
Dr. Keramat Ullah Keramat1*, Prof Dr. Muhammad Naveed Babur2
1*Helping Hand Institute of Rehabilitation Sciences, Datta Morr, Mansehra, KPK Pakistan![]()
2Professor, Isra Institute of Rehabilitation Sciences, Islamabad, Pakistan![]()
ABSTRACT
Background of the Study: The effects of novel set of interventions are known but their effects with respect to gender are not known. This study aim to determine the effects of novel set of interventions on shoulder range of motion in males and females with shoulder pathology.
Methodology: This study was of quasive experimental design. Thirty subjects of mean age (±SD) of 43. 23±10 years with shoulder pathology and restricted ROM were recruited. The major criteria for recruitment were 18-60 years of age. The general contraindications of manual therapy were the exclusion criteria. Shoulder functional movement and range of motion were the outcome measures.
Results: The mean %(SD) change for RUBB was 15.04±11.57for males and 14.49±10.44 for males. The change for RDBN was also significant (<0.00) from baseline and the % change in mean was 14.93±11.0 for males and 12.60±9.06 for females. The changes were well above the highly clinical meaningful difference (>0.8). It is further observed that the differences in gender were non-significant (P>0.05).
Conclusion: The pragmatic set of interventions affect both the genders equally and improve shoulder range of motion and functional movements. However, the results must be interpreted cautiously because of the inadequate sample size.
Keywords: Sports injury, Shoulder injury, Rehabilitation, Novel therapy, manual therapy, Gender difference.

Introduction
Shoulder painful conditions are common in both genders and overhead sports1. Among the disorder of the shoulder, Subacromial impingements (SAI) or adhesive capsulitis are the commonest. SAI constitutes 48-60 percent of shoulder disorders2,4. SAI is defined as the impingement subacromial bursa, biceps tendon (long head) between the acromion (superiorly) and greater tubercle of humerus (superiorly)5,6. In most of the diagnoses, the laceration/abrasion to the rotator cuff tendon from acromion- but the laceration also happens from the articular side to the tendon. The latter has been termed internal impingement7,9. Yet, disagreements exist about the causative factors, diagnosis, optimal rehabilitation strategies5. Several biomechanical factors are suspected that are associated as a cause of shoulder pain. Most of these factors are believed to be the precursors of shoulder pain10,11. Posterior capsular tightness- which itself is not causing any pain, is considered one of the major culprits12,14. The dysfunction of the serratus anterior and its various digitations are reported in association with shoulder dyskinesis and altered biomechanics15. Rotator cuff (RC) insufficiency has been studied extensively and considered a major factor in superior humeral translation during the overhead movement. It is evident from the latest reports that rotator cuff fatigue earlier to overcome the resistance from the tight posterior capsule10. The non-use or overuse of the shoulder, causes tightness in posterior capsul-uses capsule. The posterior capsule gets hypertropied as a results of repeated stress in overhead sports10,14. It is also reported that the stiff thoracic spine decreases the mobility of the scapula and thereby affect the shoulder range of motion16,19. Similarly, AC joint stiffness and tight pectoralis minor are common findings in association with shoulder pathology19,20. The clinical observation of reveals protracted shoulder, stoop posture and shoulder dyskineses21. Asymptomatic healthy athletes with the presence of these observation were followed prospectively and painful symptoms occurred from 9-24 months11. Manual therapy techniques are preferred for shoulder pathology. Numerous schools of thought and techniques exist. The novel set of manual interventions includes novel interventions and existing interventions and is based on emerging understanding of the mechanism of shoulder pathology. The current study reports the findings in male and female subjects with shoulder pathology.
