
Vrushali Shety1*, Asma Hamid2
1*Rehabilitation Manager, Proclaim Care Ltd. Registered In Hamilton, Glasgow Canada![]()
2Vice Principal /Assistant Professor, Sindh Institute of Medical and Allied Sciences, Karachi, Pakistan![]()
Abstract
Objective: The study was designed to estimate the prevailing percentage of Carpal Tunnel Syndrome (CTS) using Boston Carpal tunnel syndrome questionnaire (BCTSQ) in the dexterous population and to assess its severity.
Study Design: This was a Cross-sectional survey.
Study Settings and Participants: The study setting was Karachi where 226 Dexterous workers including; musicians, typist, dentists, butchers office workers, working for more than 1 year were recruited using non-probability convenience sampling.
Outcome Measures: Boston Carpal Tunnel Syndrome Questionnaire.
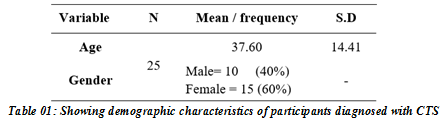
Results: This study enrolled 226 participants, 140 (61.9%) of which were males and 86 (38.1%) were females with mean age of 34.05±10.93. Out of the total 25 were diagnosed with CTS in which, 10 (40%) were males and 15 (60%) were females with mean age of 37.60±14.41. Hence, the prevalence of CTS among dexterous population was found to be 11.06%.
Conclusion: The results of our study revealed that CTS is a prevalent neuromuscular disorder among dexterous population. The severity level varies among the population. More epidemiological studies are required to get the approximate value to promote ergonomic awareness.
Keywords: Carpal tunnel syndrome, compression neuropathy, entrapment neuropathy, median neuropathy, dexterous population, demographical and genetical.

Introduction
The unwaveringly increasing prevalence of Carpal Tunnel Syndrome (CTS) in the workplaces has resulted in labelling it as the next eppandemic1. According to the National Institute of Neurological Disorders and Stroke, CTS is one of the most prevalent and well-known entrapment neuropathies reported in dexterous workers2 accounting for 90% of all neuropathies globally3. In the US, CTS has a yearly occurrence of 1 to 3 people for each 1000, and a predominance of 50 for every 1000, with approximately similar findings in most developed countries4.
CTS is an expensive upper extremity musculoskeletal disorder, having an annual estimated cost of beyond 2 billion dollars5. It is a neuropathy where the compression of the median nerve occurs which travels through the wrist’s carpal tunnel6. One of its manifestations is paresthesia on the first three digits and deep aching pain in the wrist and hand that limits the activities of an individual and restricts his participation7. Along with median nerve dysfunction somatosensory inference is also altered that impacts the motor performance and sensorimotor integration of an individual hence impeding dexterous manipulation and force distribution at the level of fingers8.
CTS has been found to be associated with numerous epidemiological factors including; vocational (dexterous), social, demographical and genetical9. However, the incidence of injury pertaining to dexterous causes is the highest among rest. On average 18% of workers develop CTS in the USA and leave their jobs within 18 months10. Similarly, in India 17.5% of CTS is developed during vocational training in dexterous population11. As reported by literature, the most commonly affected dexterous population includes; dentist, musicians, office, and industrial workers6, 12, 13, 14, 15, 16. However, literature also advocates a reduction in CTS severity and prevalence after implementation of ergonomical modulation17,18, 19, 20.
In Pakistan, epidemiological studies on the prevalence of musculoskeletal disorder are limited with little or no awareness of ergonomics guidelines for dexterous and general population leading to dysfunction and disability in a long run among them. Therefore, this study aims to estimate prevalence of CTS and to assess its severity among dexterous population.
Methodology
Target Population
Dexterous workers included in this research are all those who are musicians, typist, dentists, butchers and office workers, working for more than 1 year.
Study Design
This was a cross sectional design.
Duration of Study
January -May 2022.
