
Aftab Ahmed Mirza Baig1, Farhan Ishaque2*, Rabia Hassan3, Dr Syed Saeed Qaiser4, Kanwal Banta Ram5, Abid Kamal Ansari6, Rabia Khan7
1Senior Physiotherapist Sindh Institute of Physical Medicine and Rehabilitation, Karachi, Pakistan![]()
2*Assistant Professor, Dow Institute of Physical Medicine and Rehabilitation, Karachi, Pakistan![]()
3 House Officer, Institute of Physical Medicine and Rehabilitation, Dow University of Health Sciences, Karachi, Pakistan![]()
4Assistant Professor, Dow Institute of Physical Medicine and Rehabilitation, Karachi, Pakistan![]()
5Department of Physiotherapy, Dow Institute of Physical Medicine and Rehabilitation, Karachi, Pakistan![]()
6 Vice Principal, Jinnah Post Graduate Medical Centre, JPMC, Karachi, Pakistan![]()
7 Senior Lecturer, Bahria University College of Physical Therapy, Karachi, Pakistan![]()
Abstract
Background and Aim: To evaluate the association of pectoralis minor muscle length and the shoulder range of motion with and without shoulder pain.
Methodology: A sample of 214 participants with and without shoulder pain were enrolled in an analytical cross sectional study at Institute of physical medicine and rehabilitation, Dow University of health sciences, Karachi. Questionnaire was provided to all participants after taking consent. Individuals were categorized into two equal groups i.e. one with and the other without pain). Shoulder active ranges were measured with universal goniometer and pectoralis minor length with measuring tape. Statistical Package of Social Sciences version 21 was used for data analysis. The descriptive variables were assessed for frequencies and percentages. Continuous variables were shown with mean and standard deviations and were correlated with bivariate correlation test. Considered significant was 0.05 p value.
Results: Females were 176(82.2%) and males were 38 (17.8%). Mean ± SD of age, weight, height, and BMI were 26.82 ±7.50, 58.45 ±12.11, 160.59 ± 12.43, and 22.18 ±3.78 respectively. The pain intensity negatively correlated with shoulder range of motions (rs = -0.307 to -0.775, p< 0.05) except medial rotation. Significant difference (p< 0.05) is found for length of pectoralis minor and range of motion between groups. There was also weak positive correlation between pectoralis minor index and shoulder lateral rotation (rs =0.215; p = 0.003).
Conclusion: The shoulder pain affects shoulder joint range of motion and pectoralis minor length. Decreased pectoralis minor muscle length accompanies limited shoulder range of motion except, medial rotation.
Keywords: Physical examination, glenohumeral joint, posture, movement, asymptomatic shoulder, symptomatic shoulder.

Introduction
The shoulder pain is one of the commonest complain among general population. Moreover, along with postural issues, it is the most common work related musculoskeletal disorder1.This joint is less stable and more mobile, anatomically. These characteristics make shoulder to be injured and painful, easily2. Structurally, shoulder is composed of various connective tissues. Shoulder gives connects axial skeleton and the upper extremity and participates for upper extremity movements, primarily. This function of shoulder requires all surrounding structures to be intact3. The lifetime prevalence of pain in shoulder is about 67%2. The literature shows that higher prevalence among females (24.9%) than males (15.4%)4. The occupation of school teachers has 66.7% in China5.The point prevalence of shoulder pain in a systematic review is found to be 10.5% to 28.7%6. Different studies reveals that in the developed societies, the prevalence of shoulder pain is directly proportional to age7,8. And is most significantly increase in between 50-56 years4. The upper body bad postures, such as rounded shoulder, forward headed, poke chin and slouched posture have been suggested as the possible predisposing factors when there is no specific. These are suggested in pathogenesis of many clinical conditions which involve the shoulder5,9. Shortened pectoralis minor muscle (PMM) and abnormal posture are supposed to participate to stimulate pain and to decrease normal daily activities of upper quadrant of the body9. Furthermore, any alteration in the structures that forms the shoulder joint can results in scapular dyskinesis which is defined as the abnormality of the scapula posture or movements10.
The physical examination of surrounding structures is an important element to evaluate any shoulder problem3.The physical examination of shoulder comprises objective findings of range of motion (ROM) and length of soft tissues to identify impairments causing pain. The length of PMM can be one of the causes to affect the normal scapular function. So, this fact also suggests, its association with the shoulder pain11. Kinematics alteration and the asymmetrical changes in the shoulder joint have been widely reported among both the symptomatic and asymptomatic individuals. There are various findings on the relationship between the PMM length (PMML) and the shoulder kinematics12 but as far as the authors knowledge there are still some specific limitations left with regards this issue. So, this study purpose is to assess the significant statistical association between PMML and shoulder ROM among the participants with and without shoulder pain.