Methodology
A Pretest-posttest quasive experiment designed was used. Seventeen male subjects against thirteen female subjects were studied. The inclusion criteria older age adults, restriction in shoulder ROM and Functional movement screening (FMS)’ grade 0 to 2. Subjects with shoulder instability, recent fractures, history of Ca and radiotherapy, osteoporosis, rheumatoid arthritis, long-term use of steroids, and grade 3 of FMS were excluded. Cancerous growth, chemotherapy and Pain associated with shoulder swelling, redness or cysts, rheumatoid arthritis patients and known osteoporosis. The study represents one of the objective of Ph.D. thesis. Ethical approval was granted by the IRC of the university. Patients were given written information and informed consent taken. The study protocols are registered on clinicaltrial.gov prior to commencement of the study.
Data Collection and Instruments
Cyriax’s systematic procedure of assessment was used22 which has been found highly reliable23 and used in the previous studies23. The assessment of participants involved taking demographic information, history of presenting complaint, past medical and surgical history, medications, psychosocial history and subjective history of the current shoulder pain. Questions were asked about the onset of pain, duration of symptoms, aggravating and relieving factor of pain, previous treatment, investigation and outcome. The objective examination stated from observation and includes the active ROM of neck on all planes, Active ROM shoulder, Passive ROM and end feel. Specia test such neer’s sign, Hawkin kenndy test and Isometric resisted tests for each of the muscle of rotator cuff and long head of the biceps were included. Strength and pain responses were recorded.
Outcome measuring tools
A digital inclinometer is a validated tool. Its external and internal rotation Cronbach’s alpha scores are 0.94 and 0.95 respectively24. It is useful in assessment of shoulder movements. It can be installed on android phones such as Samsung galaxy note 8. Secured via strape to the wrist, internal rotation, external rotation, flexion and abduction were measured. Its mean level of bias reported is 3.4 degrees against the gold standard and has been recommended for measuring shoulder range of motion25. A strape was used to fasten the phone to the wrist. The inclinometer reading was adjusted to zero at 90 degree of abduction for internal and external rotation on a Bobabth’s plinth. The subject remained seated on a chair during the measurement for abduction and flexion with forearm extended and phone straped to the wrist and in a mid-prone position.To measure the reach behind the back and down behind the neck, the unaffected side was used for reference reading during down behind neck (RDBN) and up behind the back (RUBB). The distance between the bony prominances of the hand in a fist position was used for measurement before and after the intervention. Four trained undergraduate students took the measurements before and after the intervention under the supervision of a senior physiotherapist.
Interventions
The pragmatic set included 6 interventions as follows
1–Pragmatic posterior capsular stretch (PPCS)13: The effectiveness of the pragmatic posterior capsular stretch in healthy subjected with restricted shoulder mobility and flexibility had been determined. The stretch is reported with more specificity and a large clinical effectiveness had been reported with the recommendation of its trial on subjected with shoulder pathology13.
2-Serratus anterior stretch (SAS)15: The novel SAS has been reported with profound results on the shoulder ROM with greater effects on RUBB and scapular mobility. The stretch was used as recommended15.
3-Rotator cuff facilitation (RCF)26: RCT techniques involve positioning the subject in supine lying with arm flexed as far as the subject can. Thumb slides unopen the belly of the subscapularis muscle and fingers in the infra spinatus muscle- while the subject actively flex the arm to the end range. A gentle sweep/effleurage/kneading through the thumb and fingers is administered over the belly of the muscles in the direction of their attachment on the scapula while the subject actively flexes his/her arm at the shoulder. RCF greatly influences the internal and external rotation in health subjects.
4-Acromioclavicular joint mobilization26: Acromioclavicular joint in sitting position of the subject is located by sliding the thumb laterally on the lateral end of the clavicle. Thumb is position behind the lateral end of clavicle and finger on the anterior margin of the lateral end of clavicle. The other hand is used to stabilize the acromion process. Gentle force is used to glide the clavicle anteriorly and posteriorly. Five to ten sweeps per minute are administered three to four times. The applied force is combined with deep breathing. The subject is asked to report discomfort and the applied force is adjusted.
