2.4728 and of shisha smokers was 1.6992. This shows that the mean holding time of shisha smoker is less than cigarette smokers.
Similarly, the mean inspiratory reserve volume of cigarette smoker was 864 and of shisha smoker was 816 which means inspiratory reserve volume is more in cigarette smokers as shown in table1.
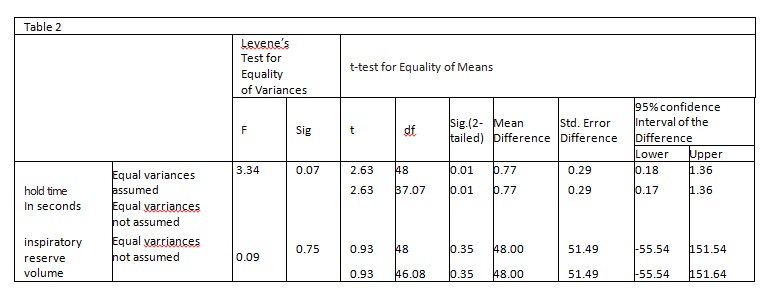
Hence, according to table 2, IRV has shown a significant decline in shisha smokers than in cigarette smokers.
DISCUSSION
Incentive spirometer is a device that is used to evaluate air that is normally inhaled and exhaled by the person. In our study we use 3 balls incentive spirometer which is used to evaluate and assess lung volume; we concisely focused on to measure “inspiratory reserve volume (IRV) “which is defined as the complemental air that is inhaled after a normal inspiration18.
Spirometer consist of 3 chambers, a color coded balls, plastic tube with 12mm OD with connecter and a mouth piece. Color coded balls indicate flow rate which is 600cc/sec, 900cc/sec and 1200cc/sec that helps to find out IRV through a formula which is level of ball raised and no of sec hold18.
Tobacco smoking is very harmful to health but it’s common in every society. Content of cigarette can cause dangerous diseases that can be fatal such as cancer. Smoking can really take your breath aside within second’s causing two to three times gain in airway resistance. Cigarette smoke content (tar) will count airway resistance as it covers the lung reducing recoiling capacity of airway sac that leads to reduced amount of oxygen consumption22. One study reveals marked deterioration in pulmonary function values in advanced age that was more noticeable than in non- smoker13.
A study was conducted in Saudi Arabia 49.7% people disclosed that Shisha is less harmful than cigarette, 60.5% people suppose that unhealthy substance was cleared by filtration through water whereas 67.8% people think that shisha is not addictive23. People suppose that shisha has herbal ingredients and so it is less dangerous than cigarette contrary to this perception tar nicotine and other toxic materials are present in shisha as they are in cigarettes. It’s a myth that shisha smoking is not harmful to the lungs but actually it is violent to the lungs because even its filter contain carcinogen causing destruction in the lung. Commonly shisha smokers believe that shisha is less toxic in comparison to cigarette. As compared to cigarette, shisha is acceptable in our society and is considered as less harmful than cigarette but actually it is more dangerous than cigarette smoking24.
A study was carried out to separate meta-analysis in which the effect of shisha smoking was compared with non-smokers and cigarette smokers resulting in significant reduction of FEV1/FVC between shisha smokers and non-smokers but there was no convincing difference amount in shisha smokers16.
Person who exercises to gain peak achievement their heart, lungs and muscle need copious amount of oxygen. But when the person smokes tobacco carbon monoxide attached to red blood cells replaces oxygen and prevent from reaching a sufficient amount of oxygen to the muscles. Reduced quantity of oxygen will reduce their physical capacity. People think that if they take exercise the tobacco smoking will not harm however it is wrong people who do exercise are less exposed to the damage of lungs and airways by tobacco smoking. On the other hand the person who exercises daily has less compromised lung capacities then that of person who exercises occasionally. In addition to this our study also show the same result as there is significant reduction in inspiratory reserve volume in the person who don’t exercise than that of person who are involved in extra physical activities than the normal lifestyle24.
The purpose of the study was to yield the comparison virulent exposure related to both kinds of smoking. Related to cigarette smoking shisha smoking was having same chemicals in addition with more exposure to smoke therefore smoking related health risks are similar or slightly more in shisha smokers25.
Another study was carried out using questionnaire and spirometry conducting that risk of COPD is markedly higher in shisha smokers than in cigarette smokers. 11.75% identified as shisha smokers and 95% cigarette smokers were prone to chronic bronchitis26.
Shisha smoker as well as cigarette smoking will give same effects on the ventilatory function in both genders male and female elevating the exposure of developing obstructive air passage disorder with shisha smokers being at more advanced hazards13.