Methodology
The study design was analytical cross sectional. Participants were recruited with convenient sampling technique at Institutes of physical and medical rehabilitation, Dow University of health sciences, Karachi. However, duration of study was from August to October, 2019. The institutional review was taken from the same institute. Sample of 214 participants with and without shoulder pain were included in the study. This sample size was extracted from degree of external rotation in pain (101.94±13.45) and without pain (107.06±13.26) of previous literature13 along with confidence interval of 95%, margin of error of 5% and power 80% through open epi. Inclusion criteria were age range between 20 – 50 years with ability to do no less than 90 degree of arm elevation. Individual having at least one week onset of symptoms were included for group of individuals with pain. Exclusion criteria comprised participants with BMI >28 kg/m2 to avoid error during palpitations, pregnancy, ligamentous hyper laxity of gleno-humeral with presence of sulcus sign, shoulder apprehension test and shoulder anterior drawer test. The individuals having history of adhesive capsulitis, any systemic illnesses, any shoulder trauma and surgery, any neurological condition (cervical radiculopathy), individuals taking any immunosuppressive medicine were also excluded11. A screening Performa was used to screen exclusion criteria. The investigators screened and provided self-designed questionnaire to all study participants after taking consent. Each of the participants willingly participated and was allowed to refuse further participation at any time. The questionnaire comprised demographics (gender, level of education and marital status), question regarding presence of shoulder pain within last 3 months. Participants were asked to rate their intensity pain after responding ‘yes’ to presence of pain. The PMM was measured with measuring tape and pectoralis minor index (PMI) test was used to assess the PMT11. However, the universal goniometer (UG) with long-arm was used to assess active ROM (AROM) of shoulder joint3. PMML was measured for symptomatic side in the group with pain. However, side for this measurement was selected randomly in the group without pain11. All the data was collected within constraints. Privacy of participants was considered. Data was entered and analysed through SPSS version 21. The descriptive variables like gender were reported through frequencies and percentages. The continuous data like age, height, weight, BMI, Shoulder ROMs, PMML and PMI was calculated for mean and standard deviations. Shapiro-wilk test was used to identify normality. The value for shapiro-wilk test for asymptomatic individuals showed 0.001 and for symptomatic individuals’ 0.000 i.e. less than the value (0.01) so that the data was non symmetrical, so spearman’s test was used for correlation of continuous outcome data. The Mann Witney U test was also employed to compare variables of two groups symptomatic and asymptomatic. The considered significant p-value was less than 0.05.
Pectoralis minor muscle length measurement
Position of participant was sitting. Assessor marked after palpation of inferior part of the medial border of the coracoid process and inferior edge of the fourth rib at the sternum. Centimeter measuring tape was used to measure distance between these two points14,15. Mean value of three times measurements was recorded15. The mean PMML for each individual was divided by height of the same individual and then multiplied by 100 in order to calculate the PMI. The suggested range of PMI refers short PMM when it is 7.65 or lower9,15.
Shoulder joint range of motion measurement
The individual was in upright sitting position on a high back chair. The fulcrum of UG was placed at inferior and lateral to the acromion process, the stable arm was placed parallel to the trunk and the moving arm parallel to the long axis of the humerus16,11. Then investigator assessed abduction in the same position, with active elevation of arm in coronal plane and the fulcrum of goniometer was placed at the midpoint of the posterior aspect of the glenohumeral joint with placing the stable and moving arm as same as for active flexion ROM16. Then the two movements external and internal rotation were assessed by the investigator in supine position with both hips and knees flexed in 45 degrees. Upper limb was in supported position with 90 degrees’ abduction with 90 degrees’ elbow flexion and neutral wrist. After this, the individual was asked to rotate their arm again in external rotation, and internal rotation maintaining the 90 degree abducted position to their end range without feeling of discomfort. After end range, stable arm and movable arm of goniometer was placed parallel to the floor and forearm respectively. 16,11 All ranges in degrees were recorded.
Ethical Concerns
All the data was collected under ethical constraints. After institutional approval from same institute the informed consent was taken from all participants before commencement of study. The study followed the declaration of Helsinki.
Results
Out of 214 participants, majority were females (table 1). The demographical data is shown in table 1. The mean age, height, weight and BMI were 26.82 +7.50, 160.59 + 12.43, 58.45 +12.11and 22.18 +3.78, respectively. The mean NPRS of symptomatic individuals were 3.4±1.5. About 73(68.2%) of symptomatic individuals had right side shoulder pain and 34(31.8%) had left side shoulder pain. However, table 2 shows the calculated mean and SD of shoulder range of motions, PMI and PML.