5-Pectoralis minor stretch: The stretch is administered in a supine lying position. The stretch has been found effective in improving shoulder mobility after the restoration of shoulder kinematics27 and other hand placed in the middle of the chest with hypothenar eminence on the sternum. The posterior force was applied27on the shoulder girdle meanwhile an opposite force is applied to the sternum with hand. A two minutes duration of hold was used and combined with deep inspiration and hold.
6-Thoracic manipulation: Afterward, thoracic manipulation was performed by using the screw method. While the patient in prone lying over the pillow the physiotherapist crosses his/her extended arm, palpating the costeroverberal joint- one above the other and a manipulative force is applied at the end of expiration to each thoracic segment7. The manipulation has been reported with increased mobility of the shoulder. A well-trained and experienced physiotherapist, other than the principal investigator administered the session of PSI. Routine physiotherapy, which mainly inclusive of heat therapy was continued.
Results
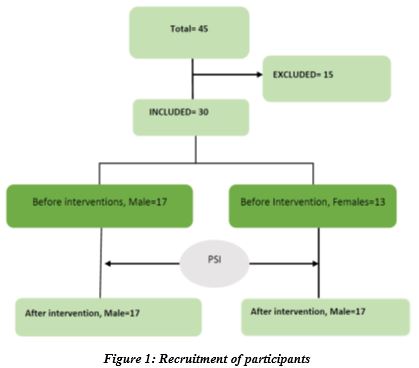
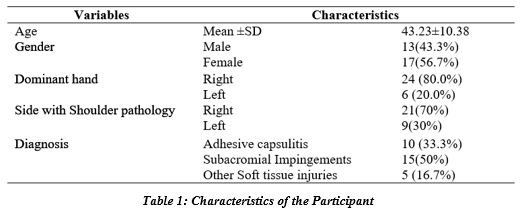
A total of 45 individuals were screened for eligibility. Subjects excluded were fifteen. Figure one shows the flow of participants. Out of 30 subjects, 13 were females and 17 were males. The mean age (±SD) of 30 subject was 43.23 (±10.38) years. The most common diagnoses were subacromial impingements (150%) and adhesive capsulitis10. The side of the shoulder pathology in majority of the cases (70%) was right side dominate hand. The demographics are summarized in table 1.
Detailed paired t-test statistics of the major outcomes of the PSI interventions before and after the first session of PSI are shown in table 2 for changes in two functional movements of RUBB & RDBN. RUBB improved significantly (p<.000). The mean % (SD) change for RUBB was 15.04±11.57for males and 14.49±10.44 for males. The change for RDBN was also significant from baseline and the % change in mean was 14.93±11.0 for males and 12.60±9.06 for females.
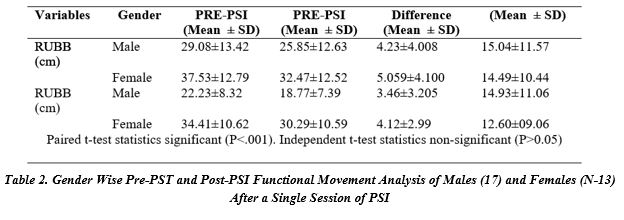
The changes were well above the highly clinical meaningful difference (>0.8). It is further observed that the gender differences were non-significant.
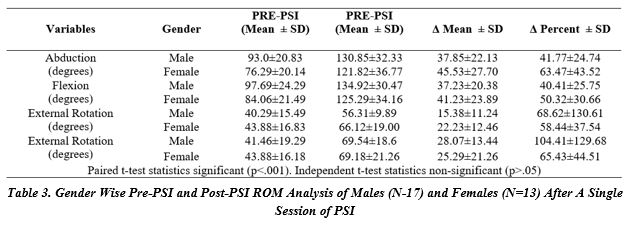
Table 3 shows descriptive statics of range of motion before and after the PSI and reveals a highly significant change from the baseline measures. A highly clinically meaningful difference (Cohen’D >0.8) were observed across changes in all shoulder ROMs. It ranged from twice to thrice. The baseline comparison of all the variables revealed non-significant difference- implying an equal match of both the genders. However, it is observed that the improvement in males and females was non-significant (P>0.05)- implying that the interventions affected both genders equally.