Sample Size
A sample of 264 was determined utilizing open EPI , with a populace size of a million, keeping Confidence Interval (CI) 95%, frequency 50%and 7% bound of error.
n = [DEFF*Np(1-p)]/ [(d2/Z21-α/2*(N-1)+p*(1-p)]
Sampling Technique
Non-Probability Convenience Sampling
Inclusion Criteria
- Dexterous workers with working experience of a minimum of 1 year.
- Both male and female age between 20-60 years.
Exclusion Criteria
- People who were unwilling to participate in the study or have less than one year of experience.
- Diagnosed diabetes (neuropathic) endocrinological patients.
- Pregnant women.
Data Collection Procedure
A total of 226 participants were approached from different districts of Karachi including; hospitals, offices, music studios and butcheries. After recruitment of the participants, brief introduction of research study, its procedure, pros, and cons were explained. Informed consent was obtained from each participant and complete autonomy and confidentiality was provided. That data collection was carried out in two steps. In the first, the participants were comfortably seated and phalens test was administered for the confirmation of CTS. In the second step, Boston carpal tunnel syndrome questionnaire was administered to assess the severity and functional status of patients. The participants were also asked if they were aware of carpal tunnel syndrome or had previously been diagnosed with it.
Data Collection Tool
Boston Carpal Tunnel Syndrome Questionnaire (BCTQ).
The Boston Carpal Tunnel Syndrome Questionnaire (BCTQ) is designed to evaluate the symptoms in people who have CTS and is based on subjective assessment. In the context of extensive research, BCTQ has greater accuracy than any other comparable tool in determining the severity of CTS. For both the Functional Status Scale and the Symptom Severity Scale, the Cronbach’s alpha is 0.93, indicating high internal consistency with an interclass correlation coefficient 0.8 for both measures, and the test-retest reliability is also quite high. The Symptom Severity Scale’s coefficient of repeatability for BCTQ is 0.80; whereas for the Functional Status it is 0.6821.
Data Analysis Strategy
SPSS 2.0 was used to analyze the data. Descriptive statistics were used to analyze the demographic information and prevalence through frequency and formula.
Results
This study enrolled 226 participants, 140 (61.9%) of which were males and 86 (38.1%) were females with mean age of 34.05±10.93. Out of 226 participants 25 were diagnosed with CTS in which, 10 (40%) were males and 15 (60%) were females with mean age of 37.60±14.41. the details are shown in table 1.
The prevalence of CTS among dexterous population was found to be 11.06% by using the following formula;
![]()
The functional status and severity of Carpel tunnel syndrome was determined using Boston Carpel Tunnel Syndrome Questionnaire. The detailed description of result is mentioned in table 2 and 3.
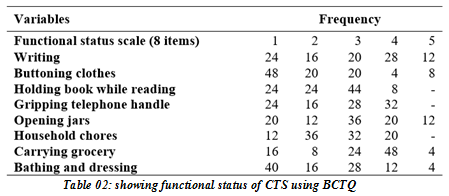
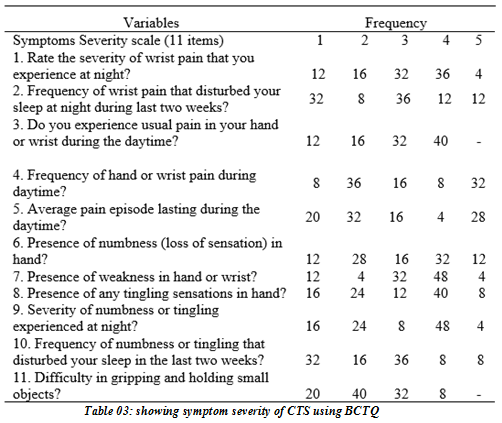
The findings of the functional status in table:2 depicts the difficulty level of the dexterous population where 40% faced difficulty while writing, 32% had difficulty with gripping activities, 32% reported activities like opening jars as troublesome, 52% had difficulty in lifting and carrying jobs while 16% faced difficulty in grooming activities. While on the severity scale depicted in table:3, 40% participants reported having severe pain during the day time, 52% reported hand and wrist weakness, 44% reported numbness, 48% reported tingling, and 52% rated their paresthesia as severe.