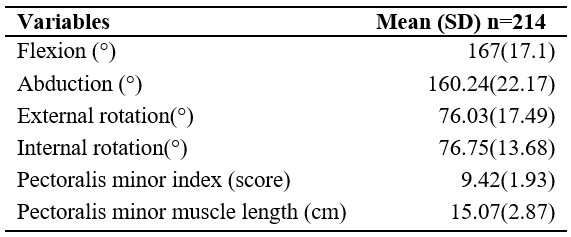
Table 1; Demographical data of all participants:
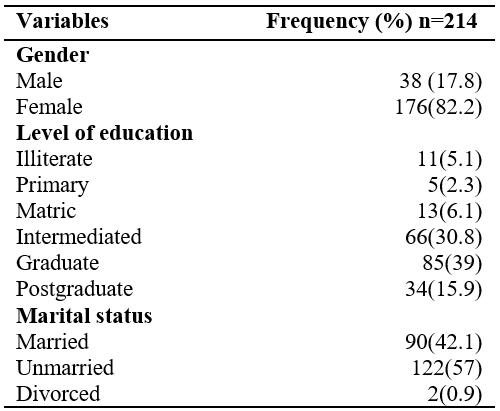
Table 2; Mean and SD of shoulder range of motion and pectoralis minor index and length
The table 3 manifests the significant difference (p-value < 0.05) of all variables between groups with and without shoulder pain. Shows the significant difference (p< 0.05) of all variables between groups with and without shoulder pain.
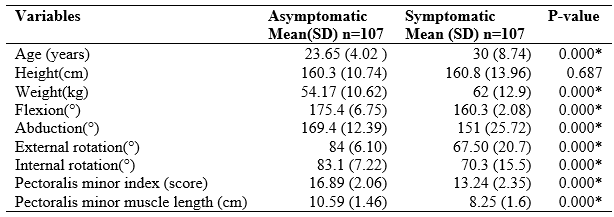
* (p< 0.05 is considered significant)
Table 3; Difference of variables between groups
* (p< 0.05 is considered significant)
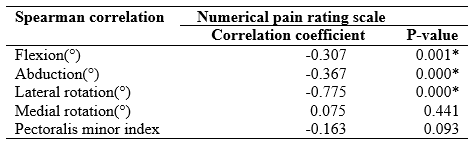
Table 4; Relationship of Numerical pain rating scale with different variables among individuals with shoulder pain
The spearman correlation showed significant weak positive correlation between PMI and degree of shoulder active lateral rotation (rs =0.215; p = 0.003) only among all participants. Whereas the spearman correlation showed moderate negative correlation of NPRS with flexion, abduction and lateral rotation of shoulder among symptomatic group in table 4.
Outcome Measures
The outcome measures used in this study were centimeter measuring tape to measure the length of pectoralis minor muscle and the universal goniometer used to assess the active ROM of the shoulder joint.
Discussion
This study evaluated the relationship of PMML and the ROM of the shoulder among individuals with and without shoulder pain. Findings suggest weak positively correlation of PMM and shoulder lateral rotation among all individuals. The symptomatic group showed decreased PMML and shoulder ROM with significant difference between both groups. However, intensity of pain moderate negatively correlated with shoulder flexion, abduction and lateral rotation.
The measurement of shoulder ROM and muscle length has been remain a critical feature of a clinician’s evaluation.17,18 The goniometry for shoulder AROM and measuring tape test to measure the length of PMML has been shown good intra- and interrater reliability along with between-day reliability for PMML among individuals with and without shoulder pain through the previous studies14,17,18. The current study included the same clinical test and outcome tools for better outcome results among individuals with and without shoulder pain. The length of PMM is assumed to be one of the potential biomechanical factor that associates with altered shoulder movement during daily activities13,18. A cross sectional study was held to evaluate association between PMM resting length and external rotation ROM of shoulder joint in participants with and without shoulder pain. The study was conducted among 50 adult individuals. Findings suggested PMML is not correlated with external rotation ROM of shoulder joint in individuals with and without shoulder pain11. The current study showed contrary results suggesting positive association of PMM resting length and external rotation ROM of shoulder joint. However, sample size of current study included 214 individuals with and without shoulder pain of same age group as previous study11, comprising for females.