Shisha smoking is a worldwide health problem. According to the survey, it will kill 10 million people yearly in the next 20-30 years. It is estimated that 70% among these deaths will occur in the developing countries. Mostly the research, awareness program and policies are being focused on cigarette smoking whereas public in developing regions smoke tobacco by water pipe method. Almost 75% of the water pipe smokers are from secondary schools, colleges and universities. A study conducted in Lebanon showed 82.7% of the shisha smokers were from intermediate or higher education group. Stress is one of the causes of smoking. In a study, it is revealed that low education and low incomes was a great factor of early start and prolong smoking27.
Out of the studies shows that the pulmonary function deterioration was serious in water pipe plus cigarette smoker which composed of 52%, at the same time in water pipe smoking it composed of 48%. Water pipe smoking leads to compelling decline in lung readiness as well as elevation in respiratory symptoms among male adult water pipe smokers. Lung function test guidelines had serious decline in water pipe smoker as well as cigarette smoker immediate water pipe and tobacco smoking cessation push is greatly recommended28,29.
The study we conducted concede that both type of tobacco smoking that is shisha and cigarette smoking are not good for health and cause adverse effect to lungs and airways as well as it deteriorate lung capacities.
Our study is based on the comparison of Inspiratory reserve volume (IRV) effects of both types of smokers. Cigarette smoking cause great decline in IRV on individuals’ lungs.
There is a positive perception about shisha smoking in our society. Shisha is regarded as less harmful in contrast to cigarette28. Even some communities believe that narghile have adverse effect on health. However in our study we witnessed that on spirometer, shisha smoker were having decline in hold time and therefore IRV were also dropped. In opposition to cigarette smoker the fall in IRV shisha smoker was larger.
CONCLUSION
As far as deciding between health concerning effects of shisha and cigarette smokers, the shisha smoking effects are same as cigarette smoking. IRV is disturbed by both means of smoking but shisha smoking has more potential risks.
Shisha smokers are more prone to carbon and smoke intake so the physician should advise that contents of shisha and cigarette are same therefore health risks are similar for each category of smoker. Effects of water pipe smoking are alike of deep inhalation of cigarette smoke. Tobacco based shisha and herbal shisha are both toxic to health because smoke from both type contain carbon mono oxide and other toxic agents. These known toxic chemicals are cause of pulmonary cancer and other pulmonary diseases such as COPD. Smoking hookah exposes an individual to more smoke than cigarette smoker. Use of nicotine in shisha makes it addictive as it is totally wrong believing shisha is not addictive. Regular shisha smokers are addicted to it and they become tobacco dependent. Beside this tobacco smoking is cause of low birth weight infants whose mother smoke during pregnancy28. Smoking has considerable health concern problem so public must be aware of its hazards. People who think that shisha is not harmful must be informed about its hazards. Regrettably many of the tobacco control programs exclude water pipe smoking. Worldwide awareness is required and strong rules to control water pipe. Clinicians can persuade public by performing simple spirometry test. Research can help the physician with data or convincing patients about the detrimental effects in lung capacities.
More research is needed that is related to water pipe smoking risk with high quality studies between shisha smokers and its clinical outcome13.
Government should take steps for the awareness about hazards of shisha. Shisha cafes should have prominent notice that” shisha kills just as we have on cigarette. Advertisement for the awareness should be on-air on official television channels.
REFERENCES
[1] Drug facts: cigarettes and other tobacco products [internet]. [Updated 2014, cited 2015]. Available from: https://www.drugabuse.gov/publicat i o n s / d r u g f a c t s / c i g a -rettes-other-tobacco-products/
[2] Global Youth Tobacco survey Collaborating Group. Differences in worldwide tobacco use by gender: finding from global youth tobacco survey. J Sch Health. 2003;73:207-15
[3] British Heart Foundation. Shisha [internet]. [Updated 2014]. Available from: http://www.bhf.org.uk/heart-health/prevention/smoking/ shisha.aspx
[4] Israel E, EL-Setouhy M, Gadalla S, AOUN el SA, Mikhail N, Mohamed MK. Water pipe (sisha) smoking in cafes in Egypt. J Egypt Soc Parasitol. 2003;33(3):1073-85.
[5] Varsano S, Ganz I, Eldor N, Garenkin M. Water-pipe tobacco smoking among school children in Israel: frequencies, habit, and attitudes. Harefuah. 2003;142:736-41.
[6] Asfar T, Ward KD, Eissenberg T, Mazaik W. Comparison of patterns of use, beliefs, and attitudesrelated to water pipe between beginning and established smokers. BMC Public Health 2005;5(9)
[7] Memon A, Moody PM, Sugathan TN, el-Gerges N, al-Bustan M,al-Shatti A, et al. Epidemiology of smoking among Kuwaiti adults: prevelance, characteristics and attitudes. Bull WHO. 2000;78:1306-1315.