Discussion
The results of this study postulated that CTS was found to be 11.06% prevalent in a sample size of 226 dexterous people. Our results are driven from a specific population i-e dexterous which is in contrast to the results obtained by previous studies where the entire population was recruited in the study22. Our findings are similar to Aljunaid et al who reported a prevalence of 13.3% in Saudi dental students23 and Hayder et al who found CTS prevalence of 10.3% in butchers of Pakistan24. Moreover, our study utilized a specialized nerve entrapment test to rule out the population suffering from CTS and then administered the questionnaire to find out the severity that is in opposition to the above mentioned studies. Our findings are in lieu of Tadjerbashi and Harris, that postulated the impact of long term abnormal wrist position in specific occupations25, 26. In our study the participants revealed having abnormal wrist positions and occupational predisposition to the symptoms of CTS. However, our study did not identify the specific positions of wrist that were the cause of CTS, as Ali et al advocated in their study. Moreover, our findings did not include predisposition of this syndrome to a specific occupation contrasting it to the findings of Tadjerbashi et al25. Moreover, our study cannot comment on the argument of Helaly et al where laboratory technicians were considered the occupation most prone to CTS as we did not included them. But, our findings are similar to Hayder et al who reported butchers are equally affected from CTS as are office workers24.
One interesting thing about our research was the fact that professionals who were not having diagnosed CTS had symptoms that were lying in the severe category of Boston Carpal Tunnel Syndrome questionnaire. However, due to less awareness and high job demands attention was not given to the existing symptoms. Thus, considering the recommendations of Demiryurek at al we believe that ergonomical guidance in the exposed dexterous population can lower the risk and severity of this condition27. Moreover, it can also reduce the burden of disease and escalate the quality of life and job satisfaction in this population. However, it should be taken into consideration that high job demands, frequency of the assigned task and demands of the employer can be considered as one of the modifiable risk factors for the development of this syndrome and requires consideration from both the professional and his profession. Nonetheless, these risk factors can be reduced by incorporating the understanding of proper positioning of the wrist of an individual while performing his work, by incorporating breaks in the continuous schedule to reduce the frequency if task, and by adding preventive exercises and stretches to the routine of the professional28. It is also to be considered that not only diagnosed CTS should be treated and taken care of but, people who do not have CTS should also be educated regarding the condition for long term health benefits.
The strengths of our study include using a Standard Questionnaire to estimate the prevalence of CTS. Although the sample size of our study was not large enough to recruit entire dexterous population of Karachi but we collected the data from wide variety of dexterous population. Furthermore, we also performed clinical examination and nerve conduction test (Phalen’s test) to quantify the symptomatic population. Our study also depicted the functional status of dexterous population, both who had CTS and those who did not, and demonstrated the specific complains in this population. Moreover, severity status was also defined in our results. Nonetheless, our study had some limitation too. The sample size of the study was not large enough so we cannot claim these results for the whole dexterous population of Karachi that would have developed the symptoms of CTS. Moreover, there was a lack of awareness about CTS among the population because most of the population was illiterate and refused to take part in our research. There was also reluctance among the population and they were hesitant to provide data.
We recommend that future research should include a large-scale survey and implement clinical trials by administering egronomical modification and evaluate the risk reduction. Considering such high prevalence in a small sample one can predict the immense exposure in entire dexterous population of Karachi and ultimately of Pakistan. Hence, interventional studies are required that imply the treatment and preventive measures among this population. Moreover, awareness campaigns and workshops should be carried out for primary prevention from this syndrome. Along with educating the population on risk, healthcare workers and general population should also be educated on the same.
Conclusion
The results of our study revealed that CTS is a prevalent neuromuscular disorder among dexterous population. The severity level varies among the population. More epidemiological studies are required to get the approximate value to promote ergonomic awareness.