Discussion
The results reveal that a pragmatic set of interventions is useful for the improvement of shoulder range of motion in both males and females subjects with restricted shoulder mobility. The findings suggest that the PSI is useful in the correction of the biomechanics of the shoulder joint. The findings of the current report are consistent with the previous reports on the non-painful healthy shoulder where improvement in factional movements and shoulder range of motion has shown13,15,28. In contrast to the assumption that the intervention will affect both the genders differently since females being a more flexible and males being of a more rigid consistency of tissue- the current findings deny the assumption. However, unequal sample sizes, duration of symptoms and specific diagnosis and mean age of subjects may render the findings of the current study inconclusive. The interventions are cost-effective and require less time of the session and resources except that training from a qualified person of the intervention may be needed. The PSI interventions are beneficial in terms of time and cost-effectiveness unlike the other protocols recommended for painful conditions of the shoulder29, 30. Pekyavas & Baltaci (2016) compared four groups comprised of Kinesio Tapping, exercise, manual therapy and high-intensity laser therapy on patients with subacromial impingements. Four groups formed were exercise group (n=15), Exercise-Kinesio tapping group (n=20), Exercise-Kinesio tapping-Manual therapy group (n=16) and exercise-Kinesio tapping- Manual therapy- High-intensity Laser therapy group (n=19). Treatments were given 3 sessions per week for five weeks. The manual therapy approach used was scapular mobilization, glenohumeral mobilization, deep friction massage and proprioceptive neuromuscular facilitation. Their outcome used in their study in a group where four the interventions were combined, were significant but less clinical meaning full in terms of pain, disability, and shoulder ROM. The outcome of their study was the result of 15 sessions extended over 5 week’s period. Therefore, the current study is associated with superior outcome in 1 sessions of treatment and normative values of shoulder ROM were achieved31. The improvement in the current study was due to the effectiveness of a set of interventiona that is pragmatic and evolved from the emerging evidence10 regarding the mechanism of indirect shoulder pathology such as subacromial impingement. One of the important interventions in the PSI is pragmatic posterior capsular tightness and measure contribution in the improvement of shoulder ROM is probably due to this manoeuvre14.The improvement in pain and shoulder related disability suggest that the intervention targets the key area areas which are associated with shoulder dysfunction and induces a healing environment. The sample chosen in this study included subjects with a diagnosis of adhesive capsulitis (n=10), in which the intervention is effective but not as much as it would be in extra-articular pathology since extra-articular structures are targeted with PSI. Patients of adhesive capsulitis mostly have co-morbidities and the aetiology is usually of primary nature which originates from within the joint (synovial membrane lesion) and the PSI. A majority (70%) of the side with shoulder pain was the right side and the dominant hand was also the right side in the majority of the subjects (80%). This implies that the most active shoulder is vulnerable to shoulder pain due to repetitive use. The current protocols are recommended for further studies of randomized control trial on shoulder specific diagnosis, duration of shoulder symptoms, and shoulder pain with primary aetiology. Studies on PSI for the prevention of shoulder pain are also recommended. The current study was exploratory in nature and the results cannot be generalized. Furthermore, the PSI evolved over the last 10 years and the therapist who administered the interventions was trained by the principal author.
Conclusion
A pragmatic set of interventions is effective in both the genders equally. However, the results must be interpreted cautiously since the number of male and female subjects was unequal, specific diagnosis different and duration of symptoms not accounted for.