[8] Khan N, Siddiqui MU, Padhiar AA, Hashmi SAH, Fatima S, Muzaffar S. Prevelance, knowledge, attitude and practice of shisha smoking among medical and dental students of Karachi, Pakistan. J Dow Uni Health Sci 2008;2(1):3-10
[9] Anjum Q, Ahmed F, Ashfaq T. Knowledge, attitude and perception of water pipe smoking (shisha) among adolescents aged 14-19 years. J Pak Med Assoc. 2008;58(6):312-317
[10] Alam SE. Prevalance and pattern of smoking in Pakistan. J Pak med Assoc 1998;48:64-6
[11] Kassem N. Side effects of shisha [internet]. [updated 2011, cited 2014]. Available from: http://www.livestrong.com/article/276983-immediate- reactions-to-hookah-smoking/
[12] Mohammad Y, Kakah M, Mohammad Y. Chronic respiratory effect of narguileh smoking compared with cigarette smoking in women from east mediterranean region. Int J Chron. Obstruct. Pulmon Dis. 2008;3:405-414
[13] Al-Fayez SF, Salleh M, Ardawi M, et al. Effects of sheesha and cigarette smoking on pulmonary functions of saudi males and females. Trop Geogr Med. 1980;40:115–23.
[14] Monn C, Kindler P, Meile A, Brandli O. Ultrafine particle emissions from water pipes. Tob. Control. 2007;16:390–393.
[15] Hawari FI, Obeidat NA, Ayub H, Ghonimat I, Eissenberg T, Dawahrah S, Beano H. The acute effects of water pipe smoking on lung function and exercise capacity in a pilot study of healthy participants. Inhal Toxicol. 2013;25:492–497.
[16] Raad D, Gaddam S, Schunemann HJ, Irani J, Jaoude PA, Honeine R, Akl EA. Effects of water pipe smoking on lung function: a systemic reviewand meta analysis. Chest. 2011;139(4):764-774
[17] A complete social history of cigarettes [internet]. Available from: http://www.datehookup.com/- consent-social-history-of cigarettes.htm
[18] World Health Organization. WHO report on the global tobacco epidemic, 2014 [internet]. Available from: http://www.who.int/tobacco/surveillance/ policy/country_profile/pak.pdf
[19] Smoking effects on your body [internet]. [updated 2014]. Available from: http://www.betterhealth. vic.gov.au/bhcv2/bhcarticles.nsf/pages/
[20] smoking_effects_on_your_body Smoking and your lungs [internet]. [cited 2014]. Avaiable from: http://www.upmc.com/patients- visitors/education/breathing/pages/ smoking-and-lungs.aspx
[21] Tobacco and cancer [internet]. [updated 2014]. Available from: http://www.cancer.org/cancer/ cancercauses/tobaccocancer/questionsaboutsmokingtobaccoandhealth/ question s-about-smoking-tobacco-and-health-how-tob acco-affects-lungs
[22] Smoking and tobacco use: health effects of cigarette smoking [internet]. Avaiable from: http://www.cdc.gov/tobacco/data_statistics/fact_sheets/health_effects/effects_cig_smoking /#adults
[23] Smoker [internet]. Available from: http://www.thefreedictionary.com/smoker
[24] Koubaa A, Trabelsi H, Masmoudi L, Triki M, Sahnoun Z, Zehgal KM, Hakim A. Water pipe tobaco and cigarette smoking: comparative analysis of the smoking effects on antioxidant status, lipid profile and cardiopulmonary quality in sedentary smokers Tunisian. Int J Pharmaceu Sci Invent. 2013;2(4):51-57
[25] Steps to staying well [internet]. Available from: h t t p s : / / m y . c l e v e l a n d c l i n – i c .org/ hea l t h / hea l t h y _ l i v i ng/ h i c _ – Steps_to_Staying_Well/hic_Dangers_of_SecondHand_Smoke/hic_Smoking_and_Physical_Activity
[26] Eissenberg T, Shihadeh A. Water pipe tobacco and cigarette smoking. Am J Prev Med.2009;37(6)518-523
[27] Al Mutairi SS, Shihab-Eldeen AA, Mojiminiyi OA, Anwar AA. Comparative analysis of the effects of hubble-bubble (sheesha) and cigarette smoking on respiratory and metabolic parameters in hubble-bubble and cigarette smokers. Respirology. 2006;11(4):449-455.
[28] Sugathan S, Daghir OM, Swaysy M. Socio-economic correlates of shisha or waterpipe smoking in Misurata, Libya. Int J Epidem. 2011;9(2):1
[29] Baiee HA, Mahmoud RI. Pulmonary function test for water pipe smokers and cigarette smokers in males in Al-Hilla City during the year 2014. Med J Babylon. 2014;11(4).1029-1036