AUTHORS’ CONTRIBUTION:
The following authors have made substantial contributions to the manuscript as under:
Conception or Design: Vrushali Shety
Acquisition, Analysis or Interpretation of Data: Vrushali Shety
Manuscript Writing & Approval: Asma Hamid
All authors acknowledge their accountability for all facets of the research, ensuring that any concerns regarding the accuracy or integrity of the work are duly investigated and resolved.
ACKNOWLEDGEMENTS: We would like to offer our special thanks to all the participants and their families for their support in conducting this research study
INFORMED CONSENT: Written Informed Consent was taken from each patient.
CONFLICT OF INTEREST: The author (s) have no conflict of interest regarding any of the activity perform by PJR
FUNDING STATEMENTS: None declared
ETHICS STATEMENTS: An ethical approval was taken from the ethical review committee of Ziauddin College of Rehabilitation Sciences.
Independence to take part in the review was given to the participants.
The confidentiality of the participants was not penetrated.
Participants were given the right to withdraw from the review whenever required.
All the causations of harm towards the participants of the research were avoided.
Reference
- Janakaran JW. The Prevalence of Carpal Tunnel Syndrome amongst Cashiers in Comparison to Other Cccupations
- nih.gov. 2022. Carpal Tunnel Syndrome Fact Sheet | National Institute of Neurological Disorders and Stroke. [online] Available at: <https://www.ninds.nih.gov/carpal-tunnel-syndrome-fact-sheet> [Accessed 10 September 2022].
- Sevy, J. and Varacallo, M., 2022. Carpal Tunnel Syndrome. [online] Ncbi.nlm.nih.gov. Available at: <https://www.ncbi.nlm.nih.gov/books/NBK448179/> [Accessed 10 September 2022].
- 2022. PubMed. [online] Available at: <https://pubmed.ncbi.nlm.nih.gov/> [Accessed 10 September 2022].
- Bukhari SR, Naz K, Ahmed Z, Rashid A, Ayaz S, Khan AU, Daniyal M, Hussain A, Ans M. Carpal Tunnel Syndrome and Its Prevalence in Pregnant Females of Faisalabad Pakistan. Pak J Med Biol Sci. 2018;2(1):10-9.
- Alhusain FA, Almohrij M, Althukeir F, Alshater A, Alghamdi B, Masuadi E, Basudan A. Prevalence of carpal tunnel syndrome symptoms among dentists working in Riyadh. Annals of Saudi medicine. 2019 Mar;39(2):104-11.
- Puchalski P, Abramczyk U, Dziubiński D, Jedut W, Żyluk A. Localization of paresthesia in patients with carpal tunnel syndrome. Pomeranian Journal of Life Sciences. 2019 Dec 1;65(4):14-6.
- Blanquero J, Cortés-Vega MD, García-Frasquet MÁ, Sánchez-Laulhé PR, Suero-Pineda A. Exercises using a touchscreen tablet application improved functional ability more than an exercise program prescribed on paper in people after surgical carpal tunnel release: a randomised trial. Journal of Physiotherapy. 2019 Apr 1;65(2):81-7.
- Bibi M, Khan B. Carpal Tunnel Syndrome and use of computer keyboard and mouse; a systematic review. Rehman Journal of Health Sciences. 2019 Dec 31;1(2):25-7.
- Genova A, Dix O, Saefan A, Thakur M, Hassan A. Carpal tunnel syndrome: a review of literature. Cureus. 2020 Mar 19;12(3).
- Inbasekaran D, Sankari M, Nambi SG. Prevalence of carpal tunnel syndrome among dentists in Chennai, India. Drug Invention Today. 2018 Nov 2;10(3):3262-5.
- Lorenzen EA. The Anatomy of the Carpal Tunnel and Hand Function of Musicians.
- Feng B, Chen K, Zhu X, Ip WY, Andersen LL, Page P, Wang Y. Prevalence and risk factors of self-reported wrist and hand symptoms and clinically confirmed carpal tunnel syndrome among office workers in China: a cross-sectional study. BMC Public Health. 2021 Dec;21(1):1-0.
- Aslam K, Hussain MM, Arif AB. Prevalence of carpal tunnel syndrome in computer users working in MCB bank of Faisalabad, Pakistan. Rawal Medical Journal. 2019 May 22;44(2):356-.