AUTHORS’ CONTRIBUTION:
The following authors have made substantial contributions to the manuscript as under:
Conception or Design: Dr. Keramat Ullah Keramat
Acquisition, Analysis or Interpretation of Data: Prof Dr. Muhammad Naveed Babur
Manuscript Writing & Approval: Prof Dr. Muhammad Naveed Babur, Dr. Keramat Ullah Keramat
All authors acknowledge their accountability for all facets of the research, ensuring that any concerns regarding the accuracy or integrity of the work are duly investigated and resolved.
ACKNOWLEDGEMENTS: We thanks all the participants in this study.
INFORMED CONSENT: Written Informed Consent was taken from each patient.
CONFLICT OF INTEREST: The author (s) have no conflict of interest regarding any of the activity perform by PJR.
FUNDING STATEMENTS: None declared
ETHICS STATEMENTS: The study has been approved by the Ethical Board of University.
References
- Singh S, Gill S, Mohammad F, Kumar S, Kumar D, Kumar S. Prevalence of shoulder disorders in tertiary care centre. Int J Res Med Sci. 2015;3(4):917-20.
- Hassan Shaheen AA, Gillani SA, Raza M, Waqas M. Frequency of shoulder pain among overhead throwing athletes. Rawal Medical Journal. 2020;45(1).
- Shabbir M, Rashid S, Umar B, Ahmad A, Ehsan S. Frequency of neck and shoulder pain and use of adjustable computer workstation among bankers. Pakistan journal of medical sciences. 2016;32(2):423.
- Van der Windt D, Koes BW, de Jong BA, Bouter LM. Shoulder disorders in general practice: incidence, patient characteristics, and management. Ann Rheum Dis. 1995;54(12):959-64.
- Dhillon K. Subacromial impingement syndrome of the shoulder: a musculoskeletal disorder or a medical myth? Malaysian orthopaedic journal. 2019;13(3):1.
- Neer CS. Impingement lesions. Clinical Orthopaedics and Related Research (1976-2007). 1983;173:70-7.
- Giaroli EL, Major NM, Higgins LD. MRI of internal impingement of the shoulder. American Journal of Roentgenology. 2005;185(4):925-9.
- Heyworth BE, Williams RJ. Internal impingement of the shoulder. The American journal of sports medicine. 2009;37(5):1024-37.
- Mihata T, Gates J, McGarry MH, Neo M, Lee TQ. Effect of posterior shoulder tightness on internal impingement in a cadaveric model of throwing. Knee Surgery, Sports Traumatology, Arthroscopy. 2015;23(2):548-54.
- Keramat UK. Conservative treatment preferences and the plausible mechanism of Neer’s stage 1 of shoulder impingement in younger people. JPMA The Journal of the Pakistan Medical Association. 2015;65(5):542.
- Hickey D, Solvig V, Cavalheri V, Harrold M, Mckenna L. Scapular dyskinesis increases the risk of future shoulder pain by 43% in asymptomatic athletes: a systematic review and meta-analysis. Br J Sports Med. 2018;52(2):102-10.
- Land H, Gordon S, Watt K. Clinical assessment of subacromial shoulder impingement–Which factors differ from the asymptomatic population? Musculoskeletal Science and Practice. 2017;27:49-56.
- Keramat KU, Babur MN. Pragmatic posterior capsular stretch and its effects on shoulder joint range of motion. BMJ Open Sport & Exercise Medicine. 2020;6(1):e000805.
- Takenaga T, Sugimoto K, Goto H, Nozaki M, Fukuyoshi M, Tsuchiya A, et al. Posterior shoulder capsules are thicker and stiffer in the throwing shoulders of healthy college baseball players: a quantitative assessment using shear-wave ultrasound elastography. The American journal of sports medicine. 2015;43(12):2935-42.
- Keramat KU, Babar MN. Serratus Anterior Stretch: A Novel Intervention and Its Effect on the Shoulder Range of Motion. Journal of Sport Rehabilitation. 2021;1(aop):1-4.