The direct and indirect relationship of PMML with shoulder pain is questionable and different mechanism are needed to be identified18,19,20. Previous cross sectional study was held amidst 54 individuals with shoulder pain and 54 without shoulder pain. The results suggest PM resting length is associated with shoulder pain21. Current study follows that study with larger sample size as it found significant difference in PM resting length between groups of shoulder pain and without shoulder pain suggesting its association with shoulder pain22,23. Another cross sectional study was done to evaluate relationship between the scapular upward rotations and the pectoralis minor and levator scapulae muscle lengths among 54 participants with the chronic shoulder pain. It was found that there is small correlation between the shoulder pain and the pectoralis minor and the levator scapulae lengths. The strong association was also found between the pectoralis minor muscle and the levator scapulae lengths24 However, in comparison to this study the current study used a large sample size and a significant difference is found in the pectoralis minor muscle resting length between the two groups of with and without shoulder pain which suggests the pectoralis minor muscle length association with the shoulder pain.
Shoulder pain and ROM has also point of discussion22. A cross sectional study was done on 35 individuals in order to evaluate the association between the pectoralis minor muscle tightness and cervical ROM and strength in car drivers. The findings of that study suggests that the cervical lateral flexion also showed positive correlation with the contralateral pectoralis minor muscle tightness25. But in this study we were only concerned with the association of pectoralis minor muscle tightness and the shoulder range of motion and found moderate negatively correlated with shoulder flexion, abduction and lateral rotation. Current study provides results related to shoulder ROM. Another cross sectional study of 64 participants in Saudi Arabia found good negative correlation of the shoulder flexion, abduction, and rotation ROM with NPRS.22 however, the current study showed moderate negative correlation same outcome tools but there was no larger symptomatic sample.
The study limitations include the choice of convenient sampling technique but there was larger sample size with reliable and standard outcome tools. There could be error in manual examination but three times reading average was taken to avoid those errors.
Conclusion
The study results suggested that shoulder joint ROM and PMML is affected with shoulder pain. The change in length of PMM affects shoulder range of motions except, medial rotation. Furthermore, increase in intensity of pain accompanies decrease in shoulder ROMs.
AUTHORS’ CONTRIBUTION:
The following authors have made substantial contributions to the manuscript as under:
Conception or Design: Aftab Ahmed Mirza Baig, Farhan Ishaque, Rabia Hassan
Acquisition, Analysis or Interpretation of Data: Dr Syed Saeed Qaiser , Kanwal Banta Ram, Abid Kamal Ansari
Manuscript Writing & Approval: Rabia Khan
All authors acknowledge their accountability for all facets of the research, ensuring that any concerns regarding the accuracy or integrity of the work are duly investigated and resolved.
ACKNOWLEDGEMENTS: We thanks all the participants in this study.
INFORMED CONSENT: Written Informed Consent was taken from each patient.
CONFLICT OF INTEREST: The author (s) have no conflict of interest regarding any of the activity perform by PJR.
FUNDING STATEMENTS: None declared
ETHICS STATEMENTS: The study has been approved by from the Ethics Committee of Dow Institute of Physical Medicine And Rehabilitation, Karachi.
References
- Saleem M, Tanveer F, Ahmad A, Gilani SA. Correlation between shoulder pain and functional disability. Rawal Medical Journal. 2018 ;43(3):483-85.
- Ackerman IN, Page RS, Fotis K, Schoch P, Broughton N, Brennan-Olsen SL, Bucknill A, Cross E. Exploring the personal burden of shoulder pain among younger people in Australia: protocol for a multicentre cohort study. BMJ open. 2018;8(7):1-7.
- Bakhsh W, Nicandri G. Anatomy and Physical Examination of the Shoulder. Sports Med Arthrosc Rev. 2018;26(3):10-22.
- Zacchilli MA, Owens BD. Epidemiology of shoulder dislocations presenting to emergency departments in the United States. JBJS. 2010;92(3):542-49.
- Temesgen MH, Belay GJ, Gelaw AY, Janakiraman B, Animut Y. Burden of shoulder and/neck pain among school teachers in Ethiopia. BMC Musculoskelet Disord. 2019;20(1):18-26.
- Chung JW, So HC, Yan V, Kwok PS, Wong BY, Yang JY, Chan AP. A Survey of Work-Related Pain Prevalence Among Construction Workers in Hong Kong: A Case-Control Study. Int J Environ Res Public Health. 2019 ;16(8):1404-16.
- Vincent K, Leboeuf-Yde C, Gagey O. Are degenerative rotator cuff disorders a cause of shoulder pain? Comparison of prevalence of degenerative rotator cuff disease to prevalence of nontraumatic shoulder pain through three systematic and critical reviews. J Shoulder Elbow Surg. 2017 ;26(5):766-73.