- Mokhtar ZA. Carpal Tunnel Syndrome and the Impact of Computer Use on Civil Engineering Department Lecturers at Sultan Abdul Halim Mu’adzam Shah Polytechnic. Journal of Technology and Humanities. 2021 Dec 24;2(2):31-6.
- Alzahrani AS, Aljunaid NM, Hegazy AA, Altassan KA. Carpal Tunnel Syndrome and its Occupational Risk Factors among Dental students in their Final Year at King Abdulaziz University, Jeddah, Saudi Arabia. International Journal of Occupational Hygiene. 2021 Dec 30;13(4):Press-.
- Porras V, Orjuela Ramírez ME, Vargas Porras C. Musculoskeletal disorders of the upper and the lumbar region: demographic and occupational characterization, Universidad Nacional de Colombia, Bogotá 2001-2009. Enfermería Global. 2013 Oct;12(4):119-32.
- Kao SY. Carpal tunnel syndrome as an occupational disease. The journal of the American board of family practice. 2003 Nov 1;16(6):533-42.
- Parmar U, Soni K. Effectiveness of Physiotherapy Intervention Along With Ergonomics among Dentists With Carpal Tunnel Syndrome: A Randomized Controlled Trial.
- Pramchoo W, Geater AF, Harris-Adamson C, Tangtrakulwanich B. Ergonomic rubber tapping knife relieves symptoms of carpal tunnel syndrome among rubber tappers. International Journal of Industrial Ergonomics. 2018 Nov 1;68:65-72.
- Multanen J, Ylinen J, Karjalainen T, Kautiainen H, Repo JP, Häkkinen A. Reliability and validity of the Finnish version of The Boston Carpal tunnel questionnaire among surgically treated Carpal Tunnel Syndrome patients. Scandinavian Journal of Surgery. 2020 Dec;109(4):343-50.
- Möllestam K, Englund M, Atroshi I. Association of clinically relevant carpal tunnel syndrome with type of work and level of education: a general-population study. Scientific reports. 2021 Oct 6;11(1):1-6.
- ALJUNAID, N., ALZAHRANI, A., HEGAZY, A. and ALTASSAN, K., 2021. Demographic and Occupational Risk Factors of Carpal Tunnel Syndrome among Dental students in their Final Year at King Abdulaziz University, Jeddah, Saudi Arabia. International Journal of Occupational Hygiene, 13(4).
- Hayder A, Fatimah A, Asghar HM, Maqbool S, Shad M, Zaheer B, Siddiqui O, Hussain A. Prevalence Of Carpal Tunnel Syndrome Among Butchers In Pakistan: Carpel Tunnel Syndrome among Butchers. Pakistan BioMedical Journal. 2022 Jul 31:183-7.
- Tadjerbashi K, Åkesson A, Atroshi I. Incidence of referred carpal tunnel syndrome and carpal tunnel release surgery in the general population: increase over time and regional variations. Journal of Orthopaedic Surgery. 2019 Feb 4;27(1):2309499019825572.
- Harris-Adamson C, Eisen EA, Kapellusch J, Hegmann KT, Thiese MS, Dale AM, Evanoff B, Meyers AR, Bao S, Gerr F, Krause N. Occupational risk factors for work disability following carpal tunnel syndrome: a pooled prospective study. Occupational and Environmental Medicine. 2022 Jan 23.
- Demiryurek BE, Gündoğdu AA. Prevalence of carpal tunnel syndrome and its correlation with pain amongst female hairdressers. International journal of occupational medicine and environmental health. 2018.
- Trillos-Chacón MC, Castillo-M JA, Tolosa-Guzman I, Medina AF, Ballesteros SM. Strategies for the prevention of carpal tunnel syndrome in the workplace: A systematic review. Applied Ergonomics. 2021 May 1;93:103353.
The Ziauddin University is on the list of I4OA, I4OC, and JISC.
This is an open- access article distributed under the terms of the Creative Commons Attribution License (CC BY 4.0).