- Barrett E, O’Keeffe M, O’Sullivan K, Lewis J, McCreesh K. Is thoracic spine posture associated with shoulder pain, range of motion and function? A systematic review. Man Ther. 2016;26:38-46.
- Haik MN. Shoulder Impingement: Short-term effects of a thoracic spine manipulation and a systematic review of physical therapy strategies. 2015.
- Norlander S, Gustavsson B, Lindell J, Nordgren B. Reduced mobility in the cervico-thoracic motion segment–a risk factor for musculoskeletal neck-shoulder pain: a two-year prospective follow-up study. Scand J Rehabil Med. 1997;29(3):167-74.
- Borstad JD, Ludewig PM. The effect of long versus short pectoralis minor resting length on scapular kinematics in healthy individuals. J Orthop Sports Phys Ther. 2005;35(4):227-38.
- Rosa DP, Borstad JD, Pogetti LS, Camargo PR. Effects of a stretching protocol for the pectoralis minor on muscle length, function, and scapular kinematics in individuals with and without shoulder pain. J Hand Ther. 2017;30(1):20-9.
- Kibler WB, Thomas SJ, Sciascia AD. Scapular Position and Motion in Shoulder Function and Shoulder Injury. Mechanics, Pathomechanics and Injury in the Overhead Athlete: A Case-Based Approach to Evaluation, Diagnosis and Management. 2019:151.
- Kesson M, Atkins E. Chapter 5 – The shoulder. Orthopaedic Medicine (Second Edition). Edinburgh: Butterworth-Heinemann; 2005. p. 119-76.
- Pellecchia GL, Paolino J, Connell J. Intertester reliability of the Cyriax evaluation in assessing patients with shoulder pain. Journal of Orthopaedic & Sports Physical Therapy. 1996;23(1):34-8.
- Smith AB. Validation of a smartphone application for measuring shoulder internal rotation and external rotation range of motion with intra-rater reliability. 2016.
- Boissy P, Diop-Fallou S, Lebel K, Bernier M, Balg F, Tousignant-Laflamme Y. Trueness and minimal detectable change of smartphone inclinometer measurements of shoulder range of motion. Telemedicine and e-Health. 2017;23(6):503-6.
- Ullah KK, Babur MN. Comparison of the effectiveness of novel intervention on restricted range of motion of shoulder in young healthy subjects. Pakistan Journal of Medical Sciences. 2021;37(5).
- Muraki T, Aoki M, Izumi T, Fujii M, Hidaka E, Miyamoto S. Lengthening of the pectoralis minor muscle during passive shoulder motions and stretching techniques: a cadaveric biomechanical study. Phys Ther. 2009;89(4):333-41.
- Keramat KU, Babur MN. Rotator Cuff facilaition technique effective in improving shoulder range of motion: Under review. J Physiother. 2020.
- Pellegrini A, Tonino P, Salazar D, Hendrix K, Parel I, Cutti A, et al. Can posterior capsular stretching rehabilitation protocol change scapula kinematics in asymptomatic baseball pitchers? Musculoskelet Surg. 2016;100(1):39-43.
- Tejera-Falcón E, del Carmen Toledo-Martel N, Sosa-Medina FM, Santana-Gonzalez F, Gallego-Izquierdo T, Pecos-Martín D. Dry needling in a manual physiotherapy and therapeutic exercise protocol for patients with chronic mechanical shoulder pain of unspecific origin: a protocol for a randomized control trial. BMC Musculoskelet Disord. 2017;18(1):400.
- Gill H, Gustafsson L, Hawcroft L, McKenna K. Shoulder joint range of motion in healthy adults aged 20 to 49 years. Br J Occup Ther. 2006;69(12):556-61.
The Ziauddin University is on the list of I4OA, I4OC, and JISC.
This is an open- access article distributed under the terms of the Creative Commons Attribution License (CC BY 4.0).