- Guzowski K, Stolarczyk A, Czyrny Z, Dębek A, Kranc B. Assessment of ultrasonography as a diagnostic tool in shoulder pain and alterations in glenohumeral range of motion in tennis players. Videosurg Other Miniinvasive Tech. 2019 ;14(1):114-25.
- Singla D, Veqar Z. Association between forward head, rounded shoulders, and increased thoracic kyphosis: a review of the literature. J Chiropr Med. 2017 ;16(3):220-29.
- Lefevre-Colau MM, Nguyen C, Palazzo C, Srour F, Paris G, Vuillemin V, Poiraudeau S, Roby-Brami A, Roren A. Kinematic patterns in normal and degenerative shoulders. Part II: Review of 3-D scapular kinematic patterns in patients with shoulder pain, and clinical implications. Ann Phys Rehabil Med. 2018 ;61(1):46-53.
- Rosa DP, Santos RV, Gava V, Borstad JD, Camargo PR. Shoulder external rotation range of motion and pectoralis minor length in individuals with and without shoulder pain. Physiother Theory Pract. 2019 ;35(10):986-94.
- Turgut E, Baltaci G. Effect of flexibility deficit on scapular asymmetry in individuals with and without shoulder pain. Braz J Phys Ther. 2018 ;22(5):370-75.
- Morais N, Cruz J. The pectoralis minor muscle and shoulder movement-related impairments and pain: Rationale, assessment and management. Phys Ther Sport. 2016; 17:1-3.
- Rosa DP, Borstad JD, Pires ED, Camargo PR. Reliability of measuring pectoralis minor muscle resting length in subjects with and without signs of shoulder impingement. Braz J Phys Ther. 2016 ;20(2):176-83.
- Kolber MJ, Hanney WJ. The reliability and concurrent validity of shoulder mobility measurements using a digital inclinometer and goniometer: a technical report. Int J Sports Phys Ther. 2012; 7(3): 306-13.
- Correll S, Field J, Hutchinson H, Mickevicius G, Fitzsimmons A, Smoot B. Reliability and Validity of the Halo Digital Goniometer for Shoulder Range of Motion in Healthy Subjects. Int J Sports Phys Ther. 2018;13(4):707-14.
- Fieseler G, Laudner KG, Irlenbusch L, Meyer H, Schulze S, Delank KS, Hermassi S, Bartels T, Schwesig R. Inter-and intrarater reliability of goniometry and hand held dynamometry for patients with subacromial impingement syndrome. J Exerc Rehabi. 2017 ;13(6):719-26.
- Finley M, Goodstadt N, Soler D, Somerville K, Friedman Z, Ebaugh D. Reliability and validity of active and passive pectoralis minor muscle length measures. Braz J Phys Ther. 2017 ;21(3):212-18.
- Rosa DP, Borstad JD, Pogetti LS, Camargo PR. Effects of a stretching protocol for the pectoralis minor on muscle length, function, and scapular kinematics in individuals with and without shoulder pain. J Hand Ther. 2017 ;30(1):20-29.
- Lin DJ, Wong TT, Kazam JK. Shoulder injuries in the overhead-throwing athlete: epidemiology, mechanisms of injury, and imaging findings. Radiol. 2018; 286(2):370-87.
- Navarro-Ledesma S, Fernandez-Sanchez M, Luque-Suarez A. Does the pectoralis minor length influence acromiohumeral distance, shoulder pain-function, and range of movement? Phys Ther Sport. 2018; 34:43-48.
- Anwer S, Alghadir AH, Al-Eisa ES, Iqbal ZA. The relationships between shoulder pain, range of motion, and disability in patients with shoulder dysfunction. J Back Musculoskelet Rehabil. 2018 ;31(1):163-67.
- Pourahmadi MR, Takamjani IE, Jaberzadeh S, Sarrafzadeh J, Sanjari MA, Bagheri R, Jannati E. Test-retest reliability of sit-to-stand and stand-to-sit analysis in people with and without chronic non-specific low back pain. Musculoskelet Sci Pract. 2018;35: 95-104.
- Navarro-Ledesma S, Fernandez-Sanchez M, Struyf F, Suarez AL. Association of Both Scapular Upward Rotation and Scapulothoracic Muscle Lengths With Shoulder Pain, Function, and Range of Movement. Journal of Manipulative and Physiological Therapeutics. 2020 Oct 1;43(8):824-31.
- Sikka S, Sasidharan A. Association of cervical range of and pectoralis minor tightness i. 2020.
The Ziauddin University is on the list of I4OA, I4OC, and JISC.
This is an open- access article distributed under the terms of the Creative Commons Attribution License (CC BY 4.0).